Practice makes perfect!
You need a lot of questions and speak with the fellows in your hospital to see how you can get ACCSap, Mayo Echo Course, practice question books (Cleveland Clinic Echo Boards QBook, O’Keefe’s) may have educational funds in your residency.
- EKG: Marriott’s (classic) or Garcia’s or Chou’s (more advanced) followed by O’Keefe’s practice book and pocket ECG criteria book. O’Keefe’s ECG website is amazing for you to practice coding and ultimately that’s how you will learn. Highly recommend that over ECGSource outdated website.
- Hemodynamics/Cath/Echo fundamentals: Start with Elias Hanna book chapters on the are great. Hanna has a book on Hemodynamics as well which I recommend. Elias Hanna Cardiology book is a hidden gem eho made me survive my first year.
- Echo: Mayo Course and Alan Klein Echo Board Review Question Book. Although I wrote for Otto’s Textbook, which is very comprehensive, recommend Jae Oh’s Echo Manual as it is easier to start and follow Mayo Lecture.
- Nuclear/CT: For nuclear you have ASNC free resources and for cardiac CT we are doing a product with ACC called fundamentals of CT that will be released in August.
Ischemic ECG Patterns — STEMI Equivalents & Beyond
De Winter Sign as an Anterior ST-Segment Elevation Myocardial Infarction Equivalent https://t.co/5f4vJ1lNo4
Non–ST-Segment Elevation Myocardial Infarction in a Patient With Dextrocardia https://t.co/q5xGSoEloG
Aslanger Pattern as a Manifestation of Inferior STEMI in Multivessel Coronary Artery Disease https://t.co/XWII7TS7SS
Acute ST-Segment Elevation Myocardial Infarction Secondary to Neoplastic Infiltration of the Left Anterior Descending Artery https://t.co/6HkYig1ALv
Pseudo-Wellens Syndrome Caused by Myocardial Bridging https://t.co/J3JmtWNyCD
Successful Emergent Surgical Repair of Post–Myocardial Infarction Ventricular Septal Rupture With Cardiogenic Shock https://t.co/cZgnyMYv3R
Identifying Inferior ST-Segment Elevation Myocardial Infarction in the Presence of Left Bundle Branch Block: Seeing Through the Block https://t.co/1tXYFNXywS
Oscillating Wellens Syndrome: Multiple Transitions Between Type A and Type B Patterns Preceding Anterior Myocardial Infarction https://t.co/u411pNuAoj
The ECG in Congenital Heart Disease
Editor's Page
The ECG in Congenital Heart Disease: What Is Beyond the Tracing? https://t.co/26peRPd2zW
An Unusual Cause of Diffuse T-Wave Inversion: Coronary Arteriovenous Fistula https://t.co/x4v2VhBBMk
When Ebstein Meets Fallot: A Right-Sided ECG Puzzle https://t.co/lpShYAt3XF
Left P-Wave Axis Deviation: A Clue for Cardiovascular Malformation? https://t.co/9eKXGQhbLK
An Unexpected Electrocardiogram in Congenital Heart Disease: A Rare Variant of a Common Cyanotic Syndrome https://t.co/3dqPdAFwye
Cardio-Oncology — ECG as Early Warning
Editor's Page
When the ECG Speaks First: Early Electrical Signals in Cardio-Oncology and Infiltrative Heart Disease https://t.co/g9H7CsDeQV
Progressive Conduction Disease on Serial ECGs Revealing Immune Checkpoint Inhibitor-Associated Myocarditis and Myositis https://t.co/iz2lcmMPWu
ECG-Facilitated Detection of Light Chain Cardiac Amyloidosis in Long-Standing MGUS https://t.co/k6RxBwJNaP
Brugada Phenocopy Associated With the Tyrosine Kinase Inhibitor Avapritinib During Febrile Illness https://t.co/6x8CBZUE3Y
Author’s handles:
@KaczmarekMD@JakeReadMD@NSA0123@CraigBasman
@PWengrofsky
@RyanKaple
@JRodriPalomare
@J_Francisco_EP@EZancanaroMD@NuriaVallejo4@sofivilasanjuan@mnobremenezes@MdTakumi@enad1998@kumar_rk@kappanayil@DrJMarine@RWeinstein12@doctor_roig@DoctorSharmaMD@anjali_md1@KrityaMangesh@wonderingpcmkr@corneliaghea@TimVanPuyvelde@CompagnucciMd@CompagnucciMd@FahedAhmad05@CarlosVergaraMD@DrBridgetLee@vardar_md@Rajiv_EP@JFMundisugih
Apply for the William A. Zoghbi Global Research Initiative – 7️⃣ awards of $25K each!
✔️ 2 for #HeartFailure
✔️ 2 for #cvMetabolic health
✔️ 3 open to any area of CV care & research
Learn more & apply by June 8 ➡️ https://t.co/TRzOa3hUdA #ACCIntl@WilliamZoghbi
I wouldn’t necessarily recommend starting all the cardiology reading before fellowship unless you have extra time during your third year of residency.
That said, the following preparation was extremely helpful for me:
1. Marino's The ICU Book before the CCU rotation.
Cardiac Intensive Care By Dr Brown
A lot of cardiologists gradually lose touch with the intensive care aspect over time. As a fellow, being strong in ICU medicine can really help.
2. EKG books — read as many as you can. My favorites were:
◦The ECG Criteria Book Okeefe
◦Rapid Interpretation of EKG's Dubin
◦The Only EKG Book You'll Ever Need Malcom Thaler
3.I loved using a pocket cardiology book during my first year. I kept adding notes to it, and by third year it had become three times bigger. I did not use it as much later on, but it was invaluable early in training.
4. For echo, buy textbooks by Jae K. Oh, Catherine Otto, and board review by Allan L. Klein. I started reading them from the beginning of fellowship along with the Mayo echo videos, and it helped tremendously.
5. Finally, going home and reading Braunwald's Heart Disease on weekends and late evenings really helped reinforce everything I learned during the day. It is an excellent resource.
@CardioNerds has some excellent resources- wasn’t available when I was a fellow but I hear it’s incredibly useful
Pace yourself. Cardiology is a marathon, not a sprint.
If you are in your third year of internal medicine residency, I would start with the EKG books first.
#Cardiology #FIT #Cardiotwitter #CardioX
🫀 Inflammation: the missing piece in cardiovascular disease?
For years, we’ve focused on cholesterol, blood pressure, and traditional risk factors.
👉 But this statement shifts the paradigm:
inflammation is not a bystander — it’s a driver
🧠 A silent but powerful process
Cardiovascular disease often develops through:
👉 chronic, low-grade inflammation
👉 no clear symptoms
👉 persistent biological activity
➡️ This is the concept of residual inflammatory risk
Even in patients well treated with statins.
📊 A simple marker, big implications
👉 hsCRP can:
predict cardiovascular events
add information beyond LDL
identify high-risk patients even when cholesterol is controlled
➡️ In some cases, inflammation predicts outcomes better than lipids
💡 What does this mean in practice?
We may be:
👉 treating cholesterol
👉 but missing inflammation
➡️ and therefore missing risk
🔥 From concept to treatment
This is no longer theoretical.
👉 Anti-inflammatory strategies work:
Low-dose colchicine → ~25% reduction in CV events
Benefits seen without changing LDL
➡️ A true paradigm shift
⚠️ But precision matters
Not all therapies are effective.
👉 Some trials failed
👉 Others showed benefit only in selected patients
➡️ The future is targeted immunomodulation
🥗 Lifestyle is part of the therapy
Inflammation is strongly influenced by:
Diet 🍎
Exercise 🏃
Smoking 🚬
Obesity ⚖️
👉 Lifestyle changes are anti-inflammatory interventions
🧠 Beyond atherosclerosis
Inflammation also plays a role in:
Heart failure
Pericarditis
Vascular disease
👉 This is the rise of cardio-immunology
🔥 Take-home
We are no longer just treating risk factors.
👉 We are starting to treat biology
And inflammation is at the center of it.
#Cardiology #Inflammation #CardioImmunology #Prevention #HeartFailure #Atherosclerosis 🫀
https://t.co/FSz66gO7K6
Submit your research abstracts or clinical cases for the 6th annual NYU Critical Care Cardiology Symposium ⤵️
🔗 https://t.co/322MMeAco8
🗓️ Due by July 10th
Excited to be a @CardioNerds conference scholar with ⭐️ co-fellow @BrototoD#CritCareCards26
#ImageOfTheWeek by Dr. Awad Osman from University Hospital Limerick, Ireland. 83-year-old gentleman has no symptoms, what is the block level? https://t.co/4vLM5GGKeU
#cardioed
The European Society of Cardiology is deeply saddened by the passing of Professor Eugene Braunwald, one of the most influential figures in the history of cardiovascular medicine, who died on 22 April 2026, aged 96.
“Professor Braunwald was the leading cardiologist of his time. His vision and innovation changed the trajectory of cardiovascular medicine. He had a rare ability to see what the field needed next, and then to build the science and rigorous evidence leading to better care. He set a standard for intellectual honesty and mentorship, giving generations of clinicians and researchers the confidence to aim higher.” Professor Thomas F. Lüscher, @ESC_President
Professor Braunwald’s work helped define how cardiovascular disease is understood and treated. His legacy endures in the patients whose lives have been saved by evidence-based cardiovascular care, and in the people he inspired to pursue medicine with integrity and purpose https://t.co/IUtVSlbzph
Dr. Steve Nissen and I discuss how management is evolving beyond statins alone—highlighting earlier combination therapy, lower LDL-C goals, and expanded roles for non-statin therapy.
Sponsored by Esperion Therapeutics Inc., who did not influence the content of the presentation
Watch video here: https://t.co/IYRqqVRLj8
Can omega-3s do more than lower triglycerides? EPA-E reshapes cardiac metabolomic and lipidomic profilies, reduces inflammation, limitis oxidative stress, and preserves mitochondrial function, ultimately promoting a pro-resolving, cardioprotective enviroment. Read more in #EHJ.https://t.co/SwzXiDQzm8
#cardioprotection #inflammation #cardiotwitter @ESC_Journals@escardio
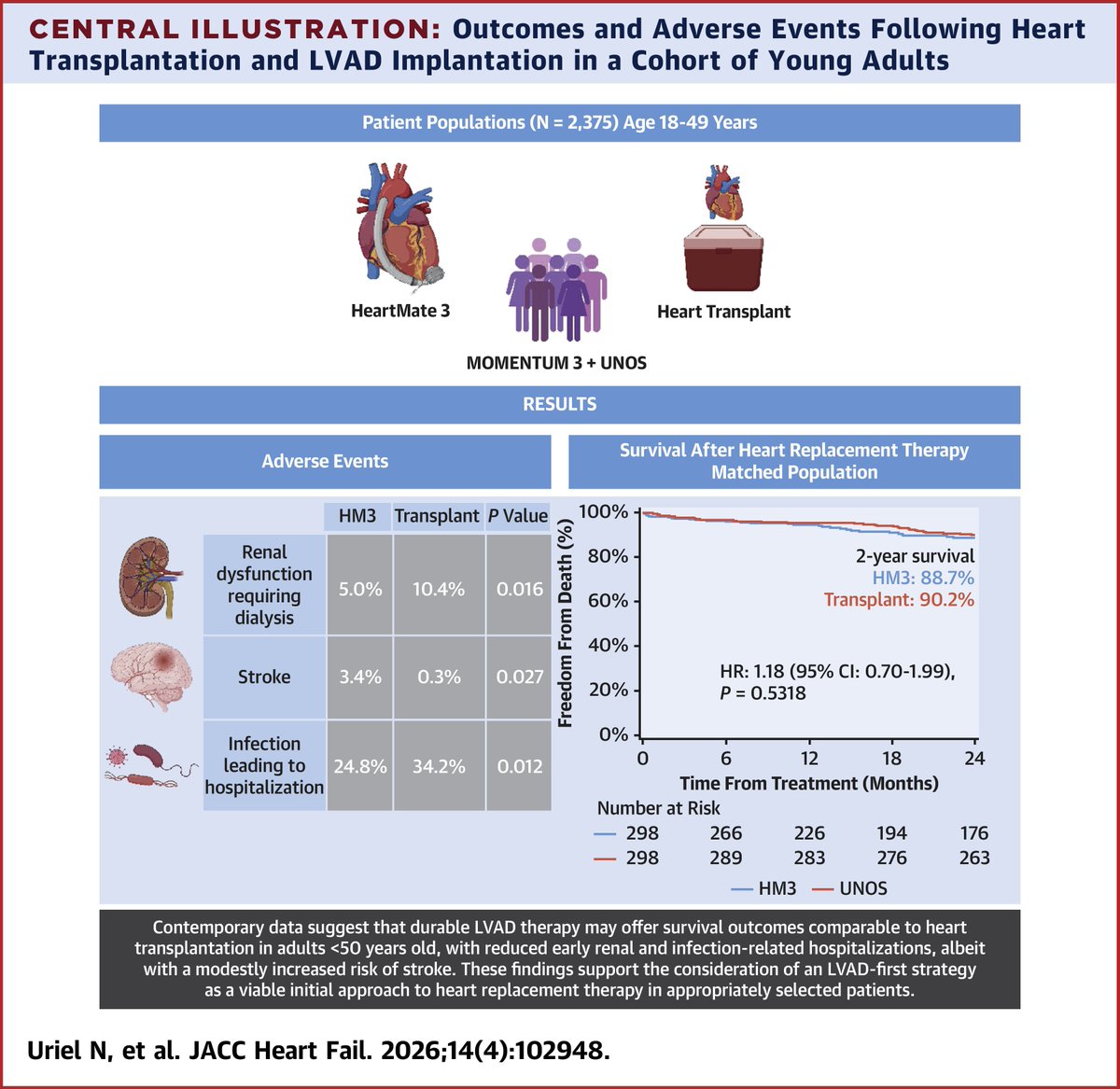
Contemporary data suggest that durable #LVAD therapy may offer survival outcomes comparable to #HeartTx in adults <50 yrs of age. These findings support the consideration of an LVAD-first strategy in selected patients. https://t.co/0Zjd3fq2yl #JACCHF
STEP trial: In older pts on intensive BP treatment, the trajectory of BP control was an effective predictor of CV risk, w/ a rapid-stable pattern associated w/ the lowest risk & uncontrolled or unstable patterns associated w/ the highest risk. 🔗 https://t.co/8iI4z4Mqdg #JACC
Syncope is defined as transient loss of consciousness due to cerebral hypoperfusion. Most syncope is not cardiac in aetiology, but cardiac syncope is a high risk subgroup.
This Practice article looks at how to identify cardiac syncope #MedEd
https://t.co/L8Xh8zkIUW
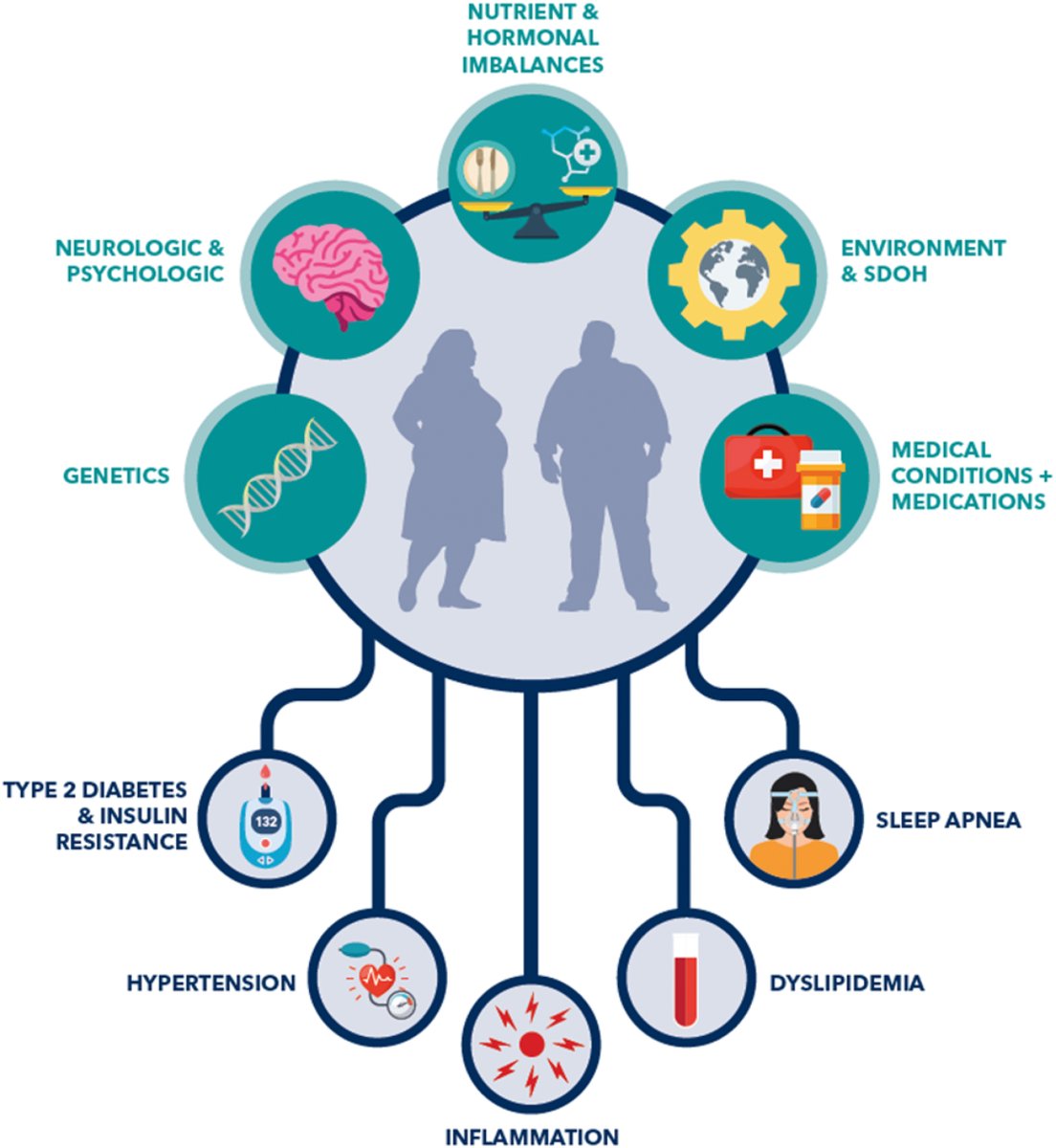
ACC's Concise Clinical Guidance report provides a framework for clinicians to medically manage obesity using the "ever-expanding set of tools to assist patients in diagnosis, weight reduction, & #CVD risk mitigation."
More: https://t.co/YAPb8T6VWl #ACCAsia#cvPrev@JACCJournals
New in #EJPC:
✅ In statin-treated patients with well-controlled LDL-C undergoing percutaneous coronary intervention, residual inflammatory risk (alone or in combination with residual triglyceride risk) is associated with a higher incidence of MACE.
📕 https://t.co/XisgvMVXyG
#EJPC @EJPCEiC@AboyansV@SilCastelletti@PTBuketAkinci@PeroneFrancesco@SMosteoru@TimKambic #cvprev
New #JACCCaseReports case highlights the synergistic interaction between pharmacologic thrombolysis and mechanical interventions, demonstrating their complementary efficacy in optimizing outcomes in extensive, limb-threatening #DVT. https://t.co/0QTwiOo3tr