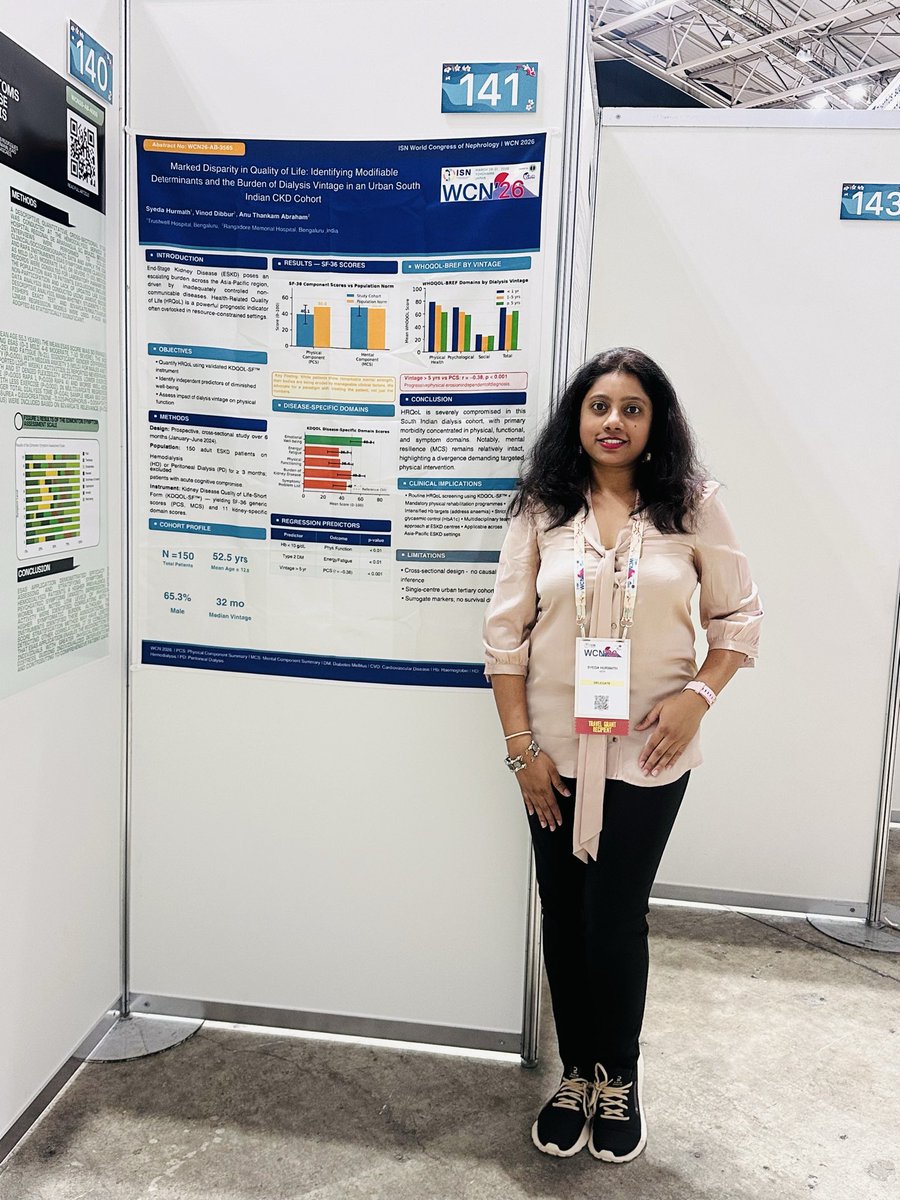
My first WCN conference in beautiful Japan—an enriching experience. Grateful for the opportunity to present my abstract. Thank you @arvindcanchi sir and Dr. Vinod Dibbur sir for your constant support, opportunity and guidance.#WCN2026
We presented a poster on Desidustat in #CKD anemia - A real world experience 👉 at #ISNCON25 today. Most of the work on this poster was done by @DrSyeda_hurmath!
Had a great time at the #Onconephrology meet with Chennai Kidney Associates in the presence of the phenomenal Dr. Rimda Wanchoo @renalmyeloma .Always a pleasure reuniting with my Chennai gang! Thank you for an amazing evening.
PC : @WordsofHemnath
Thank you, Dr. Shruthi Tapiawala mam this amazing course turned transplant immunology from a maze into a clear path. Your clarity, patience, and passion made every complex concept easy to understand. I’m grateful for all the effort you put into teaching. @AtdiMumbaiLab
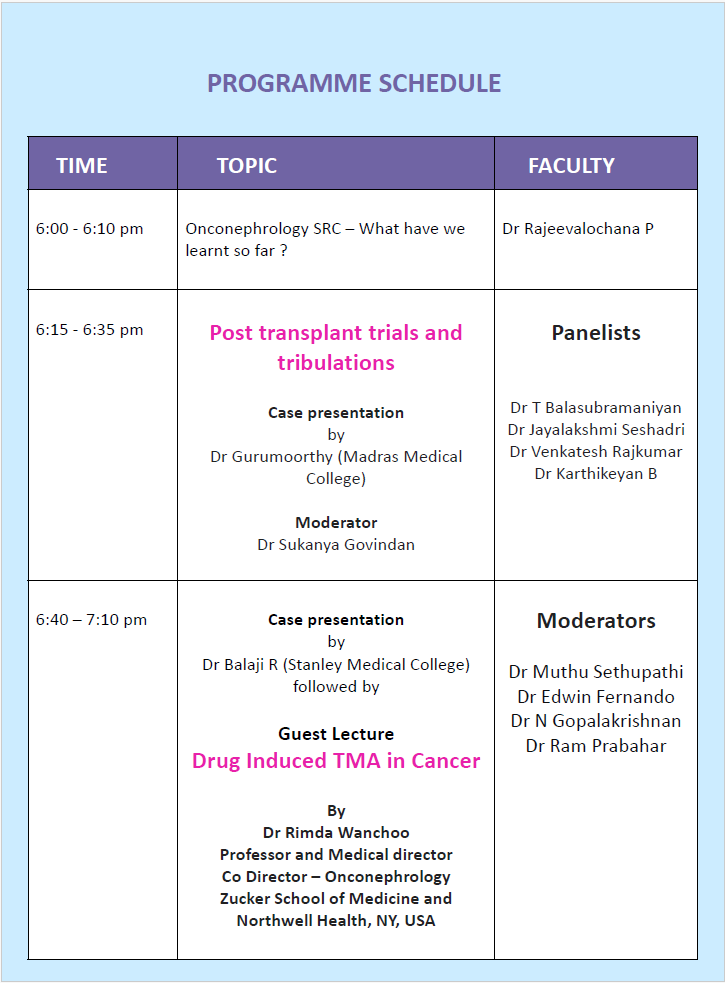
📢Dear Senior Nephrologists, Colleagues & PGs,
Join us at the #Onconephrology CME to witness expert-led case discussions on all key topics
🗓️ Date: December 16, 2025
🕒 Time: 6:00 PM - 9:00 PM
📍 Venue: Taj Wellington Mews, Chennai
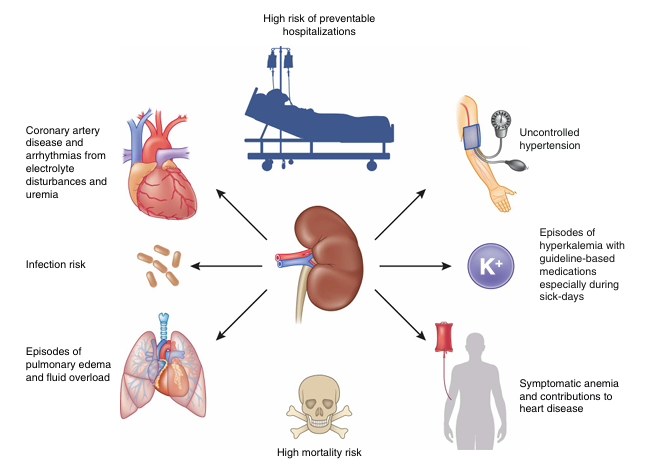
What are the drivers of preventable hospitalizations in patients with kidney diseases? And how can clinicians best intervene? This review in #ASNCJASN evaluates the current state of the science: https://t.co/chNdZ2jJ4B
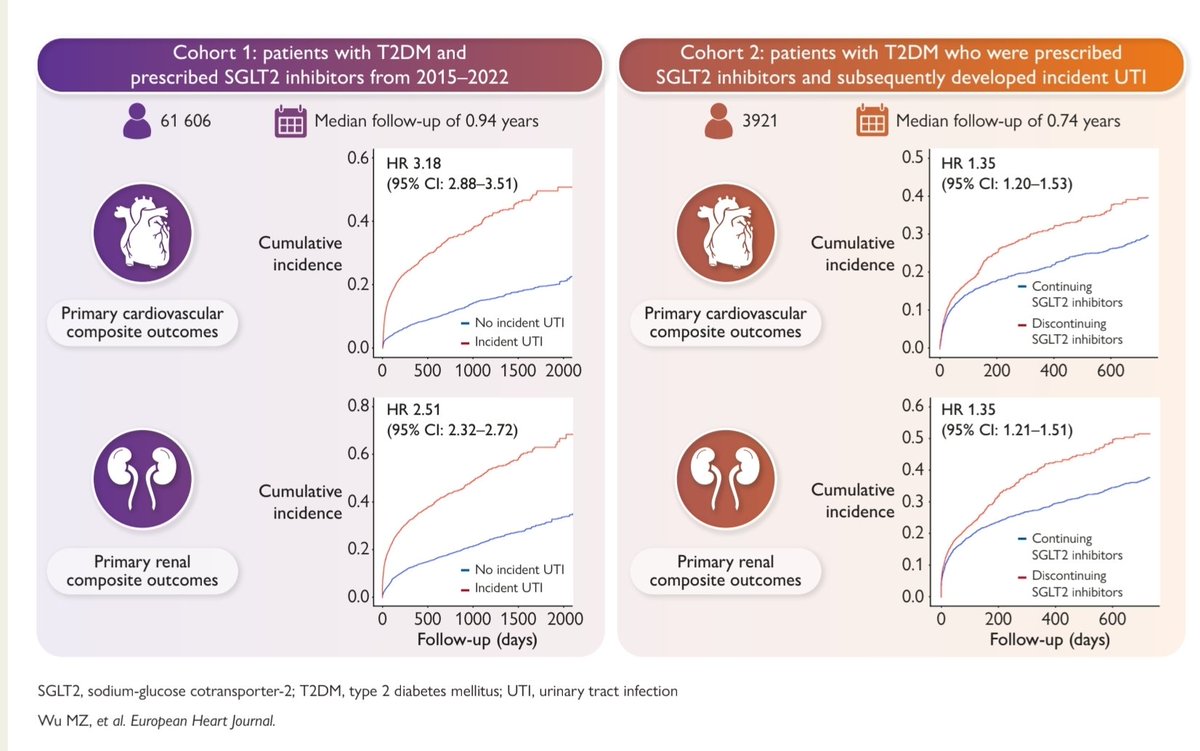
SGLT2i & UTI: Continue or Stop?
🧩 Key Question:
What happens when patients with T2DM on SGLT2 inhibitors develop a new-onset UTI?
Should therapy be continued or discontinued thereafter?
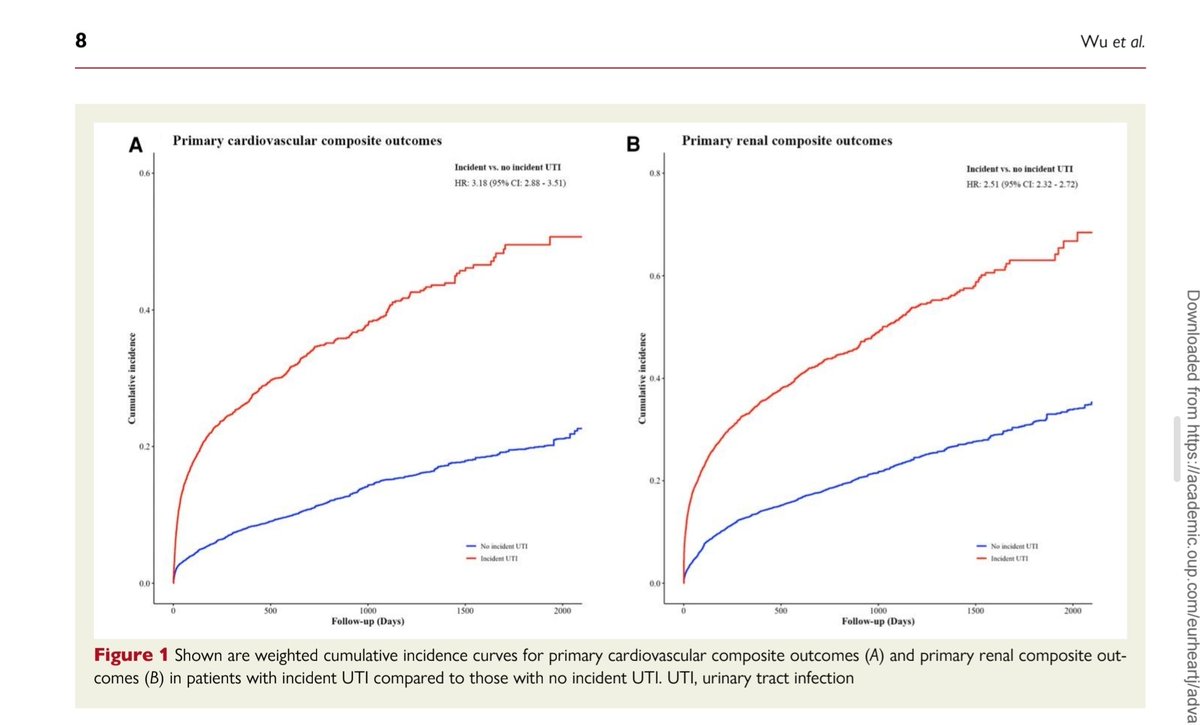
🔍 Key Finding (EHJ, 2025 | doi:10.1093/eurheartj/ehaf788)
In >61,000 T2DM patients on SGLT2i (2015–2022):
🔹 6.3% developed a new-onset UTI during follow-up.
🔹 Those with UTI had markedly higher risks of:
🫀 CV composite events (HR 3.18; 95% CI 2.88–3.51)
💧 Renal composite events (HR 2.51; 95% CI 2.32–2.72)
After UTI, 32% stopped SGLT2i.
🚫 Discontinuation increased:
🫀 CV risk → HR 1.35 (1.20–1.53)
💧 Renal risk → HR 1.35 (1.21–1.51)
💊 No significant reduction in recurrent UTI risk (HR 0.96).
💡 Take-Home Message
🌊 New-onset UTI is a marker of vulnerability — signalling higher cardio-renal risk.
❌ Stopping SGLT2 inhibitors post-UTI worsens CV and renal outcomes, without lowering reinfection risk.
✅ Best approach:
– Treat UTI appropriately 🔬
– Resume or continue SGLT2 inhibitor once infection resolves
– Maintain long-term CV-renal protection 🌿
🩺 Clinical Insight
“UTI is a complication; discontinuation is a setback.”
Keep the molecule — protect the heart & kidney, not just the bladder. 💚
Source:
📘 European Heart Journal (2025): Wu M-Z et al., Urinary tract infection and continuation of sodium–glucose cotransporter-2 inhibitors in diabetic patients.
🔗
https://t.co/Zqy6uCbVCv
Grateful for the opportunity to present a unique and challenging post-kidney transplant case at ISOT, Jaipur.
A special thanks to my mentors @arvindcanchi and Dr Vinod Dibbur for their constant support and guidance.
#ISOT2025
@sgulati2002@isn_india@IndiaSoTx Congratulations!
Here is our paper on desidustat, was alloted an oral podium presentation. We had to change it to a poster presentation since the first author @DrSyeda_hurmath was refused a SChengen Visa. #ERA25
Just wrapped up the ISN Primer Course in Glomerular Diseases at Nairobi-such a fun and enriching experience! Special thanks to @adrianliew8 for the competitive GN Jeopardy which was the highlight: high energy, brain-teasing, and full of learning gems. #ISN#Gloms#Nairobi2025
💫New algorithm proposed for cancer screening, detecting underlying malignancies, & guiding treatment in glomerular diseases—paving the way for more integrated, early detection strategies.
🔗Link to Original article https://t.co/ELL7ijplyr
#Onconephrology#Nephtwitter#CKA