Beyond brain fog: viral proteins as convergent drivers of neuroinflammation and proteinopathy
🚨“COVID-19 never really leaves your brain.”
New science review proposes SARSCoV2 viral proteins stay behind as long-lived toxins, triggering chronic neuroinflammation and planting the seeds of Alzheimer’s and Parkinson’s, even after mild infection.
This very interesting and eye-catching GERMAN review reframes post-viral neurological syndromes( L0ngC0vid) as driven by persistent viral proteins acting as long-term toxins ("protein-as-pathogen" model), not just the active infection!
➡���Core mechanisms:
- SARSCoV2 Spike and OTHER viral proteins activate glial TLR4/TLR2 receptors, triggering chronic neuroinflammatory cascades via NLRP3 inflammasome,
- They also disrupt autophagy, allowing toxic protein aggregates (tau, amyloid-beta, α-synuclein) to accumulate and seed neurodegeneration,
➡️SARSCoV2 specific evidence:
- Animal studies show Spike protein alone (without live virus) induces TLR4-mediated cognitive deficits, memory impairment, synaptic loss, and sustained neuroinflammation, recapitulating post-COVID syndrome,
- Spike binds α-synuclein, accelerating Parkinson-like clumps,
➡️Human data evidence:
- Millions experience "brain fog,"
- Post-COVID patients exhibit measurable brain damage: cortical thinning, hippocampal iron accumulation, and biomarkers of ongoing neuronal injury,
➡️Broader risks:
- Even mild infections leave lingering proteins that promote Alzheimer’s and Parkinson’s-like pathology via shared pathways,
- Same pathways seen in influenza, dengue, West Nile etc,
- Mild infection = no protection,
‼️So, according to this review, the “protein-as-pathogen” model makes it crystal clear: every new SARSCoV2 infection (even mild or asymptomatic) deposits more of these long-lived toxic viral proteins into the brain. They don’t fully clear. They accumulate.
Each reinfection reloads the TLR4/TLR2 → NLRP3 inflammasome trigger and further collapses autophagy, speeding up the tau/amyloid/α-synuclein proteinopathy and neurodegeneration.
SARS-CoV-2 does not just infect.
It weaponizes its own proteins as long-lived intracellular saboteurs.
Millions are probably already carrying this hidden payload.
This is not brain fog.
This is a silent, population-scale reprogramming of human brains toward dementia-like decline.
The long-term neurological cost will probably dwarf the acute pandemic itself!
#AvoidSars2 #AvoidReinfections
https://t.co/x0oxacaNwl
And the pattern is not random.
The affected systems - orbitofrontal cortex, limbic-related pathways, thalamocortical networks - are exactly the systems you would suspect in a condition involving fatigue, attention deficits, sleep disturbance, sensory dysregulation, anxiety or altered motivation.
This is why brain fog is such a weak term.
Fog sounds vague.
What similar studies are pointing to is much more concrete.
Fronto-limbic circuits,
white-matter pathways,
thalamocortical connectivity,
network-level reorganization.
That is not fog.
That is altered brain network biology.
Does the brain always return to baseline after COVID?
A new multimodal MRI study suggests the answer may be - not always.
After infection, some brains may remain in a different network state - and we still do not know if that state is temporary, compensatory, or maladaptive🧵
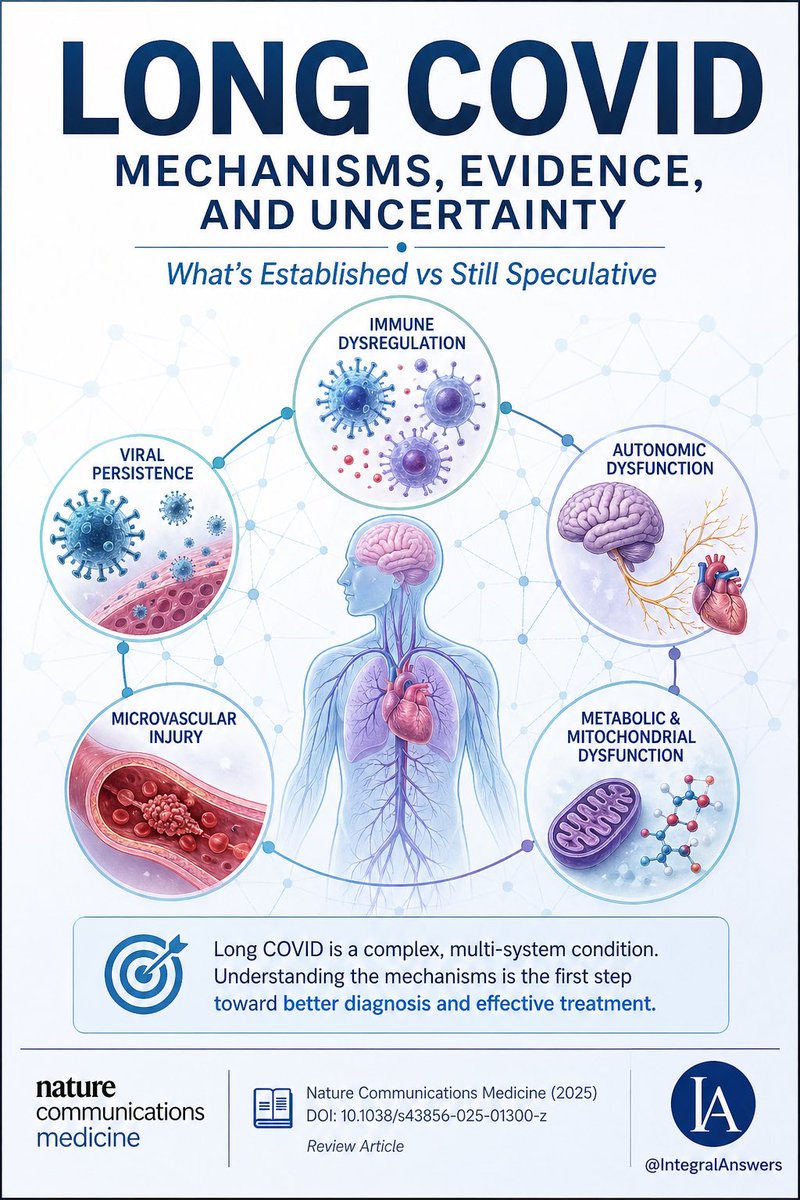
1/ Long COVID is one of the most complex post-infectious syndromes ever studied.
A new review in Nature Communications Medicine attempts to unify the biology.
Here’s what’s established, what’s emerging, and what’s still speculative. 🧵
Identifying an inflection point for Alzheimer's disease from the brains of 80 and 100 year old individuals. Microglia transition is key; initially it is protective vs inflammatory changes triggered by amyloid.
But microglia can turn destructive linked to tau. Resilience in older age, via two divergent pathways, prevents that transition. @NatureMedicine
https://t.co/cyiHYetCVt
We must be crystal clear about a few points. Long Covid is not a "poorly understood neuroimmune disorder" with no biomarkers. It is a widely studied biological medical condition. Pathology spanning basically all body systems is well documented, with damage in situ across organs
Almost one year after SARS2 infection, children with Long COVID showed measurable changes in the tiny blood vessels of the retina.
Wider arterioles.
Wider venules.
A shifted arteriole-to-venule ratio.
This was not just a symptom survey.
It was an objective microvascular signal🧵
I’m a member of the “Die Faster” LongCovid group, as I’ve been on Medicaid since COVID disabled me in 2020. I will never access MABs, I will never access cutting edge therapies, & I will never get care. I’m alive by luck. Millions of us are living like this. This is a Class War.
Said Dr. Mark Painter in a recent episode of PolyBio’s Lab Visits: “What we’re seeing in a third of people with Long COVID, maybe more, is evidence that T cells recognizing either SARS-CoV-2—or in some different people, herpesviruses—are persistently activated. Which is suggestive that those viruses are present somewhere in the body.”
Listen to the full interview here: https://t.co/g3CnbSqNsl
The study shows that infection may shift the population toward a higher degree of low-level cardiac injury. Clinically, this may be subtle. At the population level, it may matter.
💊‼️Long COVID could be, at least in some patients, an autoimmune disease occurring alongside chronic infection, antigenic persistence, or viral reactivations.
Okay.
So now what?
Are there treatments?
Can autoantibodies be removed?
Can this autoimmunity be “switched off”?
Are we close to a cure?
The honest answer is this: we are not facing an immediate cure , although possibly a future one, but we are facing a huge shift in how we think about the disease.
Because if part of Long COVID, and possibly also ME/CFS, has an autoimmune basis, then it would no longer make sense to treat it as a diffuse syndrome with no therapeutic direction. We would need to do the same thing we do in other autoimmune diseases: classify patients properly, identify biomarkers, and design a stepwise treatment approach.
Not all patients would have the same mechanism.
Not all patients would respond in the same way.
And not all patients would need the same level of treatment.
But for the first time, a more logical therapeutic map is starting to emerge.
A clearer logic is beginning to appear: identify which patients have a real autoimmune component and, from there, think about which therapies could make sense.
At present, what is accessible would not be a cure, but treatments already known from other autoimmune diseases that could help reduce autoantibody activity, modulate the immune response, or decrease part of the immunological damage.
In the best-case scenario, these would be treatments to improve, stabilize, or reduce autoimmunity. Not to completely “erase” the disease.
If I had to rank the options in an orientative way, thinking about potential usefulness and safety profile, I would do it like this:
1. IVIG
The most reasonable short-term option would probably be IVIG, meaning intravenous immunoglobulin.
IVIG does not directly eliminate all autoantibodies as such, but it can modulate the immune system, compete with pathogenic autoantibodies, block part of the inflammation, and dampen the immunological attack without requiring such intense immunosuppression.
In many autoimmune diseases, it is used precisely because of this immunomodulatory effect. Among this type of therapy, it is probably one of the options with the best balance between potential usefulness and safety profile.
That said, it is not free of side effects, it is expensive, and access is limited.
2. FcRn inhibitors
Next, I would place FcRn inhibitors.
These drugs are very interesting because they reduce the total amount of circulating IgG and, with it, they can also reduce the burden of pathogenic autoantibodies.
The advantage is that they are quite targeted toward the humoral component of autoimmunity, meaning the antibody-mediated part.
The disadvantage is that they are not yet truly established for Long COVID or ME/CFS, and it would still be necessary to demonstrate very clearly which subgroup of patients would benefit the most.
Even so, conceptually, if we are talking about an autoantibody-mediated disease, this is one of the most promising strategies.
3. Immunoadsorption
At the next level, I would place immunoadsorption.
This technique consists of filtering the blood to remove immunoglobulins, especially those that may be participating in the autoimmune process.
It is a more targeted strategy than systemic immunosuppression and, in diseases mediated by autoantibodies, it can make a lot of sense.
Its main limitation is logistical: it is not a simple therapy, it requires specialized centers, and its effects may not last if the immune system continues producing the same autoantibodies afterwards.
(1/3)
🔵Continued in the next post.👇🏻
The societal response to covid and moral injury - some thoughts 🧵
Non-cc people are often of the belief that my greatest moral injury related to covid is the injustice of letting vulnerable people “fall by the wayside”.
1/6
🔵 If we translate this to Long COVID and other post-infectious syndromes, it is actually not new.
What this study shows is that, after COVID-19, the risk of developing several allergic/atopic conditions increases during the following 18 months, both in children and in adults.
But the underlying immunological logic is not exclusive to SARS-CoV-2.
This can happen after many infections, because one of the first cells to become activated in mucosae and barrier tissues are mast cells. They are sentinel cells, very fast to respond, and they quickly participate in recruiting the rest of the leukocytes. That is why, during and after many infections, a phase of mast cell activation, mucosal inflammation, and poorer tolerance to external stimuli can appear.
The difference is that, when the pathogen is effectively cleared and the inflammation resolves, this response usually decreases progressively over the months after infection.
The problem is when the antigen, the inflammation, or the immune dysregulation persists. That is where we can apply this same logic to Long COVID and to other post-infectious syndromes: if antigens persist or sustained inflammation/autoimmunity remains, mast cells can also remain chronically activated.
And from there, the consequence is not just “more histamine.”
There may also be:
-persistent mucosal inflammation
-worse tolerance to allergens, foods, and chemicals
-epithelial barrier disruption, allowing more things to pass through than they should and further amplifying the problem
-and potentially a more Th2-skewed inflammatory environment, recruiting eosinophils, basophils, and mast cells, and in some patients even promoting further IgE production
So the point is that this may go beyond simple mast-cell-driven “histaminosis.” In some patients, chronic mucosal inflammation and mast cell activation could also help promote a more stable allergic/atopic phenotype.
In other words, the sequence would be something like this:
infection / mucosal inflammation
→ mast cell activation
→ if the pathogen is cleared and the immune response resolves, activation gradually decreases over time
But if there is:
-persistent antigen / chronic inflammation / autoimmunity / sustained immune dysregulation
-chronic mast cell activation
- worse immune tolerance and more allergic/atopic phenotypes
Impact of SARS-CoV-2 infection on subclinical myocardial injury in the general population: the Trøndelag Health Study
🚨NORWEGIAN CONFIRMATION BOMBSHELL:
COVID infection leaves lasting, hidden scars on the heart muscle, even years later.
"An elevated cardiac troponin I (cTnI) level indicates the presence of heart damage!"
➡️Study:
- This was a prospective longitudinal cohort study within the Trøndelag Health Study (HUNT), a large population-based survey in Norway,
- Researchers measured high-sensitivity cardiac troponin I (hs-cTnI), a sensitive blood marker of subclinical myocardial (heart muscle) injury, at baseline before the COVID-19 pandemic (2017–2019) in 37,823 general-population adults,
- The same marker was then re-measured after the pandemic wave (2021–2023) in the 19,550 participants who returned for follow-up,
- SARSCoV2 infection status was rigorously determined at follow-up via spike and nucleocapsid IgG antibody tests in blood, combined with self-reported infection history and any available laboratory confirmation of prior infection,
- Infection was defined using nucleocapsid IgG (specific to natural infection, not vaccination) plus spike IgG, self-report, and lab confirmation, precisely to capture true infections regardless of vaccination,
➡️Pre-infection result:
- Higher baseline hs-cTnI was associated with a lower risk of subsequent SARSCoV2 infection,
➡️Post-infection result:
- Confirmed SARSCoV2 infection (any definition) was independently linked to higher post-pandemic hs-cTnI concentrations and a significantly greater probability of an increase in hs-cTnI from pre- to post-pandemic levels, after full adjustment for confounders and baseline troponin,
➡️Vaccination:
- Study reports that 98.9% of participants were vaccinated and explain(in Methods) why they used nucleocapsid IgG (not spike) to avoid vaccine confounding,
➡️Limitations:
- Correctly sited and commented,
- No data on symptoms, asymptomatic/mild/severe cases, or hospitalization, but one may rightfully assume that the majority were mild SarsCoV2 cases,
➡️Conclusion:
“SARSCoV2 infection is associated with increased risk of developing chronic subclinical myocardial injury in the general population, but pre-existing chronic subclinical myocardial injury is not associated with increased risk of contracting SARS-CoV-2.”
‼️To all minimiser still shrugging off SARS-CoV-2 as “just a cold” or “over”: this Norwegian study proves every infection silently scars hearts across the general public with lasting subclinical damage, and with the now-established cumulative cardiac injury from reinfections, your denial is quietly killing many! WAKE-UP!
#AvoidSars2 #AvoidReinfections
https://t.co/7CwdsPsslD
🔥 Excellent study on #LongCOVID demonstrating neuroimmune and autoimmune etiology of #LongCOVID. This is further proof to pre-pandemic studies on #POTS, #MECFS and #fibromyalgia demonstrating similar findings.
Our clinical paper on the topic: 🧠
https://t.co/fEkNHAQvKv
Small #LongCovid study finds LC patients' cells used way more energy than controls during infection, then way less.
This correlated with LC symptoms & suggests widespread metabolic reprogramming. Cells also ignored crucial hormone and metabolic signals.
https://t.co/f2XYoZTd2A
⚠️‼️In just 24 hours, hope for real treatment for Long COVID has moved forward.
For years, some of us have been pointing to the same pieces of the puzzle.
✅ Herpesvirus reactivations are part of the symptom-driving process in a subgroup
✅ Hypocortisolemia / secondary adrenal insufficiency exists in a subset of patients
✅ Autoimmunity is present in Long COVID, including anti-GPCR antibodies
And yesterday I highlighted again two ideas we have already discussed in previous papers and posts, which now seem even more relevant:
✅ A relevant subgroup of Long COVID / ME/CFS may fit anti-GPCR autoimmunity, especially autonomic and parasympathetic dysfunction
✅ Deep B-cell depletion / immune reset is starting to look like one of the most promising treatment directions
What is still missing?
⬜ To prove which susceptible ancestral HLA-II haplotypes are behind the loss of tolerance and autoimmune subgroups
⬜ To prove whether B-cell reset with CAR-T, like the approach that has already induced remission in lupus, can also become an effective treatment for Long COVID and ME/CFS
That is why this matters so much.
We are no longer just talking about vague “dysregulation.”
We are starting to see a much clearer model:
-persistent antigen / viral reactivation
-immune dysfunction
-autoimmune subgroups
-autonomic and endocrine subgroups
-and, hopefully, targeted immune-reset therapies
This is the first time in a long while that it feels like the field is moving from description toward actionable treatment logic.
That gives me hope.
Below I’m adding the posts I shared yesterday, because they connect directly to what is now being reinforced.
Save this post and let’s revisit it in a few years.
7) Practical message (for patients and clinicians)
📌 If your presentation looks dysautonomic/cholinergic, don’t stop at cortisol.
It would be reasonable to evaluate:
✅ anti-M3 autoantibodies (and other GPCR/mAChR depending on panel availability)
✅ and also a myasthenia gravis panel (e.g., anti-AChR, anti-MuSK, anti-LRP4)
Because:
• it may explain many symptoms
• guides symptomatic treatments (volume/salt, compression, thermoregulation, cholinergic approaches like Mestinon in selected cases)
• and, most importantly, helps objectify autoimmunity — crucial for future targeted therapies
5) Here comes the important part
In our model, many autoimmune diseases share predisposition via ancestral HLA-II haplotypes:
🧬 DR2-DQ6, DR3-DQ2, DR4-DQ8
The attached article does not yet study a statistical association with anti-M3 autoantibodies, but it shows immune reactivity against the M3 receptor presented through HLA-II in a small cohort, where several patients carried DR2-DQ6.
👉 https://t.co/0k7rFQOPFW
👉 This suggests that certain HLA-II backgrounds may facilitate presentation of M3R peptides and contribute to loss of tolerance against this target.
This supports the idea that we may not be dealing with completely separate diseases, but variations of the same immunogenetic framework:
Ancestral hyperreactive HLA-II + persistent stimulus → loss of tolerance → autoimmunity against different targets (M3, other GPCRs, etc.).