🚨 We need your help! 🏛 This Tuesday, March 11, 2025, Congress will begin votes on a continuing resolution that includes a devastating 57% cut to the Department of Defense’s Congressionally Directed Medical Research Program. The Prostate Cancer Research Program has been instrumental in developing most of the cutting-edge treatments our community relies on today. These massive proposed cuts would severely jeopardize the future of prostate cancer research.
Make your voice heard! Contact your elected officials today, tomorrow, and Tuesday!
💻 Click the link: https://t.co/MOtCk1UKDd
📲 Text CDMRP to 1-888-824-4109
#ZEROProstateCancer #ProstateCancer #HealthcareAdvocacy #Congress
@jgong15@MPishvaian@AnthonyNguyenMD Good point, in STAMPEDE (Arm H) 18% received docetaxel, as SOC evolved to include docetaxel for mCSPC as trial was accruing. I'd have to dig to see what percent of low vs high volume patients received docetaxel.
13/20 #TumorBoardTuesday
📋Back to our case
65M with de novo low-volume mCSPC
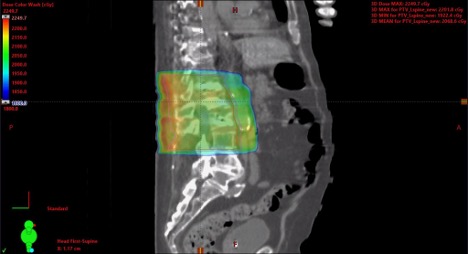
Prostate RT 5500 cGy ⚡ in 20 fractions
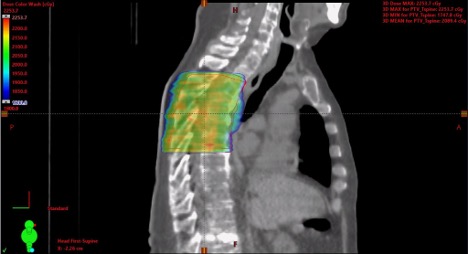
SBRT 2000 cGy ⚡X5 fractions to T7 and L3 mets
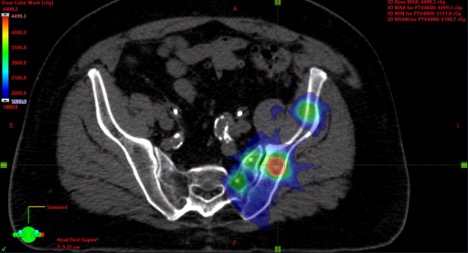
SBRT 4000 cGy ⚡ X5 fractions to L iliac met
@MPishvaian@AnthonyNguyenMD Yes, STAMPEDE (arm H) trial showed OS benefit with RT to the primary given concurrently with ADT (vs ADT alone). We tend to extrapolate and give SOC ADT + ARPI (abi/apa/etc) while treating the primary. More studies are ongoing to evaluate.
20/20 #TumorBoardTuesday
Summary
Ability to detect oligomets will likely change with more use of PET-PSMA, e.g., patients with biochemical relapse but no apparent mets on conventional CT or bone scan → 74% PSMA-positive lesions
Post-Test 2 #TumorBoardTuesday
TITON data for 1L apalutamide + ADT in mCSPC indicate that PSA ⬇️ ≥90% or levels ≤0.2 ng/mL in the first 3 months extend OS by:
@MPishvaian Agree. Logically it makes sense treating the primary would have (more) benefit if you have less disease elsewhere. Nice when you have data to back up that gut-feeling.
9/20 #TumorBoardTuesday
💡Mini tweetorial 5
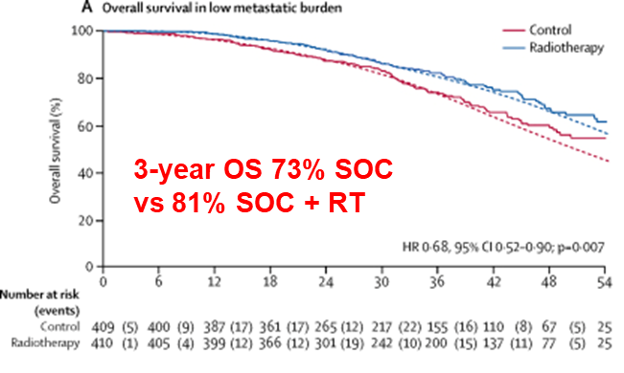
📚STAMPEDE (Arm H) trial
ADT vs ADT + radiotherapy to primary
Prespecified low and high burden of disease groups
High burden: no OS difference
Low burden OS at 3 years: 73% w/o RT vs 81% w/ RT
@MPishvaian Correct. The common fusion is TEMPRSS2-ERG, where ERG is the oncogene partner. There is some preclinical data supporting ERG inhibition, but none in the clinic that I know of.
6/20 #TumorBoardTuesday
📋Back to our case
65M de novo low-volume mCSPC
NM bone scan, MRI, CT CAP show bone mets to L iliac, T7 spine, T3 spine 🩻
🧬NGS shows MSS, TEMPRSS2 fusion, BARD1, FGFR4
💊Bicalutamide → 💉leuprolide 22.5 mg IM Q3 months
Started apalutamide 240 mg qd
Great point/question. mOS is a little deceiving to compare here since the PEACE-1 data is separated between low and high volume. When PEACE-1 low and high populations are pooled their control arms (ADT + doce) have a similar mOS: 4.4 years (PEACE-1) and 4.1 years (ARESENS). PEACE-1 pooled mOS:
3/20 #TumorBoardTuesday
💡Mini tweetorial 2
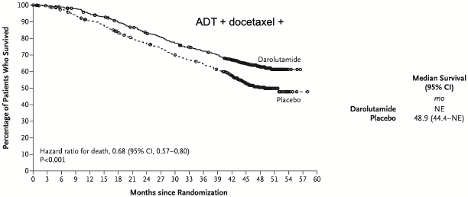
2.📚ARASENS trial
ADT + doce vs ADT + doce + darolutamide
Including both low and high burden of disease
Median OS: 48.9 months w/o daro vs Not Reached w/ daro 🏆
17/20 #TumorBoardTuesday
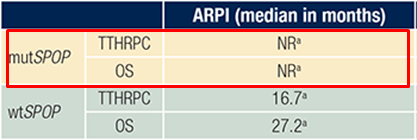
Lack of an established biomarker to guide 1L therapies in mCSPC
🔬Studies ongoing, e.g. SPOP mutations 🧬may be predictive for ARPI + ADT
15/20 #TumorBoardTuesday
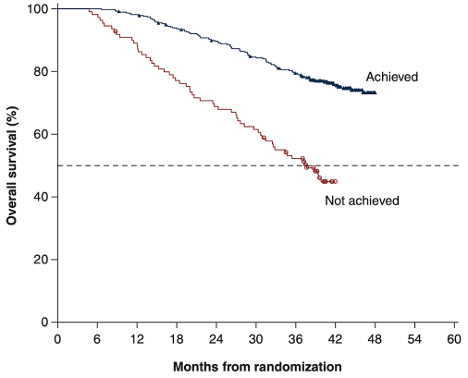
💡Mini tweetorial 7
Sig of rapid, deep, and durable PSA declines with apa + ADT
Post-hoc analysis of 📚TITAN, median 44.0 mo
Pts: mCSPC getting ADT + apa
Achieved: >90% PSA decline or PSA <0.2 ng/ml at 3 months
Median OS: 37.7 months “Not achieved” vs Not Reached “Achieved” (HR=0.35)