New preprint on a controversial topic:
Through which socioeconomic mechanisms do individuals with higher genetic predisposition for educational attainment end up with higher income over their working life?
We study this using uniquely rich Finnish data.
New preprint out: Effects of introgressed Neanderthal alleles on present-day brain morphology! 🧬🧠 using 370 phenotypes derived from ~40k brain MRIs we found a textbook neanderthal-mediated GWAS hit at DAAM1, Neanderthal burden associations and more https://t.co/XbGKR5ptnG
🚨New preprint out
Mapping real-world statin adherence at population scale (https://t.co/0SSjYsixyA ). We analysed >1 million long-term statin users in Finland and Italy (Lombardy), identified adherence patterns, and examined baseline factors associated with declining adherence.
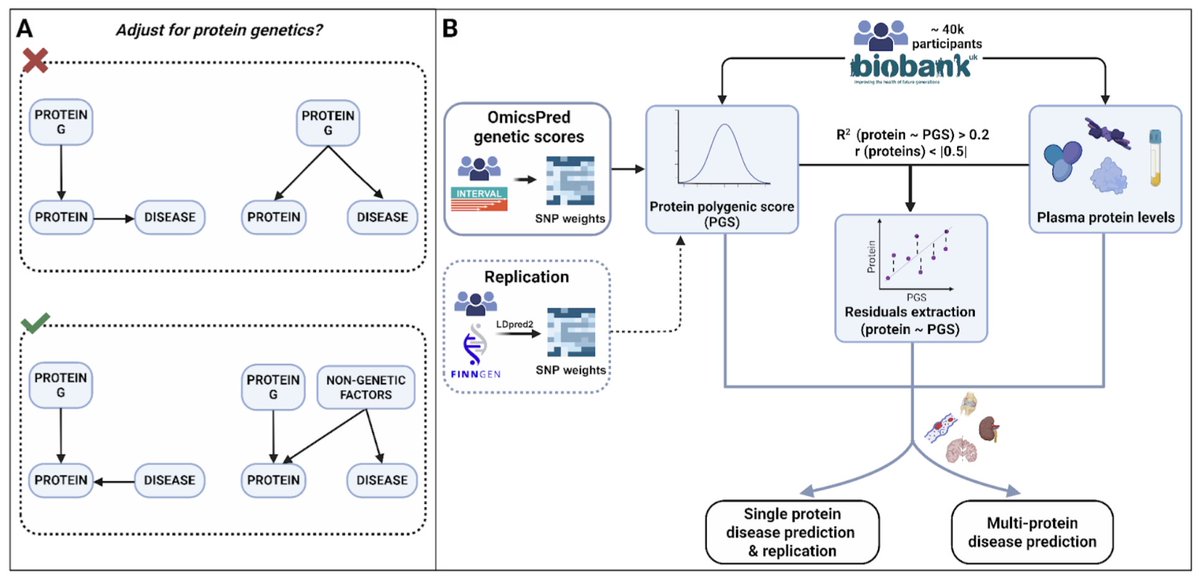
I liked the idea of this recent preprint suggesting that adjusting for genetic effects improves the utility of plasma proteins as biomarkers.
Most protein associations with disease risk were significantly stronger after adjusting for their genetic architecture.
https://t.co/22z1eX7FP8
New pre-print out! 🎉 With Mathilde + team we traced spatio-temporal shifts in genetically regulated #transcription across 10,000 years of Western Eurasia, fine-mapping regulatory features targeted by #selection! 👉 https://t.co/ihS4OoBats ! #popgen#genomics
We are pleased to announce that our new study explaining the missing heritability of many phenotypes using WGS data from ~347,000 UK Biobank participants has just been published in @Nature. Please check out our manuscript here: https://t.co/PK2DIpshOQ.
A new preprint reports a rare case of a boy with X-linked Fanconi anemia in whom the hematopoietic phenotype (bone marrow failure) was completely rescued by full triploid mosaicism (69, XXY) 🤯
Fanconi anemia (FA) is an inherited genetic disorder caused by mutations in DNA repair genes leading to bone marrow failure, congenital abnormalities, and increased cancer susceptibility.
The one of subtypes of FA is an X-linked disease caused by mutations in FANCB.
In a hospital in Melbourne, doctors one day encountered a remarkable case of a boy with FA. Initially he presented with clinical features suggestive of FA, along with positive family history with X-linked inheritance. Diagnostic work up confirmed a loss of function mutation in FANCB.
As any other child with FA, the doctors expected his clinical course to worsen with time, ultimately leading to bone marrow failure and requiring a bone marrow transplant. But then they noticed something strange!
As doctors monitored his bone marrow over time, they noticed an unusual shift in his cells' chromosomes:
At diagnosis: 99% of bone marrow cells were normal diploid (46,XY) - but FA-deficient
15 months later: 10% had become triploid (69,XXY)
25 months later: 95% triploid
28 months later: 100% triploid
Puzzlingly, his blood counts did not worsen during follow ups, and he didn't go into aplastic anemia.
A research team, led by Wayne Crismani at St Vincent's Institute in Melbourne, investigated the case and discovered something extraordinary.
Here's what happened:
The egg (that became this boy) carrying a defective FANCB gene on its X chromosome was fertilized by a normal Y-bearing sperm, creating a diploid (46, XY) embryo destined for FA.
But then something extremely rare happened: the second polar body from meiosis II that usually gets discarded during fertilization somehow got incorporated into early embryonic cells.
This polar body carried the mother's other X chromosome with a normal FANCB gene. Fusion of this polar body resulted in a mosaic embryo with two cell populations:
- diploid cells (46,XY) with a single copy of defective FANCB gene
- triploid cells (69,XXY) with two copies of FANCB gene--one defective and the other normal.
In most tissues, the triploid cells remained a minority. For example, his skin cells were 96% diploid. But in the bone marrow - where cells divide constantly and accumulate DNA damage - the triploid cells had a massive competitive advantage.
Over just two years, the triploid lineage spread through his entire bone marrow, replacing every cell with full triploid (69, XXY) genome.
The genomic fingerprint clearly showed that two X chromosomes in the triploid cells came from the mother: identical sequences near centromeres (where no cross-overs happen) and different sequences near telomeres (where cross-overs happen)
This pattern could only come from sister chromatids that separated during the mother's egg formation - one went into the egg, the other into the second polar body that was supposed to disappear but instead became this boy's lifeline.
This case represents an extraordinary case of "natural gene therapy" - a developmental anomaly injecting extra DNA inside cells treating a fatal genetic disease.
Sharp, Harris, et al. medRxiv 2025
https://t.co/9PMcJ5UHUF
🎉 New preprint out!
"Removing genetic effects on plasma proteins enhances their utility as disease biomarkers"
We show that adjusting plasma proteins for genetic effects can make them stronger predictors of disease
👉 https://t.co/vt3qYvmejW
🧬💥 Do the genetics that make you develop a disease also help you survive it? Not much.
Our new @NatureGenet including 9 disease and 7 biobanks shows:
• Susceptibility variants ≠ survival
• PRSs for onset weak at predicting survival
• Lifespan PRS predicts survival better
Matteo Ferro, a doctoral candidate in my team has a new blog on health data science where he is collecting the most interesting papers, each month.
Check it out!
https://t.co/gjmaiZCLn8