Oral daraxonrasib nearly doubled overall survival in previously treated metastatic PDAC: 13.2 vs 6.6 months, with a 60% lower risk of death vs chemotherapy.
A major phase 3 signal for targeting active RAS.
#NEJM#PancreaticCancer#RAS#Daraxonrasib
https://t.co/qgHdwsYfpL
経口RAS(ON)阻害薬ダラクソンラシブが、既治療の転移性膵管腺がんでOSを13.2 vs 6.6カ月に延長という驚異的成績。死亡HR 0.40、PFSも7.3 vs 3.5カ月に改善した第3相試験。
#NEJM#膵臓がん#RAS阻害薬#臨床試験#daraxonrasib
https://t.co/rXvzsYbbte
経口RAS(ON)阻害薬ダラクソンラシブが、既治療の転移性膵管腺がんでOSを13.2 vs 6.6カ月に延長という驚異的成績。死亡HR 0.40、PFSも7.3 vs 3.5カ月に改善した第3相試験。
#NEJM#膵臓がん#RAS阻害薬#臨床試験#daraxonrasib
https://t.co/rXvzsYbbte
The biggest cancer meeting of the year just ended. The headline most people missed: some of the strongest results cost almost nothing.
4 wins from ASCO 2026, cheapest first:
1️⃣ Exercise, basically free. A structured program after colon cancer cut the risk of death 37%. Survival at 8 years: 90% vs 83% for usual care. The health economists ran the numbers and called it “dominant,” meaning it cost the system less AND people lived longer. They almost never get to use that word.
2️⃣ Low-dose immunotherapy, about $230 a month. A Mumbai hospital gave one tenth the usual dose of a checkpoint drug plus three generic pills. In head and neck cancer it beat standard chemo: 10.3 months of survival vs 6.2. Same class of drug that costs tens of thousands elsewhere.
3️⃣ The gentler prostate pill, same price as the harsh one. Two standard drugs control the cancer about equally. One (darolutamide) caused half the brain fog of the other (enzalutamide). Costs the same. The cheaper “win” here is just knowing to ask.
4️⃣The expensive one, when it’s worth it. A targeted combo for BRAF-mutant colon cancer doubled survival (30 months vs 15). It’s not cheap. But this is the case where the price buys you something real, the contrast that makes the first three land.
The pattern of the year: the next gains in cancer aren’t all locked behind a bigger price tag. Some are a referral, a dose, or a question you didn’t know to ask.
Which of these would you want your doctor to bring up first?
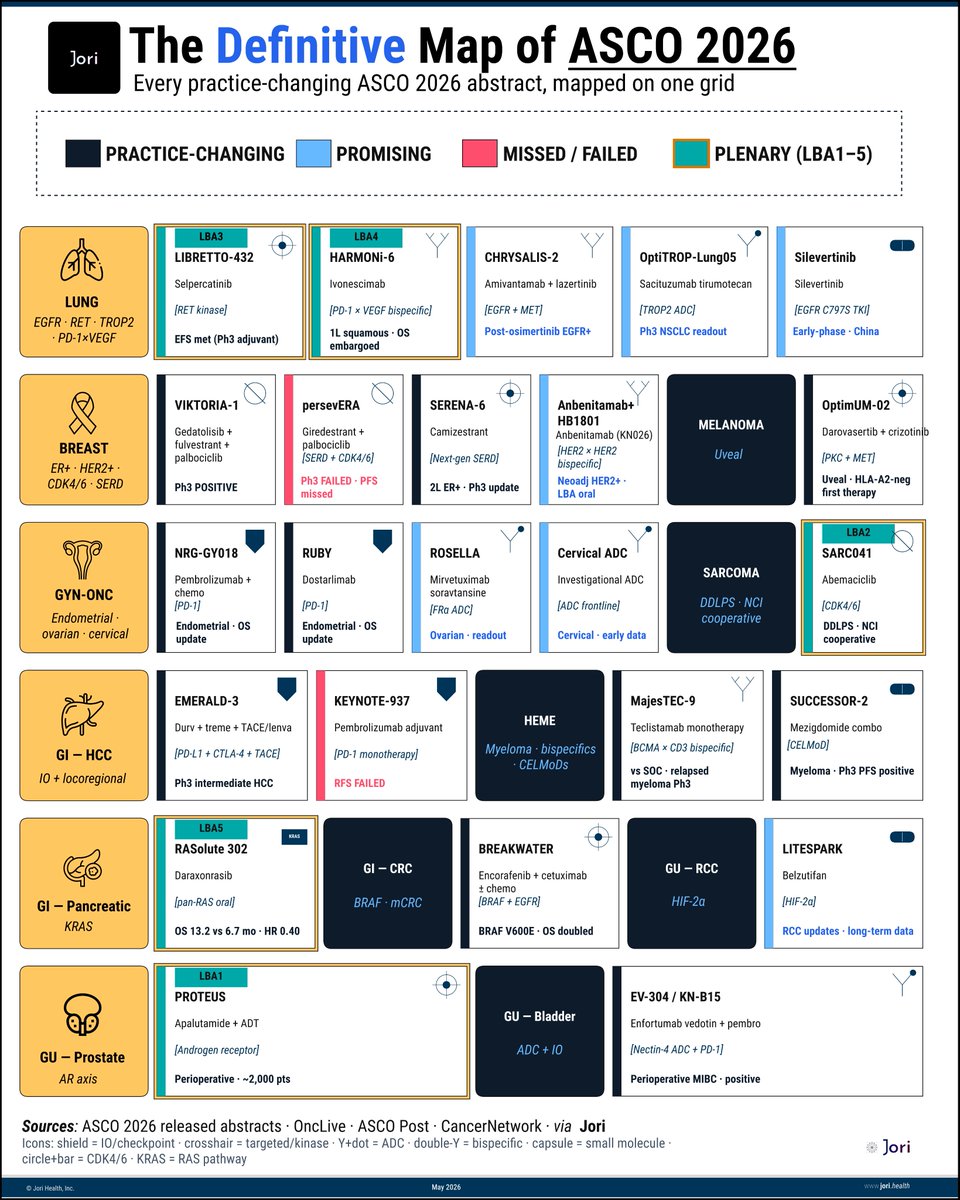
ASCO this year has 5,000+ abstracts.
But maybe 24 will actually change practice. This is that map.
(ERRATA: this plot fixes an error on VICTORIA which reflected incorrect data, thnx @Dr_RShatsky)
Map spans 12 disease areas, 24 critical readouts, 5 plenaries & 2 confirmed misses already on the board.
Few things jump out immediately:
▫️Pancreatic cancer gets the headline.
Daraxonrasib: 13.2 vs 6.7 months.
▫️Sarcoma gets a plenary because public science funded what pharma would not.
▫️Lung cancer remains the most crowded battlefield in oncology:
RET adjuvant, bispecific OS, post-osimertinib, next-gen EGFR.
By next week, some of these cells will become new standards of care.
This is your cheat sheet to keep score in real time.
- - - - -
Sources: @asco@OncLive@CancerNetwrk via @Jori_health
- - - - -