Biomed Scientist in #longevity. Mentor & Investor in Health startups. Past CTO @BioVivaScience ,Researcher @CASMIORG ,Lead @oxfordscisoc @NewsInLongevity ,BGRF
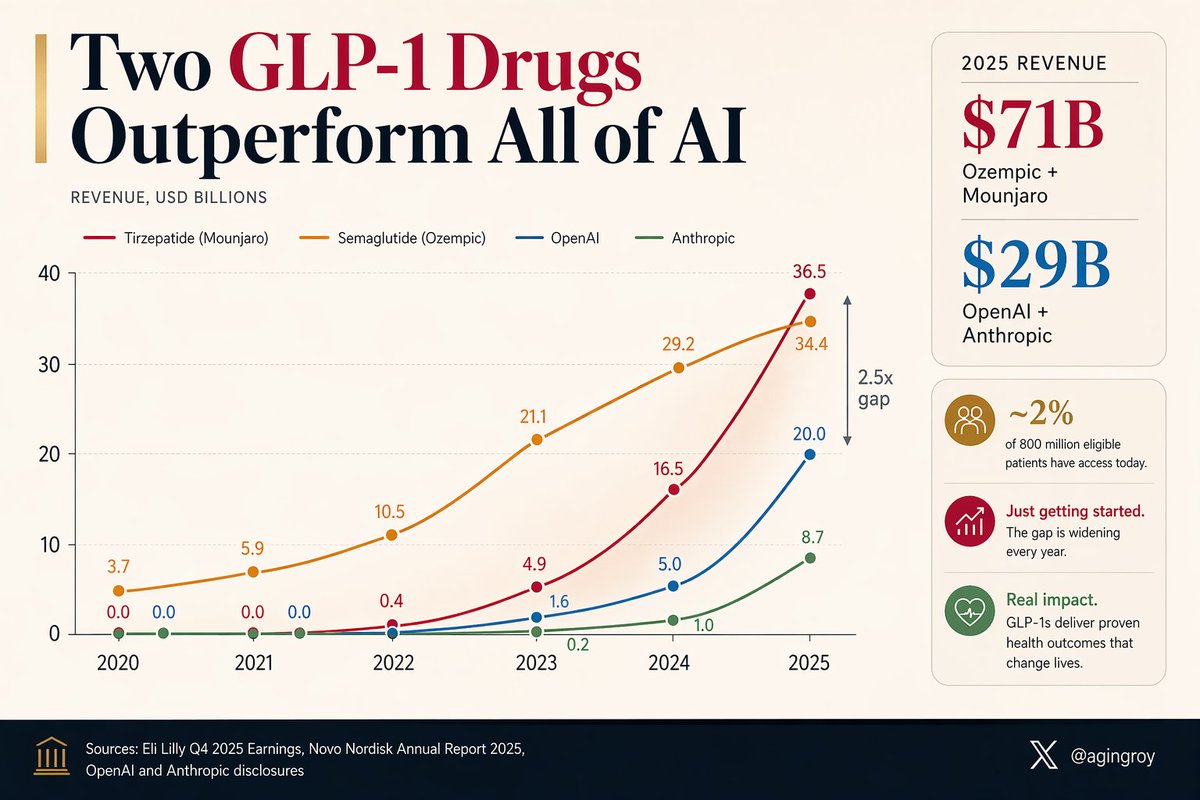
A weekly jab in the belly is generating more revenue than the entire AI industry.
Ozempic + Mounjaro: $71B in 2025.
OpenAI + Anthropic: $29B.
And they've barely started. ~2% of the 800 million eligible patients can currently access them.
h/t @DrSamuelBHume
Everyone on a weight-loss drug is being told to eat more protein and lift to save their muscle. Good advice. The cellular problem runs deeper than diet.
As muscle ages, an enzyme called 15-PGDH accumulates and destroys the very signal muscle uses to repair. @Stanford's Blau lab blocked that enzyme in mice losing weight on semaglutide. The fat still came off. The strength, which the drug alone had cut by nearly 40% after injury, came back.
A drug that switches your repair signal back on does something protein shakes cannot. The muscle problem behind the GLP-1 era finally has a target.
How to sustain muscle quality while losing fat?
GLP-1 drugs like semaglutide are transforming obesity treatment, but muscle loss remains a concern.
In mice, inhibiting the gerozyme 15-PGDH preserved muscle regeneration and strength during semaglutide-induced weight loss—improving muscle quality without compromising fat loss. #GLP1 #MuscleHealth #Aging
https://t.co/swFzPq7h6M
Sources, for anyone who wants the actual data.
The Kansas pilot (creatine in Alzheimer's, brain creatine +11%, cognition up on global and fluid composites, n=20, single-arm, no control group):
https://t.co/uVtIQ6x69n
The bioenergetic follow-up from the same trial (lymphocyte ATP rose, mitochondrial respiration improved in women, biology lines up with the energy idea):
https://t.co/u0rik2asnN
The brain-starving-on-a-scan part isn't new. FDG-PET has shown brain regions losing glucose uptake years before symptoms for decades. That's the established backdrop, not the surprise.
One honest note. Some posts going around say creatine "slowed decline 30%." That number isn't in either paper. The real result is smaller and earlier. The idea is what's interesting, not a headline stat.
We've treated Alzheimer's as a plaque disease for 30 years, and the drugs that finally clear the plaque barely help the patient.
The Alzheimer's brain may be starving.
For their size, neurons are the hungriest cells you own. Decades before memory slips, a scan shows the same regions going cold: hippocampus, posterior cingulate, parietotemporal cortex. They stop pulling in fuel as the mitochondria inside them wind down.
Creatine is the body's fast-charge battery. Muscles refill energy with it in seconds, and the brain runs the same system.
So a team in Kansas tried the obvious experiment: 20 people with Alzheimer's, 20 grams a day, 8 weeks. Brain creatine rose 11%. Several memory scores climbed with it.
Single arm, no control, 20 patients. Read it as a signal, not a verdict.
But if the energy idea holds, the amyloid drugs didn't fail because they were weak. They may have been treating the wrong half of the disease.
Sources, in the order they appear:
1. Smell loss as an early prodromal sign: established in the PPMI prodromal cohort (hyposmia), Siderowf et al, Lancet Neurology 2023. https://t.co/umjDsFjZtq
2. Acting out dreams (REM sleep behaviour disorder): 6.3% convert per year, 73.5% by 12 years, n=1,280, 24 centres. Postuma et al, Brain 2019. https://t.co/MFayXqnJRl
3. Smartwatch (wrist accelerometry) flagged Parkinson's up to 7 years before diagnosis and outperformed genetics, blood and lifestyle models. Schalkamp et al, Nature Medicine 2023. https://t.co/mtx3U1h0Bc
Caveat worth saying plainly: the lead time is real, but the absolute accuracy at a population level is still low. It's a screening signal, not a diagnosis.
4. Retinal scan (OCT): GCIPL and INL thinning showed up on average about 7 years before a Parkinson's diagnosis. Wagner et al, Neurology 2023. https://t.co/cvNPkzTeUM
5. Skin biopsy (Syn-One test): cutaneous phosphorylated alpha-synuclein detected in 92.7% of Parkinson's patients (89 of 96), with 3.3% of controls positive, n=428 enrolled across 30 sites. Gibbons et al, JAMA 2024. https://t.co/7eXuPfm0VW Commercially available in the US via CND Life Sciences.
6. Spinal-fluid seed amplification assay (SAA): about 99% sensitivity in classic sporadic Parkinson's, and it turns positive in prodromal people (RBD, hyposmia) who have no motor symptoms yet. Siderowf et al, Lancet Neurology 2023, PPMI / Michael J. Fox Foundation. https://t.co/umjDsFjZtq
The 2024 shift: a biological staging system (NSD-ISS) now defines Parkinson's by the alpha-synuclein protein detected in vivo, not by symptoms. Simuni, Hoglinger et al, Lancet Neurology 2024. https://t.co/SXSnDSdTar
The smell story: Joy Milne, the Scottish nurse who could smell Parkinson's, led to the sebum-odour work in Barran's lab at the University of Manchester.
Honest caveats: most of these detect risk, not certainty. The skin and spinal-fluid tests are the most clinically established; the smartwatch and retinal signals are population-level research findings, not personal verdicts.
By the time a Parkinson's tremor shows up, the disease has been running for a decade and most of the dopamine cells are already gone.
We can now see it coming. Six ways, ordered by how early they catch it:
1. Your sense of smell. Losing it is one of the first signs, often 10 years before a tremor.
2. Acting out your dreams. This sleep disorder turns into Parkinson's or dementia in 73% of people within 12 years.
3. Your smartwatch. One week of wrist movement flagged future Parkinson's up to 7 years early, and beat genetics and blood tests doing it. (An early warning, not a diagnosis.)
4. Your eye doctor. Routine retinal scans showed thinning about 7 years before diagnosis.
5. A skin punch you can order in the US today. It finds the Parkinson's protein in your skin nerves in 92.7% of patients, with almost no false alarms.
6. A spinal-fluid test. It catches about 99% of classic Parkinson's, and turns positive in people who still feel fine.
The shaking is the last thing Parkinson's does, not the first. Which of these would you want to know about yourself?
Longevity is being sold as a condo amenity now.
Here’s the thing the brochure won’t tell you.
The stuff with real evidence is cheap.
Walking. Sleeping enough. Old generic drugs being tested for aging, statins, metformin, viagra, and rapamycin, all still in trials.
Semaglutide went from luxury to near-generic in about two years.
Concierge care does buy earlier screening, and that matters.
You aren't paying for the science, you are paying for the fancy service.
Developers at a new New York luxury condo have leased its commercial space to a high-end longevity company that offers to lengthen the lives of its members. https://t.co/txLw1ERm2H
You learned in school that mitochondria are the powerhouse of the cell, locked inside it for life. That’s wrong.
Cells pass mitochondria to each other. New work in @Cell_Metabolism ties that swap to how cancer cells stay alive and how damaged tissue stokes inflammation.
Here’s why it matters beyond cancer. The same organelle trade is showing up in aging research, where failing mitochondria are a hallmark of aging.
One currency, moving between cells, sits underneath two of the hardest problems in medicine.
Cancer and the mitochondria @Cell_Metabolism
Effects of mitochondrial transfer between cells (pathological spelled wrong in figure) and these organelles as a driver of cell death, inflammation
https://t.co/vs6b11wwEf
https://t.co/4GFjBSLBYf
@MarkGPatterson That's the better question. VO2max tracks healthspan, not just lifespan. The fittest don't only live longer, they stay independent and out of hospital later. Quality and quantity move together here, which is rare.
5x higher mortality. That's the gap between the least fit and most fit adults, measured over 46 years.
7 wearable metrics that actually predict how long you'll live, ranked by mortality evidence:
1. VO2max —> HR 5.04 (fit vs unfit). Each 1 ml/kg/min ≈ 45 extra days of life. JACC 2018, 122,007 patients. Measurable on Garmin, Apple Watch, Whoop.
2. Grip strength —> Every 5 kg drop = HR 1.16 for all-cause death. Predicts cardiovascular mortality better than systolic blood pressure. Lancet PURE, 140,000+ people, 17 countries.
3. Resting heart rate —> Stronger mortality predictor than hypertension in adults 20-50. 2025 study, n=692,217. Your wearable reads it while you sleep.
4. HRV — > Each 10ms increase = 20% lower mortality risk. Oura Gen 3/4 now matches ECG accuracy for this metric among consumer wearables.
5. Gait speed —> Walk 4 meters. If it takes more than 5 seconds, you're in clinical frailty territory. No wearable needed. Just a hallway and a stopwatch.
6. ECG/AF detection —> 95% sensitivity, 97% specificity across 26 studies (n=17,349). AF doubles stroke risk.
7. SpO2/sleep apnea — >FDA-cleared AI algorithm detects severe OSA with AUROC 0.92.
The most accessible test on this list costs nothing. The others fit on your wrist.
@julezBee2@DrDenaGrayson Not yet, and it depends on the tumor. IMA401 targets MAGE-A4, a marker some solid tumors carry and others don't. It's Phase 1, so spinal mets would only be in play if the primary cancer expresses that marker. Early days for all of it.
A new cancer drug works like a molecular handcuff. One arm grabs a passing immune cell. The other grabs the tumor. It clamps them together and forces the kill, whether the cancer agrees to the meeting or not.
That trick cleared blood cancers a decade ago. Blinatumomab still does it in leukemia.
Solid tumors blocked it for one reason: the old handcuffs could only grab a protein sitting on the cell’s surface, and solid tumors hide their tells inside the cell.
This one reads the inside. Its grabbing arm is built from a T-cell receptor, so it spots the scraps of internal proteins that every cell puts on display. In a phase 1 study, 61 patients, it shrank head and neck, melanoma, and lung tumors that surface-only drugs never reached.
Solid tumors are most cancer. This is the first handcuff that fits them.
Just published @NatureMedicine and presented @ASCO
Advanced, refractory solid cancers treated with a bispecific T cell engager (BiTE, Figure), Phase 1 trial, with or without Keytruda, in 61 patients. Some very favorable responses with "manageable safety profile"
https://t.co/MkzQXY1psA
Best of a young field, agreed. The catch is the NHS-Galleri trial just missed its primary endpoint (combined Stage III+IV flat, IRR 1.03). It did pull Stage IV diagnoses down and cut emergency presentations 25%, so it's doing something. 'Best available' still isn't 'proven to extend life' yet. The $1K is the easy part.
If you’ve seen the ads for a GRAIL Galleri blood test that screens for 50+ cancers at once and wondered whether to get one, the biggest trial yet just reported real numbers. 142,250 people. What it actually does for you, in plain terms:
Screen 1,000 people.
-> About 9 get a “cancer signal found” letter.
-> Around 5 of them really have cancer, and some are caught early, before any symptom.
-> The other 4 get the fear and a round of scans that turn up nothing.
-> The test also stays quiet for about half the cancers that are truly there, so a clean result is not an all-clear.
Where it earns its keep is catching cancer earlier. More found at a stage you can still treat, fewer found after they’ve already spread, and a quarter fewer people learning they have cancer by collapsing into an emergency room.
Now the part it has not shown. Whether any of this makes people live longer. That trial is still running, so we genuinely don’t know yet. Worth knowing before you pay for one.
@allmeasures One of the better ones, yeah. The bispecific cleared blood cancers a decade ago with blinatumomab. Watching that same handcuff trick finally land on solid tumors is the part I didn't expect to see this fast.
@samuelgil Half the picture. Fix metabolism and a lot of disease eases, sure. But the bladder-cancer signal held even after adjusting for weight, so something beyond metabolism is moving. That's the part worth chasing.
Your heart is the organ that won’t heal. Adults replace under 1% of their heart muscle cells a year, a number Olaf Bergmann pinned down by carbon-dating the cells. So a heart attack kills about a billion of them for good, and the scar it leaves never fills back in. That’s why heart failure is a one-way door.
Here’s what the new gene therapy is trying to do. Heart cells can divide before birth, then switch that ability off and never turn it back on. A protein called YAP is the switch. The lead therapy, YAP101, flips it back on, telling surviving heart muscle to grow new muscle.
The field has been burned chasing this. The cardiac stem cell era collapsed in fraud, 31 papers flagged for retraction. The big gene therapy after it, SERCA2a, failed in 250 patients.
YAP101 has dosed three people so far. Safety only, no efficacy yet.
Worth watching. Worth not overselling.
Scientists are developing a new wave of gene therapies to regenerate the heart — offering hope for treating heart failure, a debilitating and common condition.
https://t.co/7E5bL7WWe4
The flat primary endpoint is the trap. Combined Stage III+IV came in at IRR 1.03, p=0.63, basically zero. But Stage IV diagnoses dropped 14% while Stage III went up. The test didn't miss those cancers. It caught them one stage earlier, which is exactly the point. The III+IV math cancels out the win.
@S_OhEigeartaigh Means the world, @S_OhEigeartaigh. The feeling is mutual and always has been. And congratulations on the far bigger news, the kid won the lottery on parents.
Neither, really. It's treatment, not prevention. You get it after surgery, once a melanoma's already been removed, to stop it coming back. In KEYNOTE-942 adding the vaccine to pembrolizumab cut the recurrence risk by about half at five years. A healthy person wouldn't take it to avoid ever getting melanoma.
The melanoma vaccine everyone’s sharing cut recurrence and death by about half at five years. Real result.
But the hard part of personalized medicine was never the idea. It was the factory.
A cancer vaccine built for one patient used to take months. This one was made in weeks.
@UrnovFyodor, who helped name gene editing, says that’s the tell: once you can print a custom genetic medicine on demand, the vaccine is just the first thing off the line.
The biology was ready. The supply chain finally caught up.
This mRNA is made in < 3 wks vein-to-vein time ... on-demand ... in a patient-specific way ... and thus is not in the IND.
= RNA on-demand for severe disease. In 3 weeks.
Hmmm. What does this remind one of?
Could it be ... gene editing on demand?
Yup. Watch this space.