Subjective estimation of sleep is actually not the best indicator of how good your sleep is
Partial sleep deprivation shows up in metabolic indicators of stress before we perceive them
My favorite well designed study on this topic:
The Economist makes a good point on sleep trackers:
Just as the only good bottle of wine is the bottle you enjoy, the best measure of how well you slept is if you wake up feeling rested.
A watch, ring, or those fancy new health tracking earrings are no substitute.
@cremieuxrecueil Subjective estimation of sleep is actually not the best indicator of how good your sleep is
Partial sleep deprivation shows up in metabolic indicators of stress before we perceive them
This is a well designed study on this:
https://t.co/EqR7bgX0cm
I spoke at @VitalistBay and found the speakers and tech discussed at the event very grounded in reality and science
In fact, my main takeaway was that there is not enough rigorous science going on in the antiaging field and the conference highlighted those few who are doing serious work in the field
A couple of panels included pessimists and dissenting opinions from researchers who don’t believe radical life extension is possible at all
A good response from the event organizer @adamgries
https://t.co/8YaXozeZex
This is pretty neat:
Patients who are at lower risk of having a cardiovascular event--heart attack, stroke, or death--get larger benefits from lowering their LDL.
The reduction in their risk is relatively larger than the reduction for higher-risk people!
NAD probably doesn't actually decline with age. This is one of the problems in NAD-world that I've been warning about for years. I'm glad to see it finally reaching publication.
https://t.co/0n2bzuBfeW
The myth that NAD levels broadly change with age in humans and other animals has been propagated by some high-profile people in the field, both in the scientific literature (mostly review articles not real data, which should tell you something) and in the pop-sci podcast world. This has generated hundreds of millions of dollars in sales for NAD precursors and hundreds of millions of dollars in grant funding for those investigators.
To be clear, NAD biology is real and important. There are likely specific disease states, tissues, or individuals where NAD availability becomes limiting and where interventions targeting NAD metabolism may prove useful. But that is very different from the much broader claim that declining NAD is a universal driver of normal aging in otherwise healthy people.
The evidence increasingly suggests that NAD precursors like NR and NMN do not extend lifespan in mice under standard conditions and likely provide limited or no meaningful benefit to the average healthy person.
This is a good reminder of how science should work. Strong claims require strong evidence, especially when they become the basis for major commercial industries and public health narratives. Aging biology is complex, and we need to be careful not to confuse plausible mechanisms with demonstrated outcomes.
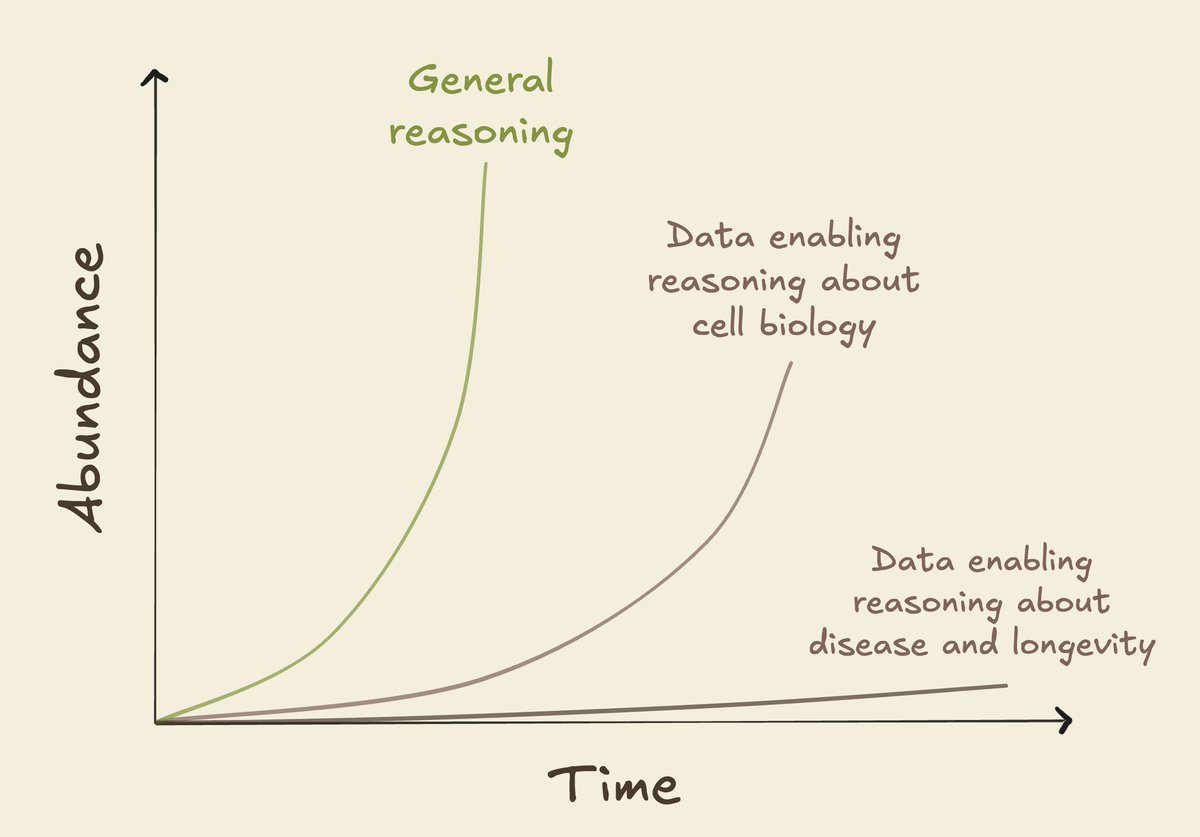
The “data for AI in bio” discourse is shifting from “we need data” to “what's the right data for this problem?”, and then how to produce it.
Right now there's a key gap between stated goals of curing disease and ongoing data generation efforts. We gravitate towards rapid and scalable experiments, even when those will never tell us how to treat Alzheimer's or aging.
The default path is that intelligence will explode, and cures will be stuck waiting for data that can't be accelerated.
There is work we should start today if we want to avoid that.
I wrote out thoughts on how we can identify data that will/won't let us cure disease, and how to overcome the technical and physical barriers to making it.
@edwin_mccallum Its more about measuring how tissues and organisms change over time and capturing that complexity. A lot of people are working on this but still underfunded I think
The problem in anti-aging science is a data problem which AI can’t fix
If we are not accurately measuring the aging process itself, then AI is mostly finding patterns in incomplete information. It cant “fill in” biology we dont capture
This is mostly BS
Sleeping >7.8 in an otherwise healthy person is absolutely not a sign of something wrong
And might be preferable
Especially for highly active people and athletes
If you feel like you need more than 7.8, do not try to shorten your sleep
The longevity dose for sleep is 6.4 - 7.8 hours.
> 23 biological aging clocks
> multi-omics: 11 proteomic, 5 metabolomic, 7 MRI
> 500,000 people
Interesting findings:
+ Brain proteins notice sleep loss before brain anatomy does. When you measure brain aging by plasma proteins, the brain looks biologically youngest at 7.82 hours of sleep in women and 7.70 hours in men. When you measure brain aging by MRI of brain anatomy, it looks youngest at 6.48 hours in women and 6.42 hours in men.
+ The brain and the metabolic organs share the same U-shape but hit their optimum at different hours. Fat tissue and the pancreas both bottomed near 6 hours. The brain bottomed higher, between 6.4 and 7.8 hours depending on whether you measure by MRI or plasma proteins. Sleep less or more than the organ-specific optimum and aging accelerates.
+ Short sleepers vs long sleepers DNA.
Short sleepers' DNA matched the DNA of people whose bodies are breaking down all over.
> back pain 40%
> depression 37%
> substance use disorders 37%
> anxiety 32%
> heart failure 31%
> lung disease 28%
> type 2 diabetes 18%.
Looking at genes only, chronically too little sleep makes the body look like it's breaking down everywhere.
Long sleepers' DNA matched the DNA of people with brain conditions versus whole body breakdown.
> major depression 29%
> schizophrenia 28%
> ADHD 28%,
> migraine 28%
> bipolar disorder 21%
Short sleep gets you through the body directly: the nervous system get's aggravated, the immune system gets confused and stress hormones flood the bloodstream.
Long sleep get's you through the brain, but it's the result and not the cause. By the time someone is sleeping too long, the damage is already happening inside their organs.
Summary:
Less than 6.4 hours is a stressor. Your body is wearing down because it never gets enough time to recover. The short sleep is what is causing the damage.
More than 7.8 hours is a warning sign, signaling that something is already going wrong in your brain or your metabolic organs.
BPC-157 was tested on HUMAN knees. Not rats. Humans.
16 patients. Real knee pain. Osteoarthritis. Meniscus tears. Ligament damage.
Their doctors gave them two options: cortisone or surgery.
They got BPC-157 instead.
90% reported pain relief. Not for a week. Not for a month. Past 6 MONTHS.
(PMID: 34324435)
Every time someone says “it’s just rat studies” — show them this.
Cortisone numbs pain for 3 weeks then BREAKS DOWN the collagen holding your knee together. You pay $500 to accelerate the damage.
Surgery costs $15,000-50,000. Months of recovery. And most knees are never the same.
BPC-157 grows new blood vessels into the damage. Builds fresh collagen. Activates repair your body stopped sending.
→ 90% pain relief past 6 months
→ no surgery
→ no cortisone
→ no side effects reported
→ a peptide your stomach already makes
16 patients. 90% success. Published. Peer-reviewed.
Your orthopedic surgeon charges $30,000 and gives you a 60% chance.
BPC-157 cost a fraction and hit 90%.
That’s not even the craziest thing BPC-157 has done. Check the comments.
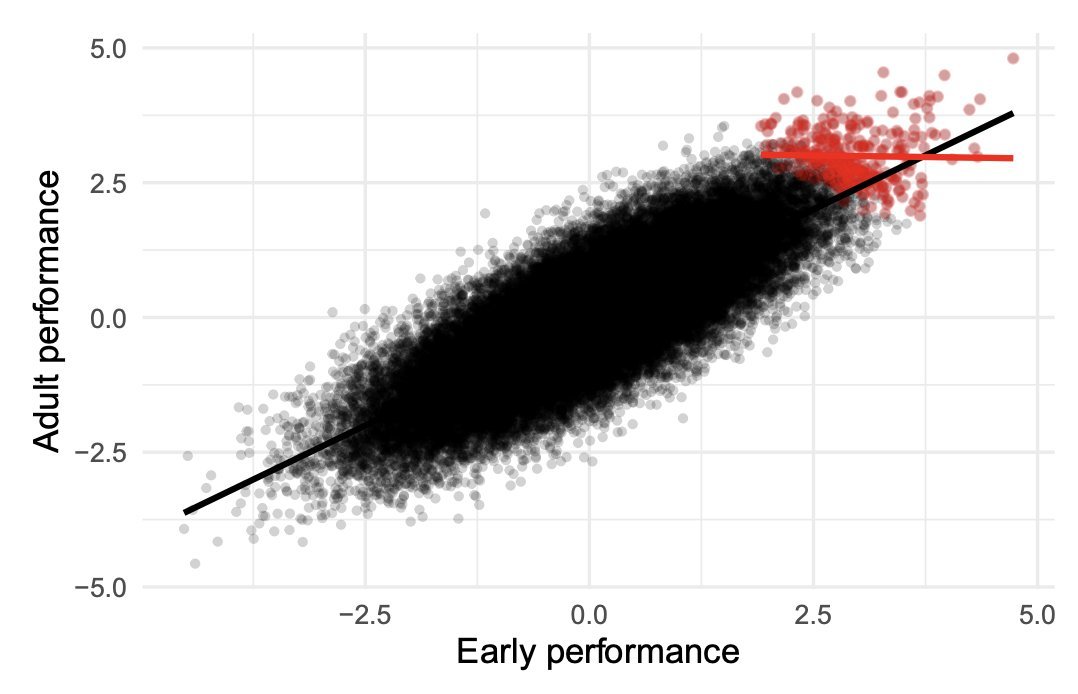
Among elite chess players, those with the lowest IQ are the best.
Among NBA players, the shortest ones are the best.
Among Hollywood actors, the least attractive are the most talented.
Among elite academics, those with poorer early academic performance are the best.
Among people with high LDL & high plaque burden, LDL is barely correlated with plaque burden.
Learn collider bias. Nice catch by @AlexTISYoung
This @NYTmag article on longevity science, reversing aging with cellular reprogramming, by @susandominus, is over the top. We have no proof that rejuvenation of a human organ is possible, no less the whole body, and there is risk of inducing cancer.
gift link https://t.co/VEGpaBncFN
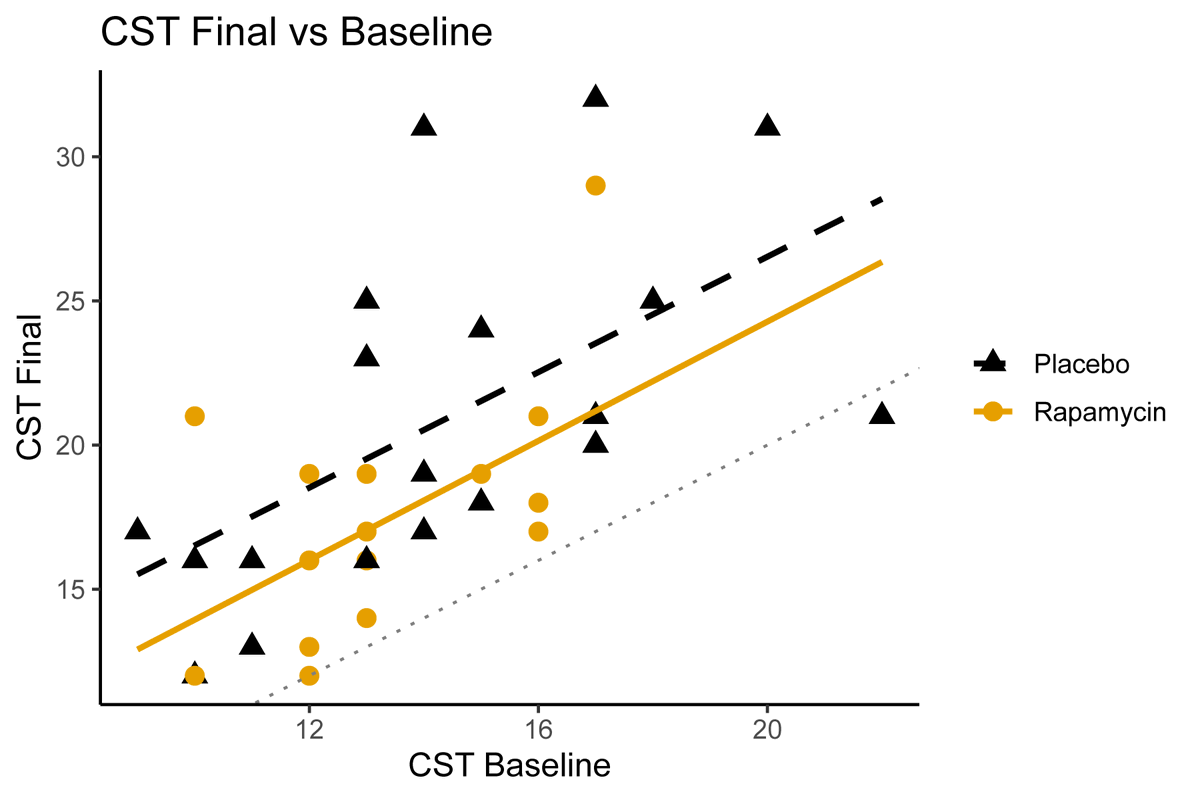
Impressive study and even with the limitations, is an important addition to the Rapamycin literature
In my opinion, the only plausible off-label use of Rapamycin currently should be in ApoE4 carriers as not many options are available). That would be an important trial we are currently lacking
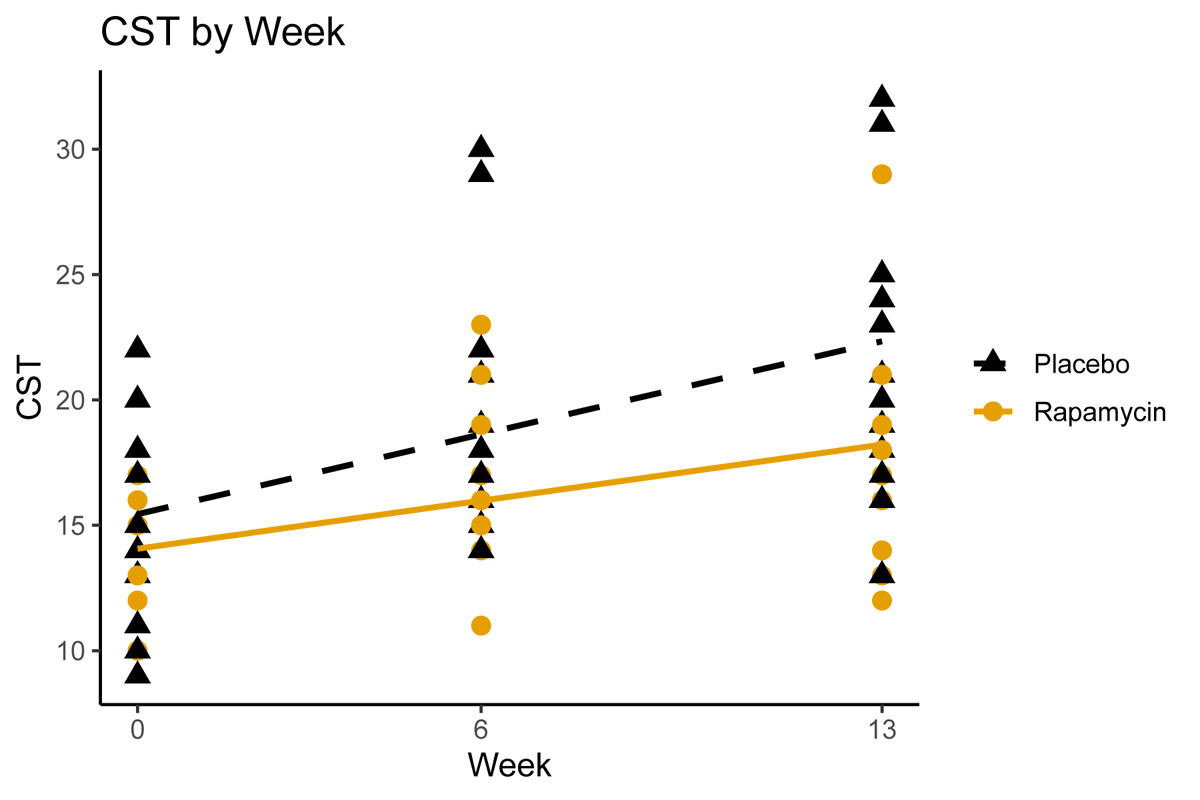
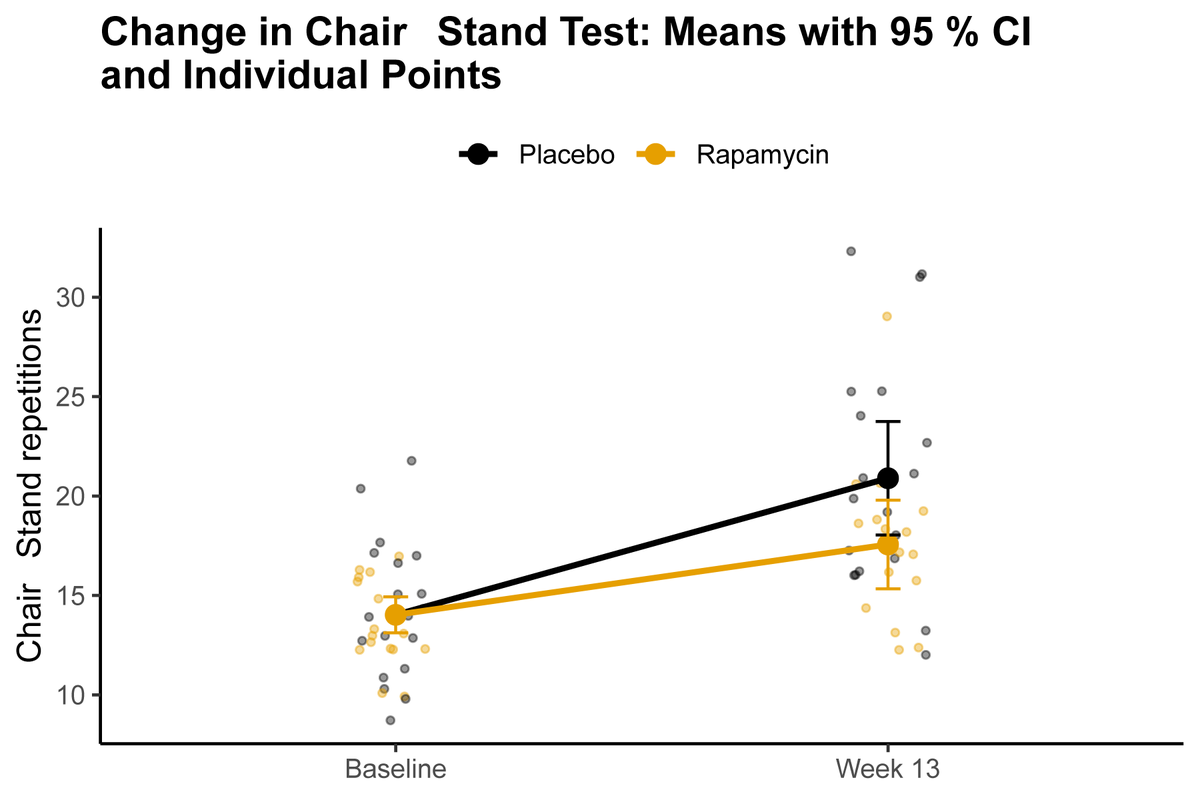
Our Rapamycin & Exercise clinical trial has just been published!
The topline result?
Rapamycin didn't help. Instead, it may have made things worse.
Here's what we found 🧵
https://t.co/vpy9bPrGDJ
Drug hunters everywhere, sear the lesson of Revmed and daraxonrasib in your brain:
Life is too short for incrementally me-too and me-better. Drug the fucking undruggrable and you can double OS, even in pancreatic cancer.
Absolutely inspiring. LFG.