Relationship Between Baseline and Longitudinal Self-Reported Physical Function and Cardiorenal Outcomes in CKD: Findings From the CRIC Study
@shlipak_khrc@NavTangri @markunruh_01@JonTaliercio_DO @ManjulaKTamura@SarahJSchrauben
https://t.co/VXn5OPPUD0
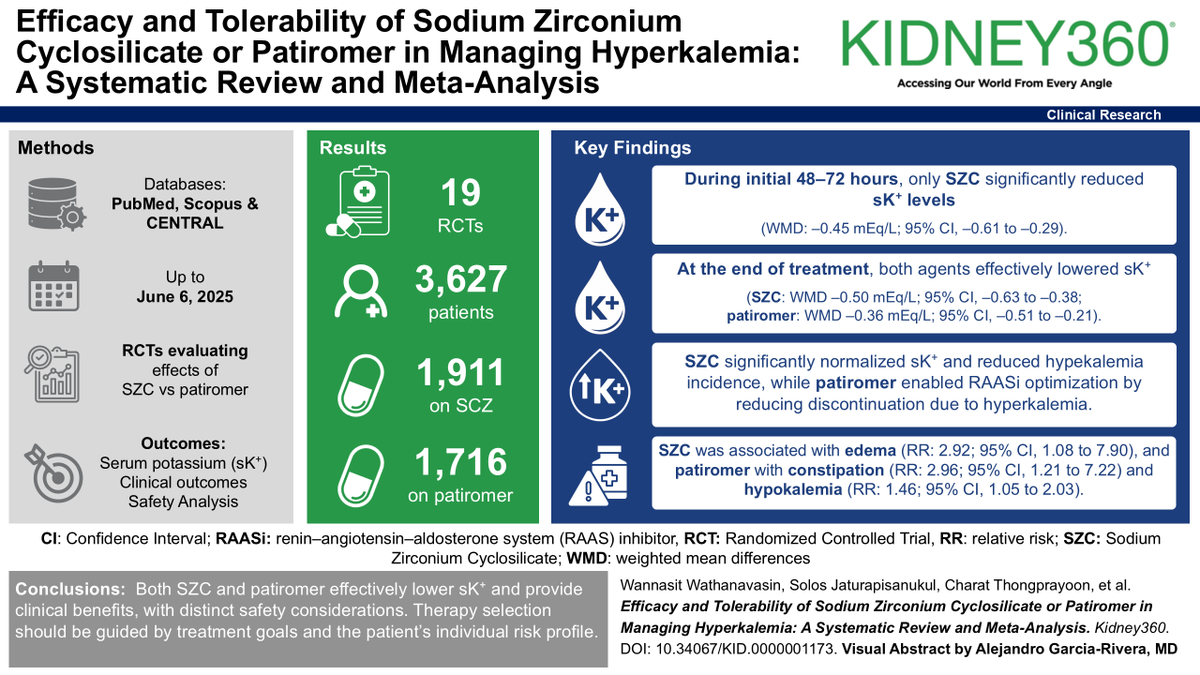
Which is a better treatment for people with hyperkalemia: sodium zirconium cyclosilicate (SZC) or patiromer? That depends. Find out why in the #ASNKidney360 study. https://t.co/RYsFq2uuZD
🩸 Bleeding on anticoagulation is NOT a complication… it’s a turning point
⚠️ The problem
We prescribe anticoagulants to prevent:
👉 Stroke
👉 MI
👉 VTE
But the most frequent complication is:
👉 Bleeding
And here’s the uncomfortable truth:
> Bleeding often determines prognosis more than thrombosis
🧠 Why this matters
Bleeding is NOT just an event.
It triggers:
❌ Treatment interruption
❌ Fear-driven underdosing
❌ Permanent discontinuation
👉 Leading to ↑ stroke, ↑ MI, ↑ mortality
🔥 Key clinical reality
📊 Major bleeding:
~1-3% per year
30-day mortality >15%
1-year mortality >25%
👉 That’s NOT benign
⚖️ The real battlefield
Every anticoagulated patient lives here:
👉 Thrombosis vs Bleeding
And we often focus on only one side.
🧠 What experts are telling us (ESC)
This is the new paradigm 👇
1️⃣ Risk is dynamic
Bleeding risk is highest:
👉 Early after starting anticoagulation
👉 In elderly / multimorbid patients
👉 Reassess continuously, not once
2️⃣ Not all bleeding is equal
🚨 Critical sites = high mortality:
Intracranial
GI
Retroperitoneal
Pericardial
👉 Even small volumes can kill
3️⃣ Combination therapy is dangerous
👉 OAC + antiplatelet = 2–3× ↑ bleeding
✔️ De-escalate EARLY
✔️ Avoid triple therapy when possible
4️⃣ Prevention is powerful
Simple interventions:
✔️ PPI for GI protection
✔️ Avoid NSAIDs / SSRIs when possible
✔️ Correct dosing (DOAC underdosing = worse outcomes)
👉 Most bleeding is preventable
🚨 When bleeding happens
Think in 3 steps:
🩸 1. Stabilize
Stop anticoagulant
Airway, oxygen, access
Fluids + transfusion
🧪 2. Reverse (if needed)
VKA → PCC + Vitamin K
Dabigatran → Idarucizumab
FXa inhibitors → PCC (± Andexanet)
🔎 3. Find and control the source
Endoscopy
IR embolization
Surgery
⚠️ The biggest mistake
> “Let’s stop anticoagulation and never restart”
🧠 The evidence says:
👉 NOT restarting = ↑ stroke + ↑ death
✔️ Restart early when safe
✔️ Individualize timing + dose
🔄 The future
We are moving toward:
👉 Personalized anticoagulation
👉 Dose tailoring
👉 Drug selection based on bleeding profile
🎯 Take-home message
Anticoagulation is NOT binary.
It is:
👉 A continuous balance
👉 A dynamic decision
👉 A personalized therapy
🤓 Final thought
> The goal is not to avoid bleeding
The goal is to survive both bleeding AND thrombosis
📚 Reference
Galli, M., Simeone, B., ten Berg, J., et al. (2026). European Heart Journal: Acute Cardiovascular Care.
https://t.co/dovWgN9BEu
Current and Future Therapeutics for Focal Segmental Glomerular Sclerosis in the Era of Precision Medicine: A Review
https://t.co/RkHblc7Bg6 (OPEN ACCESS)
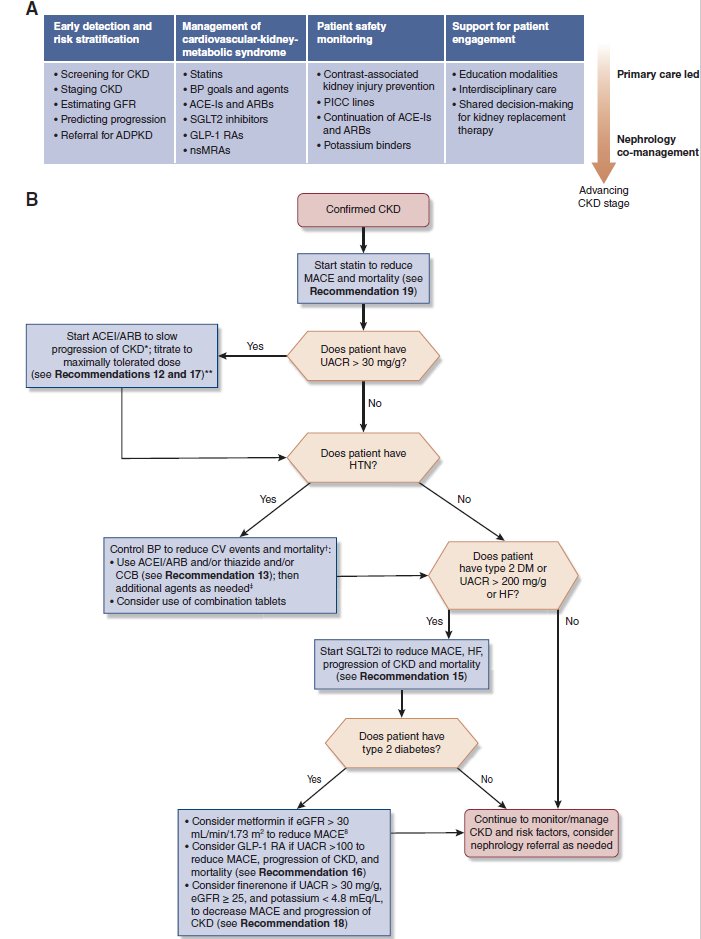
The dramatic expansion in CKD therapeutics to prevent progression of kidney disease and reduce cardiovascular events calls for thoughtful implementation. The 2025 guidelines synthesize new evidence for Primary Care Management of CKD in this #ASNCJASN#perspective https://t.co/6yj0GWECfy
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
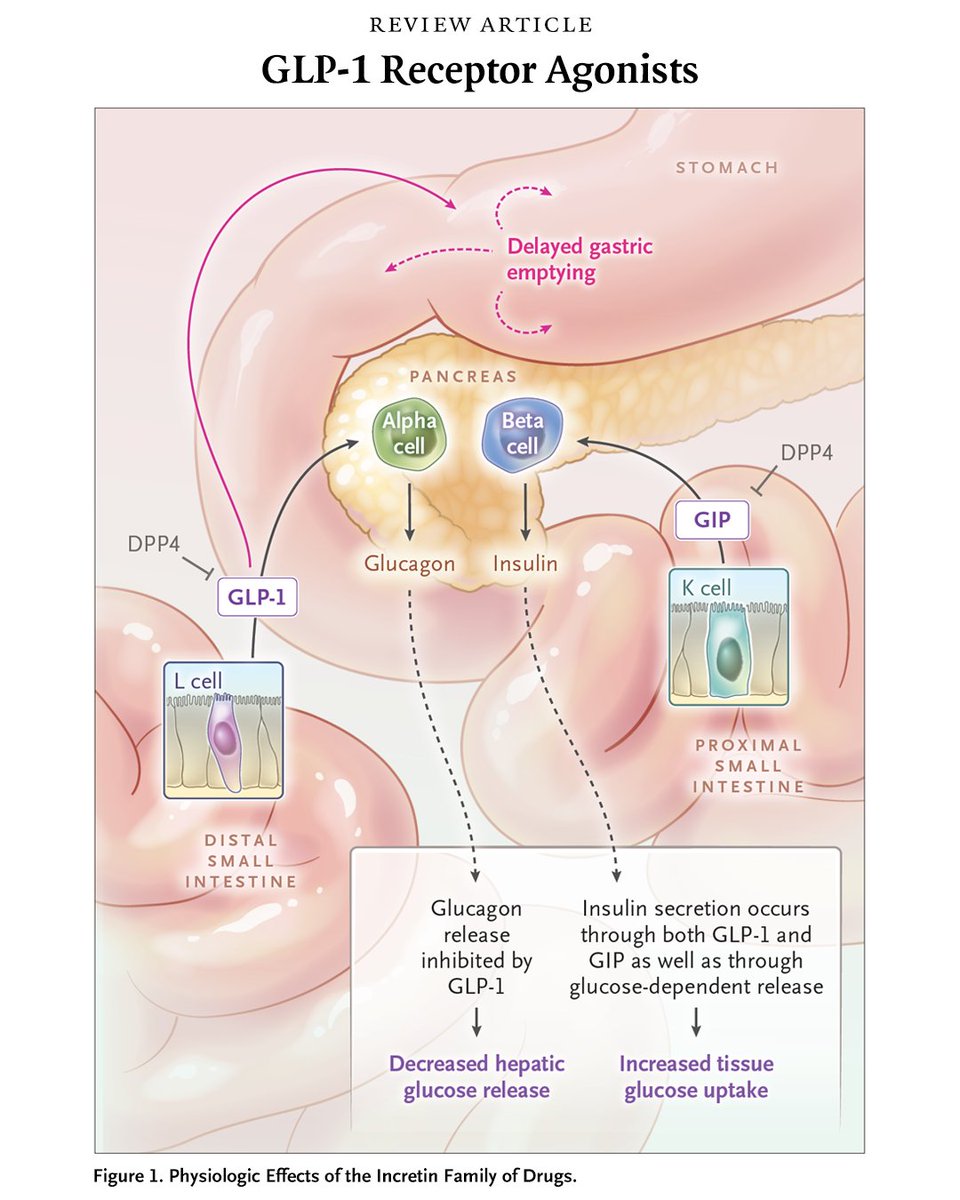
GLP-1 receptor agonists are increasingly used to treat type 2 diabetes and obesity, and trials have shown reductions in cardiovascular risk and slowing of kidney failure. Adverse events are mostly gastrointestinal.
Read the Review Article “GLP-1 Receptor Agonists” by Clifford J. Rosen, MD, and Julie R. Ingelfinger, MD, from @tuftsmedschool and the Maine Medical Center Institute for Research: https://t.co/D0XSLv7U8n
When eGFR drops after initiating treatment with empagliflozin or finerenone, we often stop these treatments. This is less likely to happen when eGFR is already low. The initial eGFR drop associates w/ diuretic use. Back off on the diuretics, not the disease modifying therapies.