#POCUS image of the day:
Not every pulsatile structure is an artery. 👇
Pulsatile internal jugular vein in severe tricuspid regurgitation.
Courtesy 🔗 doi: 10.1007/s00134-019-05542-z.
@ToruGotoMD Si. De hecho los dibujos sencillos generan una menor carga cognitiva que esquemas y dibujos complejos. Compartirlo con todo el equipo quirúrgico!!! Incluyendo al anestesiólogo. Richard E. Mayer. https://t.co/cAKENvKj3M https://t.co/sR0ZG5Fmhx
Right-heart clot-in-transit & left-heart clot-in-transit. In both cases reported mortality is very high without treatment and remains substantial even with therapy #echofirst
It’s live 🎉
I built a bowel ultrasound masterclass. Here’s why: 🧵
1/ I’m a gastroenterologist. I scan every day IBD patients, acute abdomens, ward emergencies.
2/ Bowel ultrasound saved my patients from unnecessary CTs more times than I can count.
https://t.co/coT0IRKPPB
⬇️
Love this quote 😄
But “precision guesswork”….now upgraded with #POCUS, because seeing beats blind guessing (or even semi-blind with labs alone) 👀
#Nephrology#Medicine
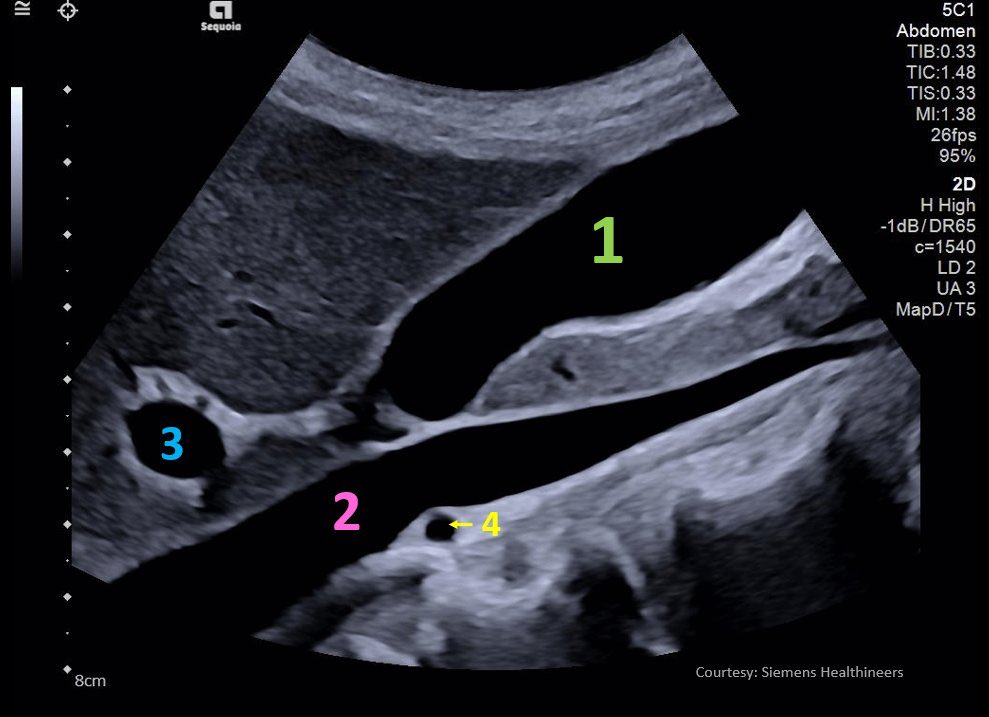
#POCUS image of the day: Continuous sweeping transversal scan performed along the right mid-clavicular line. What do we see here?
#FOAMed#Nephpearls#CriticalCare
Image courtesy: J Clin Monit Comput. 2024, PMID: 38460104.
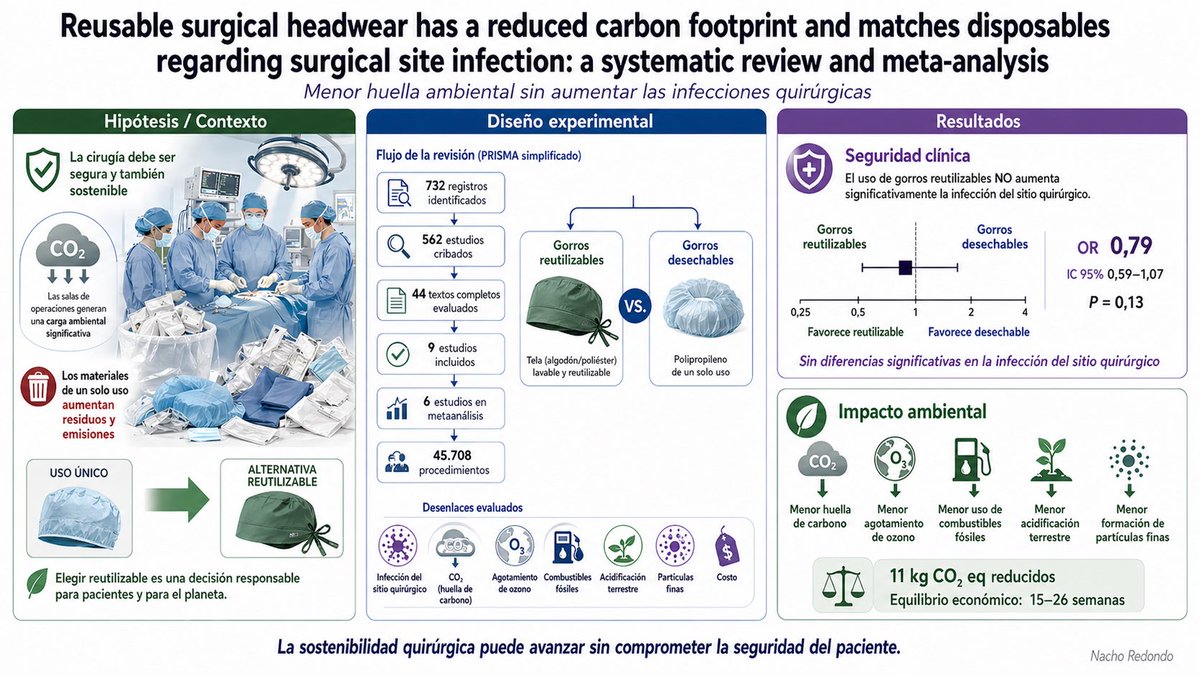
Usar gorros quirúrgicos de tela reutilizables es seguro: este metaanálisis con 45.708 procedimientos no encontró más infecciones quirúrgicas frente a los desechables. Además, reduce impacto ambiental 🌍🏥
DOI: https://t.co/jRPnSyWQsq
#Sostenibilidad#Cirugía#Anestesia
@NephroP@nickmmark In 22% of septic patients, a dynamic left ventricular outflow tract obstruction can occur, increasing mortality in these patients. So remember that sepsis is not just vasoplegia and norepinephrine… doi: 10.1186/s13054-015-0980-z. PMID: 26082197; PMCID: PMC4522114.
🩺 Arterial line ≠ just a number on the monitor
If you’re only looking at MAP…
you’re missing most of the physiology.
🧠 Invasive BP is a real-time hemodynamic language
Every component tells a different story:
▪️ MAP → organ perfusion
▪️ DAP → vascular tone
▪️ SAP → LV afterload
▪️ Pulse Pressure (PP) → stroke volume surrogate
➡️ It’s not one number.
It’s a dynamic physiological system
⚠️ First rule, often ignored:
👉 If the waveform is wrong → everything is wrong
Before interpreting:
✔️ Check damping
✔️ Perform fast flush test
✔️ Look for:
Rapid upstroke
Dicrotic notch
Smooth diastolic decay
➡️ Bad waveform = bad decisions
📉 MAP alone is NOT enough
We target MAP ≥65 mmHg…
but:
▪️ Duration of hypotension matters
▪️ Individual physiology matters
▪️ CVP matters
👉 Think instead:
🎯 Perfusion pressure = MAP − CVP (MPP)
➡️ A “normal MAP” can still mean hypoperfusion
🔥 DAP = your vasopressor trigger
Low DAP = low vascular tone
▪️ Septic shock → ↓ DAP
▪️ Early signal before MAP collapses
👉 Use it to:
✔️ Start norepinephrine earlier
✔️ Avoid delayed vasopressor therapy
➡️ It’s one of the most underused variables in ICU
⚡ Pulse Pressure = hidden CO monitor
PP reflects:
▪️ Stroke volume
▪️ Arterial stiffness
👉 Dynamic changes = key:
✔️ PLR
✔️ Fluid challenge
✔️ Ventilator cycles (PPV)
➡️ You can track CO trends without a CO monitor
🧬 Next-level physiology (very underrated):
New indices:
▪️ DSI = HR / DAP
→ identifies vasoplegia early
▪️ VNERi = DAP / (HR × NE dose)
→ detects norepinephrine resistance
👉 These may define who needs vasopressin early
💡 Mindset shift
Don’t ask:
❌ “What’s the MAP?”
Ask:
✔️ “What is the physiology behind this waveform?”
🧠 Take-home
Arterial line monitoring is not passive.
It’s:
▪️ Diagnostic
▪️ Therapeutic
▪️ Predictive
➡️ If you read it correctly…
it becomes a precision resuscitation tool
📚 Bertrand M et al. (2025)Annals of Intensive Care
DOI: 10.1186/s13613-025-01608-y