New @Nature study: >50% of lung cancer metastases are seeded by other metastases, not the primary tumor. This "seeding from seeding" reveals a complex evolutionary cascade that allows cancer to colonize the body.
https://t.co/lYUyfRYOcP
🧬 Tumor-agnostic therapies: time for living guidelines at @JCOPO_ASCO! From histology → biology
https://t.co/j4qb1LrtoS
💉💊Tumor-agnostic drugs (NTRK, MSI-H) are here
🤔 Trials (TAPUR, NCI-MATCH): cross-tumor feasibility
🔴 Gap: lack of real-time, unified guidance
🎯 Living guidelines = faster access & better implementation
Precision needs to be dynamic, as tumor-agnostic care can’t follow static guidelines
@OncoAlert@OncoReporte@myESMO@_SEOM
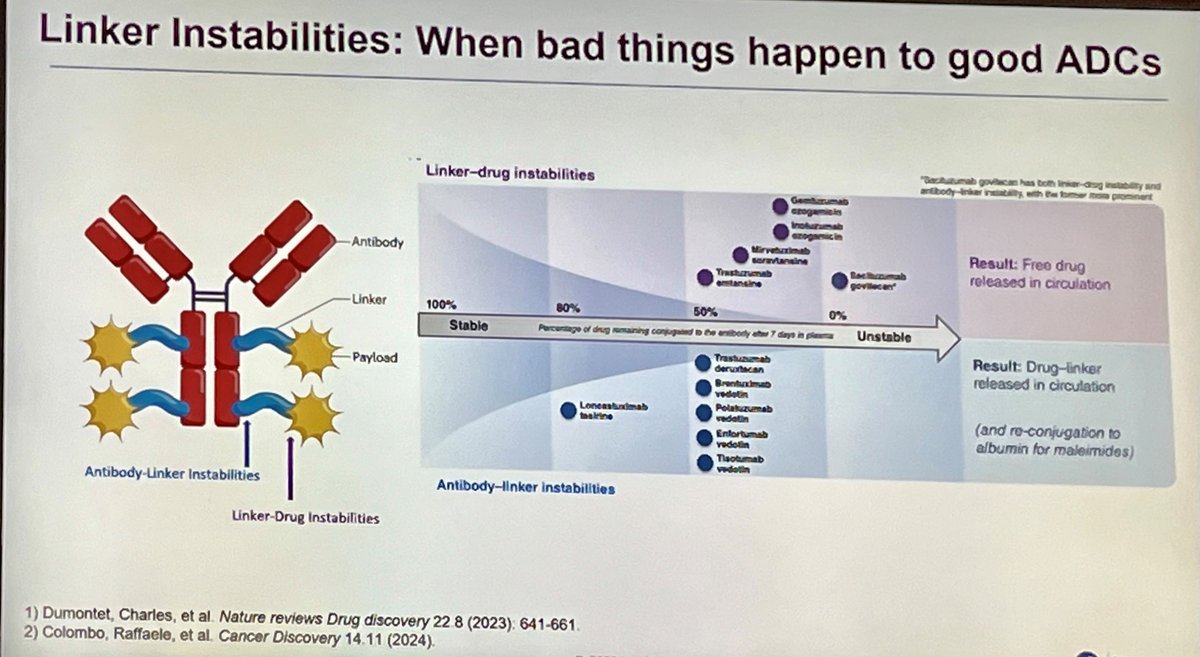
"Just 1% of the dose makes it to the tumor"😯
Dr Tolba shows why most ADCs go wrong at #NYLCF today:
▶️50-70% dissolve or degrade in circulation in 1st week
▶️ Most bind to albumin creating reservoir of cytotoxic that just sits in the blood.
Session led by @StephenVLiu, and @fred_hirsh
Is Unmutated IgG1 a Wrong Choice for Therapeutic Antibodies Targeting Immune Checkpoints? Lessons From the Clinical Failures of the First Anti–TIGIT Antibodies.
Read the full article. https://t.co/TNQwvtHMed
🫁 In pts with breast cancer brain metastases, ILD with #TDXd follows a biological pattern.
Pulmonary injury likely reflects Fcγ receptor–mediated uptake by alveolar macrophages, intracellular DXd release & a secondary inflammatory response rather than direct cytotoxic lung damage.
In this systematic review in @JournalCancer, ILD occurred in 10% comparable to non CNS populations, 11% discontinued tx, with no fatal cases.
Early recognition & steroids remain key.
https://t.co/cRLVQj64mX
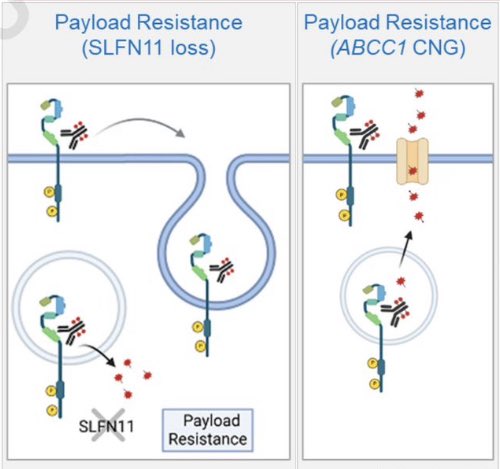
Wonderful study. Large part of the resistance to T-DXd derives from PAYLOAD resistance, via SLFN11 loss or efflux pump amplification. Thus, sequencing 2 ADCs with similar payload can lead to cross resistance, while switching payload is more likely to work. https://t.co/NzjHVq4yiI
Cancer Discoveryから、T-DXdの新たな抵抗性メカニズムの話。T-DXd後、HER2内在化によってHER2発現低下が見られたり(約半数)、トラスツズマブ結合部の変異がT-DXd取り込み減少で耐性につながる。
面白いのが、低濃度でT-DXdとDato-DXdを組み合わせるとこれを克服できるかも。
https://t.co/wXXHO6bsAy
Is TMB < 10 always a "cold" signal for immunotherapy?
New data in @OncJournal reveals that in TMB-low patients, specific mutations like VHL (in RCC), MAP2K1, SETD2, and PBRM1 are linked to improved OS under ICI therapy.
Full paper: https://t.co/sLOQgZaRU9
#Immunotherapy#TMB
This study clearly shows that resistance to trastuzumab deruxtecan is not drug failure — it’s target loss. @AACR@CD_AACR
• Nearly 50% of tumors lose HER2 at progression
• Some acquire ERBB2 mutations that block trastuzumab binding.
@OncoAlert#bcsm
https://t.co/aSiwp9rWGU
Trastuzumab Deruxtecan Resistance via Loss of HER2 Expression and Binding
In paired pre/post T-DXd samples, 49% show HER2 downregulation, with IHC 0 in 52%. ERBB2 binding site mutations ↓ T-DXd binding/internalization while DXd payload sensitivity is intact.
Low dose T-DXd + anti-TROP2 restores intratumoral DXd delivery & overcomes resistance in vivo. The next chapter after ADCs is just beginning
https://t.co/YaOjOEnaFq @OncoAlert
Expression of ADCs targets in post-mortem samples of breast cancer metastases and normal tissue: nectin-4 is higher in primary tissue, TNBC, and non-bone metastases https://t.co/GSRe01JK8a
Important Data!!!
Real-world evidence shows that the HER2 L755S mutation is associated with shorter treatment duration on T-DXd, while other kinase-domain mutations have heterogeneous effects.
Not all HER2-low tumors are biologically equal!
@OncLive@OncoAlert@brunolarvol@ozdogan_md@SuyogCancer
https://t.co/wOyg0WgZ6Y
Do you know how to FISH? I am delighted to share our 20+ years of experience with FISH, just published in @Human_Pathology (PMID: 40782985) - Everything You Need to Know About FISH!
This comprehensive review covers the full spectrum of fluorescence in situ hybridization (FISH) applications from HER2 FISH interpretation and 1p/19q deletion cutoffs to emerging applications, future directions, and the role of AI.
On a personal note, this paper has been two decades in the making. I began writing it nearly 20 years ago, when my late colleague and friend, Dr. John Eble, asked me to establish a molecular lab and implement FISH testing at Indiana University. Seeing it finally published is deeply gratifying. It’s true that it can take a decade (or two!) to write a comprehensive review and I’m thrilled that it’s finally out. I hope you find it a valuable and practical resource.
This review provides practical guidelines for the clinical application of interphase FISH in diagnostic surgical pathology. It discusses key technical considerations - including tissue preparation, interpretation thresholds, and limitations - and highlights selected diagnostic applications relevant to daily surgical pathology practice.
The central dogma that abnormal chromosomal DNA determines a diseased cell’s phenotype continues to have powerful clinical utility for tumor diagnosis and treatment. FISH remains a versatile, cost-effective, and rapid tool for detecting chromosomal alterations.
Even as technology evolves, pathologists must remain mindful of FISH’s underlying chemistry, potential artifacts, and clinical context. It continues to be an indispensable and irreplaceable adjunct in surgical pathology for resolving diagnostic dilemmas and identifying therapeutic targets.
The full article is available at the following link: https://t.co/d1Cerr9alo
#Pathology #Pathologists #SurgPath #pathresidents #MolDx #MolPath
Revisiting the Rationale for a Modern Systemic Total Neoadjuvant Treatment Approach for Locally Advanced Gastroesophageal Adenocarcinomas | JCO Oncology Advances https://t.co/MqqTmEZMH3
Does chemotherapy affect the biology of BRAF V600E mCRC when combined with encorafenib + ceruximab?
Answer appears to be YES! Very intriguing translational finding showing that addition of chemo to E+C reduces development of acquired RAS, MAP2K1 , and other mutations that drive resistance to BRAF + EGFR blockade.
Will use this data in counseling patients why we add chemo to E+C in this pt population.
👏 to BREAKWATER team for releasing translational data on their large 500 pt (‼️) analysis!! And congrats to the always amazing @skopetz for an incredible presentation- our @MDAndersonNews team remains so inspired by you!!
Ivonescimab plus chemotherapy versus tislelizumab plus chemotherapy as first-line treatment for advanced squamous non-small-cell lung cancer (HARMONi-6): a randomised, double-blind, phase 3 trial - The Lancet #ESMO25 @OncoAlert https://t.co/XEh1isU13k