Like it or not, the Inflation Reduction Act (IRA) is forcing unprecedented visibility into the 340B program.
@edsilverman of @statnews broke the story that @EliLillyandCo is requiring #340B hospitals to submit claims data or lose access to 340B discounts.
As I told Ed, this is a predictable consequence of the IRA's drug pricing provisions. The law created new pricing obligations for manufacturers, but policymakers never established a reliable way to identify which claims qualify for 340B pricing.
Here's the relevant section from his article:
"The issue has intensified thanks to the Inflation Reduction Act, which imposes a maximum fair price on drugs paid for by Medicare and obligates drugmakers to pay added inflation rebates in Medicare. But the requirement overlaps with the 340B program. Why? Drugmakers must offer hospitals the lower of the maximum fair price or the 340B price — and pay inflation rebates only on drugs not sold at the 340B price.
'The Inflation Reduction Act is forcing transparency into the notoriously opaque 340B program,' said Adam Fein, who heads the Drug Channels Institute and tracks prescription drug pricing and insurance coverage. 'The IRA’s maximum fair price requirements make it impossible to ignore the long-standing lack of visibility into 340B claims.'
He noted, however, that the federal government has not created a mechanism to identify 340B claims, and the HRSA maintains that it lacks the authority to do so. 'The result is a growing compliance dilemma that Congress never intended and regulators have yet to resolve,' he said."
Full article: https://t.co/XTgpm2X6EJ
Congratulations to @GeBaiDC on her nomination to be Assistant Secretary of U.S. Department of Health and Human Services. Ge is exceptionally knowledgeable, thoughtful, and dedicated to improving healthcare. She would be a tremendous asset in this important leadership position.
https://t.co/EQKgdLa1aJ
𝐓𝐡𝐞 340𝐁 𝐂𝐨𝐧𝐭𝐫𝐚𝐜𝐭 𝐏𝐡𝐚𝐫𝐦𝐚𝐜𝐲 𝐌𝐚𝐫𝐤𝐞𝐭 𝐢𝐧 2026: 𝐀 𝐌𝐚𝐭𝐮𝐫𝐢𝐧𝐠 𝐈𝐧𝐝𝐮𝐬𝐭𝐫𝐲 𝐃𝐨𝐦𝐢𝐧𝐚𝐭𝐞𝐝 𝐛𝐲 𝐁𝐢𝐠 𝐂𝐡𝐚𝐢𝐧𝐬 𝐚𝐧𝐝 𝐏𝐁𝐌𝐬
The 340B program was created in 1992 as a narrow policy solution to address an unintended consequence of Medicaid’s best-price provision while supporting core safety-net providers.
But Drug Channels Institute's latest exclusive analysis of the 340B contract pharmacy market shows just how dramatically the program’s current operations and economic incentives have diverged from that original intent.
In 2026, five publicly traded mega-corporations—Cigna, CVS Health, UnitedHealth Group, Walgreens, and Walmart—are capturing 77% of all 340B contract pharmacy relationships.
For the full 2026 market breakdown—including which companies are winning and how the market keeps consolidating—read our latest analysis on Drug Channels:
👇
https://t.co/Mt1u9E5woD
From @Kalderos: 𝐃𝐫𝐮𝐠𝐬, 𝐃𝐢𝐬𝐜𝐨𝐮𝐧𝐭𝐬 𝐚𝐧𝐝 𝐃𝐚𝐭𝐚: 𝐂𝐫𝐚𝐟𝐭𝐢𝐧𝐠 𝐒𝐮𝐬𝐭𝐚𝐢𝐧𝐚𝐛𝐢𝐥𝐢𝐭𝐲 𝐢𝐧 𝐚𝐧 𝐈𝐦𝐩𝐞𝐫𝐟𝐞𝐜𝐭 𝐒𝐲𝐬𝐭𝐞𝐦
Register for "GTN Oversight: A New Standard of Transparency Is Here" (free 6/23 webinar): https://t.co/r6LgQtn05c
Read the article: https://t.co/zzMtTW8Tur
#sponsored
𝐌𝐚𝐫𝐤 𝐂𝐮𝐛𝐚𝐧 𝐖𝐢𝐧𝐬 𝐭𝐡𝐞 𝐆𝐞𝐧𝐞𝐫𝐢𝐜 𝐏𝐫𝐢𝐜𝐞 𝐖𝐚𝐫 (𝐀𝐠𝐚𝐢𝐧) 🏆
For a surprising number of generic drugs, paying cash through @costplusdrugs can be dramatically cheaper than using commercial insurance:
A new article from @AnnalsofIM found:
• For generic prescriptions with out-of-pocket costs above $15, nearly 80% would have been cheaper through Cost Plus Drugs.
• For prescriptions with cost sharing above $100, the median patient cost dropped from $140 through insurance to just $25 through Cost Plus.
Affordability directly impacts adherence and outcomes. Unfortunately, the warped incentives of the U.S. drug channel mean that many insured patients pay MORE than transparent cash pricing.
Small caveat: Less than 5% of generic prescriptions had OOP<$15.
Nonetheless, another reminder from Mark Cuban @mcuban that complexity is the enemy of low costs and efficiency.
Full article
👇
https://t.co/hX4yHnakiR
𝐃𝐫𝐮𝐠 𝐂𝐡𝐚𝐧𝐧𝐞𝐥𝐬 𝐍𝐞𝐰𝐬 𝐑𝐨𝐮𝐧𝐝𝐮𝐩, 𝐌𝐚𝐲 2026: My $0.02 on Optum Rx’s Transparency, Must-Read 340B History, PBM Unbundling Update, PA Delays, and Vegas Fun
Summer unofficially kicked off last weekend. So fire up the grill and enjoy these noteworthy delicacies, seared to perfection on the Drug Channels barbeque:
• Why Optum Rx Is Accelerating Its Transparency Strategy
• The Most Important 340B Paper You’ll Ever Read
• Blue Shield of California’s PBM Unbundling Plan Meets Reality
• Prior Authorization: Administrative Complexity = Delayed Care
Plus: The Drug Channels Institute team takes on Las Vegas—with stickers!
Read all the juicy details here:
👇
https://t.co/HessWVWC3i
𝐓𝐡𝐞 𝐌𝐨𝐬𝐭 𝐈𝐦𝐩𝐨𝐫𝐭𝐚𝐧𝐭 340𝐁 𝐩𝐚𝐩𝐞𝐫 𝐘𝐨𝐮'𝐥𝐥 𝐄𝐯𝐞𝐫 𝐑𝐞𝐚𝐝
If you care about #340B policy, use the long weekend to read this outstanding new paper:
"Stretching Scarce Authorizing Legislation as Far as Possible: A Legislative History of the 340B Drug Pricing Program."
Sayeh Nikpay @saynikpay and her colleagues went back to the early 1990's to reconstruct the program's origins. Their research draws on interviews with 18 key participants and 175 primary source documents spanning 1990–1992.
Their conclusion is difficult to ignore:
340B was originally designed as a narrow policy solution to address an unintended consequence of Medicaid’s best-price provision and to support core safety-net providers.
But the paper makes a compelling case that today’s program extends far beyond Congress’s original intent.
Whether you support or oppose the current structure of 340B, this paper is essential reading for anyone who wants to understand how we got here.
Read it here: https://t.co/MrD8O31wNI
One especially fascinating detail: The disproportionate share hospital (DSH) eligibility threshold of 11.75% was chosen to qualify two specific hospitals and secure bipartisan support from Senator Hatch and Representative Bliley.
In other words, the threshold was not grounded in any broader scientific or policy rationale.
Amazing.
𝐏𝐁𝐌 𝐒𝐡𝐚𝐤𝐞𝐨𝐮𝐭: 𝐇𝐨𝐰 𝐕𝐞𝐫𝐭𝐢𝐜𝐚𝐥 𝐈𝐧𝐭𝐞𝐠𝐫𝐚𝐭𝐢𝐨𝐧 𝐈𝐬 𝐑𝐞𝐬𝐡𝐚𝐩𝐢𝐧𝐠 𝐖𝐡𝐚𝐭’𝐬 𝐍𝐞𝐱𝐭 (𝐕𝐈𝐃𝐄𝐎)
The PBM market is entering a shakeout phase.
In this short video excerpt from DCI’s recent PBM Industry Update webinar, I review:
• The changing market shares of the largest PBMs
• Why many smaller PBMs still depend on the Big Three
• How vertical integration continues to reshape the industry
• Why regulation and scale pressures could accelerate consolidation
We expect the PBM market five years from now to look very different from today.
Watch here
👇
https://t.co/kh6kalPPlx
#PBM #Healthcare #Pharmacy #DrugChannels #HealthPolicy
𝐏𝐢𝐧𝐤 𝐒𝐡𝐞𝐞𝐭: 𝐏𝐁𝐌 𝐑𝐞𝐠𝐮𝐥𝐚𝐭𝐢𝐨𝐧 𝐌𝐚𝐲 𝐁𝐨𝐥𝐬𝐭𝐞𝐫 𝐁𝐢𝐠 𝐓𝐡𝐫𝐞𝐞 𝐌𝐚𝐫𝐤𝐞𝐭 𝐏𝐨𝐬𝐢𝐭𝐢𝐨𝐧 𝐕𝐞𝐫𝐬𝐮𝐬 𝐒𝐦𝐚𝐥𝐥𝐞𝐫 𝐂𝐨𝐦𝐩𝐞𝐭𝐢𝐭𝐨𝐫𝐬
PBM reform may not have the impact many expect.
In a recent Drug Channels Institute webinar, we discussed:
• How new federal transparency rules could disadvantage smaller PBMs
• Why the Big Three are better positioned to adapt
As transparency becomes standard, differentiation shrinks.
As compensation shifts away from list prices, PBMs move toward fee-based models. (Hello, Net Pricing Drug Channel! #NPDC)
The twist: these changes could reduce pressure for further legislation and ultimately strengthen the largest players.
More in The Pink Sheet
👇
https://t.co/4yuwzlU2Sh
#PBM #DrugPricing #HealthcarePolicy
From PHIL: 𝐏𝐫𝐨𝐭𝐞𝐜𝐭𝐢𝐧𝐠 𝐆𝐫𝐨𝐬𝐬-𝐭𝐨-𝐍𝐞𝐭 𝐏𝐞𝐫𝐟𝐨𝐫𝐦𝐚𝐧𝐜𝐞 𝐓𝐡𝐫𝐨𝐮𝐠𝐡 𝐒𝐢𝐧𝐠𝐥𝐞-𝐂𝐡𝐚𝐧𝐧𝐞𝐥 𝐄𝐜𝐨𝐬𝐲𝐬𝐭𝐞𝐦𝐬
Learn more about PHIL’s technology solution for brands: https://t.co/FGHxk0Xefw
Read the article: https://t.co/aAMLtvrUUP
#sponsored
🚨 𝐃𝐫𝐮𝐠 𝐂𝐡𝐚𝐧𝐧𝐞𝐥𝐬 𝐍𝐞𝐰𝐬 𝐑𝐨𝐮𝐧𝐝𝐮𝐩, 𝐌𝐢𝐝-𝐌𝐚𝐲 2026 🚨
Bryce Platt breaks down a timely mix of policy, pricing, and market dynamics:
• Are drug launch price analyses built on flawed assumptions?
• Pharmacy closures are accelerating—new data reveal where and why
• The complex reality of how hospitals are paid for uncompensated care
• Key differences between 340B hospitals and federal grantees
• A fresh (and unexpected) take: specialty pharmacy as a luxury hotel
Dive in:
👇
https://t.co/ipzCxgCpuK
🚨340𝐁 𝐢𝐧 2026: 𝐌𝐚𝐫𝐤𝐞𝐭 𝐒𝐡𝐢𝐟𝐭𝐬, 𝐏𝐨𝐥𝐢𝐜𝐲 𝐁𝐚𝐭𝐭𝐥𝐞𝐬, 𝐚𝐧𝐝 𝐖𝐡𝐚𝐭 𝐓𝐡𝐞𝐲 𝐌𝐞𝐚𝐧 𝐟𝐨𝐫 𝐒𝐭𝐚𝐤𝐞𝐡𝐨𝐥𝐝𝐞𝐫𝐬 (Live Video Webinar) 🚨
The 340B Drug Pricing Program remains one of the most complex—and contentious—parts of the U.S. drug channel.
On June 12 (12:00–1:30 p.m. ET), I’ll be hosting a live webinar where I’ll break down what’s really happening behind the headlines:
• The economics and continued growth of 340B
• DCI’s latest data on contract pharmacy trends and market dynamics
• How PBMs, manufacturers, and distribution strategies are evolving
• Key legal, regulatory, and state policy developments
• IRA implications, rebate model proposals, and oversight challenges
• the growing role of employers and plan sponsors
• Emerging risks and —and what to watch next
• And more
Clear facts. Sharp analysis. Live Q&A.
If 340B affects your business, you won’t want to miss this.
Register 👉 https://t.co/OTVVdcutCQ
#340B #DrugPricing #PBM #Pharmacy #DrugChannels
In 2024, Blue Shield of California promised "$500 million in medication savings” with its widely-praised attempt to unbundle the traditional PBM model across nine different vendors. At the time, I was a bit skeptical. (Link in comments.)
So, how’s it going?
Not so well.
According to this @modrnhealthcr interview with Paul Markovich: "Progress toward major savings is proving more gradual than the company anticipated."
Blue Shield reports $100 million in savings through "lower administrative costs." But last year, Mr. Markovich revealed that the company had already “spent nearly $100 million getting our pharmacy model set up and working.”
So, despite the glowing press coverage in 2024, there's little evidence of net savings (so far).
I remain skeptical that Blue Shield has stumbled upon a viable and scalable alternative to the traditional PBM model.
In anything, the company's misadventures reinforce a lesson often emphasized by Mark Cuban @mcuban :
𝐂𝐨𝐦𝐩𝐥𝐞𝐱𝐢𝐭𝐲 𝐢𝐬 𝐭𝐡𝐞 𝐞𝐧𝐞𝐦𝐲 𝐨𝐟 𝐥𝐨𝐰 𝐜𝐨𝐬𝐭𝐬 𝐚𝐧𝐝 𝐞𝐟𝐟𝐢𝐜𝐢𝐞𝐧𝐜𝐲.
Full interview: https://t.co/n055yftgtX
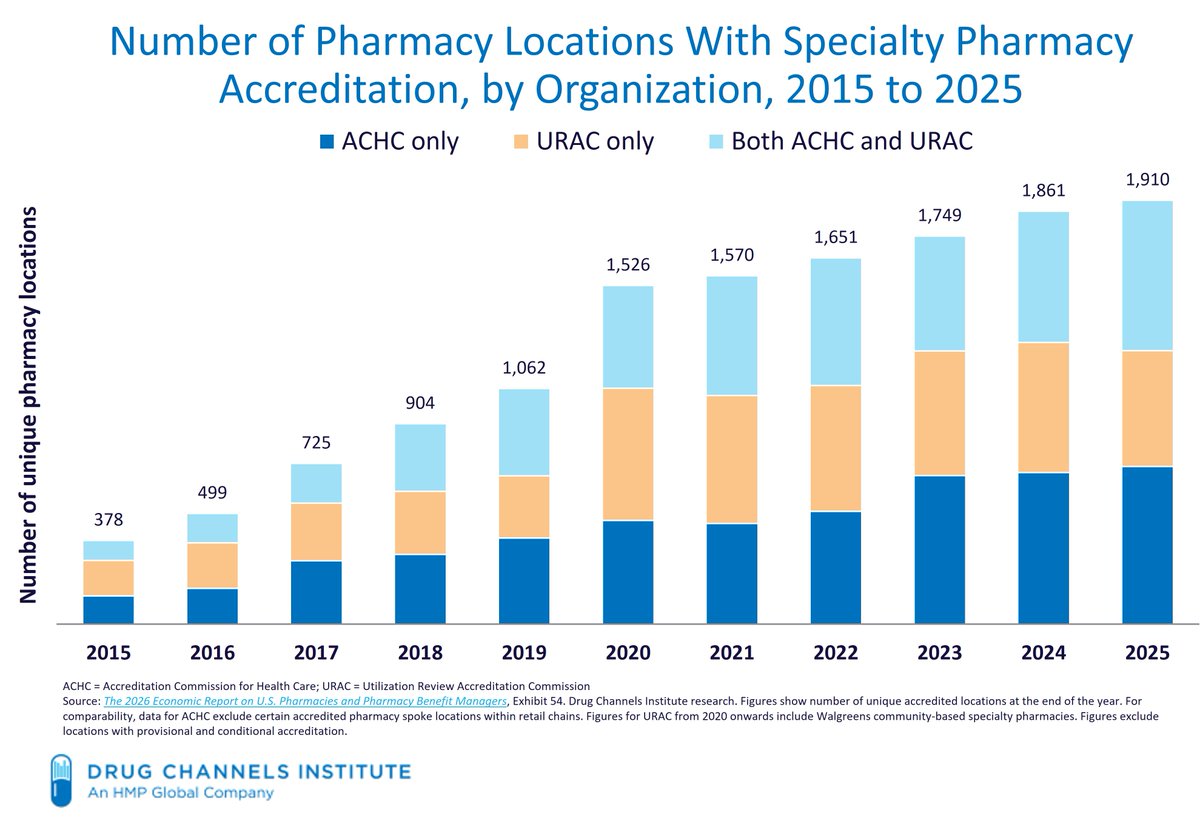
𝐒𝐩𝐞𝐜𝐢𝐚𝐥𝐭𝐲 𝐏𝐡𝐚𝐫𝐦𝐚𝐜𝐲 𝐀𝐜𝐜𝐫𝐞𝐝𝐢𝐭𝐚𝐭𝐢𝐨𝐧: 𝐃𝐂𝐈’𝐬 𝐄𝐱𝐜𝐥𝐮𝐬𝐢𝐯𝐞 𝐀𝐧𝐚𝐥𝐲𝐬𝐢𝐬 𝐑𝐞𝐯𝐞𝐚𝐥𝐬 𝐚 𝐌𝐚𝐫𝐤𝐞𝐭 𝐚𝐭 𝐚𝐧 𝐈𝐧𝐟𝐥𝐞𝐜𝐭𝐢𝐨𝐧 𝐏𝐨𝐢𝐧𝐭
The specialty pharmacy market keeps growing… but not the way you might think.
DCI identified 1,910 accredited locations.
But:
• Growth has slowed
• 40% of pharmacy locations now operated by healthcare providers
• Independents down to 29% share (from 59% in 2015)
• Two-thirds of specialty revenues flow through a few PBM-affiliated giants
Fragmented on the surface. Concentrated underneath.
Read our full analysis:
👇
https://t.co/LqpRzCvGO5
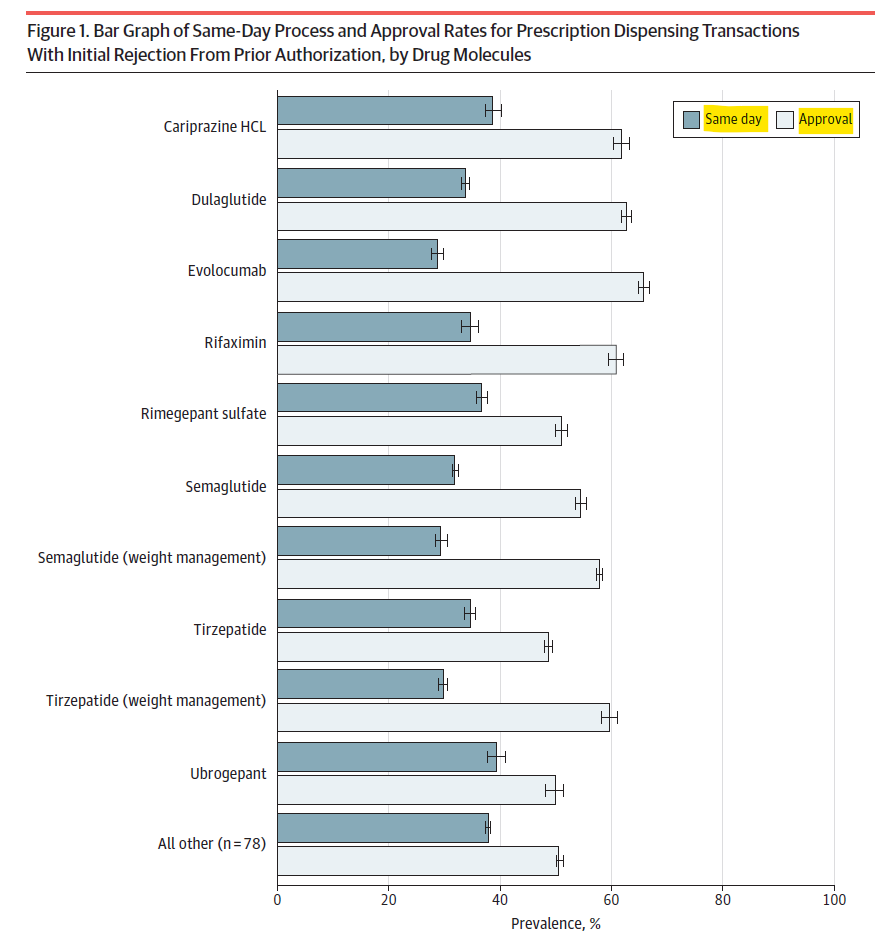
𝐏𝐫𝐢𝐨𝐫 𝐀𝐮𝐭𝐡𝐨𝐫𝐢𝐳𝐚𝐭𝐢𝐨𝐧: 𝐀𝐝𝐦𝐢𝐧𝐢𝐬𝐭𝐫𝐚𝐭𝐢𝐯𝐞 𝐂𝐨𝐦𝐩𝐥𝐞𝐱𝐢𝐭𝐲 = 𝐃𝐞𝐥𝐚𝐲𝐞𝐝 𝐂𝐚𝐫𝐞
New data on ~206,000 brand-name drug #prescriptions with initial prior authorization (PA) rejections:
• Only 35% cleared same day
• 65% delayed (median = 6 days)
• Nearly half (46%) were never approved
Multiple PA reviews and added rejection reasons significantly reduced same-day processing:
• Refills and complex cases were less likely to move quickly
• Medicaid patients and those with multiple conditions had lower approval rates
• Wide variation across drugs highlights uneven access 👇
For many patients, an initial PA rejection means delayed (or no) treatment.
Source: JAMA Health Forum https://t.co/LY2ryRhtmG
From @ConnectiveRx: 𝐖𝐡𝐞𝐫𝐞 𝐆𝐫𝐨𝐬𝐬-𝐭𝐨-𝐧𝐞𝐭 𝐏𝐫𝐞𝐬𝐬𝐮𝐫𝐞 𝐀𝐜𝐭𝐮𝐚𝐥𝐥𝐲 𝐋𝐢𝐯𝐞𝐬 𝐀𝐟𝐭𝐞𝐫 𝐋𝐚𝐮𝐧𝐜𝐡
Register for "Gross-To-Net FOMO: What GTN Dangers Are You Missing Post-Launch?" (free webinar): https://t.co/SXA6zp2AgE
Read the article: https://t.co/tlKFZCmutD
#sponsored
🚨 𝐃𝐫𝐮𝐠 𝐂𝐡𝐚𝐧𝐧𝐞𝐥𝐬 𝐍𝐞𝐰𝐬 𝐑𝐨𝐮𝐧𝐝𝐮𝐩, 𝐀𝐩𝐫𝐢𝐥 2026🚨
Are PBMs steering patients? Are insurers shifting profits? And what’s really behind hospitals’ “fake prices”?
This month’s roundup tackles some of the most contentious issues in today’s drug channel:
• PBM-affiliated specialty pharmacies: New data shows major differences in patient access—and raises tough questions about steering
• MLR profit shifting: Fresh evidence that vertically integrated insurers may be moving margins within Part D
• Nonprofit hospitals: A provocative look at the widening gap between mission and financial reality
Plus: A behind-the-scenes look at how we build a DCI webinar
Read the full roundup here
👇
https://t.co/2NJHmf9VOg
𝐇𝐨𝐬𝐩𝐢𝐭𝐚𝐥𝐬 & 𝐓𝐡𝐞𝐢𝐫 𝐅𝐚𝐤𝐞 𝐏𝐫𝐢𝐜𝐞𝐬
A must-read, hard-hitting piece from Anthony DiGiorgio @DrDiGiorgio on the economics of nonprofit hospitals and the growing gap between their public mission and financial reality.
He lays out the extensive subsidy ecosystem supporting hospitals:
• Property and sales tax exemptions
• Public funding (DSH payments, GME, research support)
• 340B Drug Discount Program revenues
• Market power–driven pricing from consolidated health systems
…among others
Then comes the key question:
"After all of those subsidy streams, what exactly is still unfunded"?
As he puts it, hospitals should provide a true accounting:
• What is the net Medicaid shortfall after supplemental payments?
• What is the real value of tax exemptions?
• Where does 340B revenue actually go?
• How are funds allocated across executive pay, administration, expansion, reserves, M&A, and lobbying?
Until we see that level of transparency, claims about underfunding deserve more scrutiny.
Strong, provocative piece.
👉 https://t.co/EJZ8DAHOQL