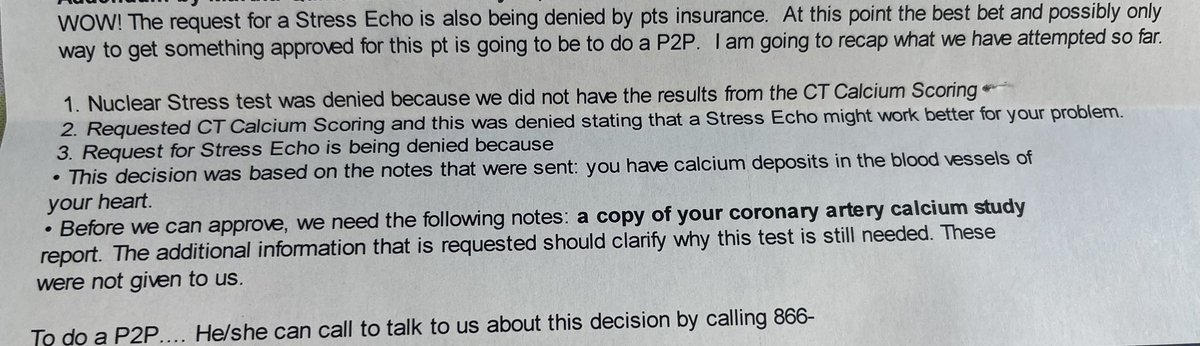
50’s M w DM HTN HLD new fatigue w exertion, tobacco user, lung CT w incidental CAC. Stress test ordered d/t symptoms/ risk factors.
Good ole American Healthcare
Stress -> denied order a CAC
CAC -> denied order stress echo
Stress echo -> denied order a CAC
Last chance to register for @SCAI FIRST Chicago Thurs April 17, 2025. Pls join @AdhirShroff & I for 5 great cases presented by #InterventionalCardiology fellows from around #ChiTown. (Come for the cases/stay for the colorful commentary :) #CardioTwitter
https://t.co/g7EaG6rodt
The 2025 ACS guideline synthesizes new evidence since the 2013 STEMI and 2014 NSTEMI guidelines and the 2015 focused update on primary PCI in STEMI.
This guideline was developed with @ACCInTouch in collaboration with and endorsed by @EmergencyDocs@NAEMSP@SCAI
@drjohnm@djc795 CCTA can be superior in that it offers a definitive answer. Not just affirming or refuting the presence of CAD, but also quantifying the extent. It is up to us as clinicians to decide when to halt the testing cascade though.
80 yo pt w/HTN, DM, HF recovered EF (45-50%) CAD, NASH & diverticular bleed 1 yr ago presents w crushing CP, HR 40, BP 90/50/63 MAP. DAPT+UFH in ED. ECG c/w inf STEMI; angio & still images👇🏽. What’s your preferred approach #CardioTwitter? #MedTwitter
@drjohnm The only thing to be skeptical of is the thought that a single lab or imaging test results should dictate the entirety of a patient’s care for the rest of their life - CAC of 0 has a very useful negative predictive value, but that NPV is not 100%
@DavidLBrownMD I think CCTA is a tool, and its intent depends on the person ordering the test.
However, if I’m getting a CCTA for any reason, and the FFR can be made available without subjecting the patient to increased risk, what’s the argument against it?
@DavidLBrownMD I agree that initial treatment is the same, but you just stated its value. Far superior to stress testing in terms of less false positive rate, and I can’t think of a better way to rule out left main without subjecting someone to the risks of a diagnostic cath.
Placing HFrEF in the context of other medical conditions may make the “extreme high-risk” and “very extreme high-risk” nature of HFrEF more readily apparent; lead to greater prioritization of HF prevention and treatment efforts
Contextualizing Risk in HF https://t.co/kIhOInNBuv
Finally, is CCTA the ideal test for patients with suspected NSTEACS?
(Due to tech issues, we only have the Con argument recorded – so feel free to put the Pro arguments in the replies!)
Pro - Dr. Klaus Kofoed
Con - @mirvatalasnag