Need help!
Where can I learn how to make better slides for my talks? I know what good slides look like just don’t know how to execute #FOAMed#MedTwitter
@AnnaGaddy @emily_fri I wonder if some disclosure at the beginning of your M&M saying that this is a part of a formal quality review process would protect that. I think you could argue M&M is part of a formal QI process esp if your department has a formal QI plan and M&M is somewhere in it.
We wonder why LPs are so uncomfortable for patients and then put a 3cc syringe and tiny needle in the kit for providers to use when providing local anesthesia. I can think of two easy fixes that I bet would help at least somewhat with pt comfort
Hey @_JaceMullen I just wanted you to know that I still think this is one of the best blog posts on the internet and I still make every paramedic student read it. @FOAMfrat
https://t.co/2xCTqhuX08
Hey #EMS#educators: ever taught a lesson that didn't result in the change you intended? How do you design ed that works? Here's the latest episode from The EMS Educator podcast w/ guest @EMtgDO. @ReadyMKE @maiadorsett@UKROBL1@gateshil@MedicalCollege https://t.co/eGcx09x2eo
@DrJeffJarvis I struggle w/ how interventions with minimal/no evidence are added into EMS guidelines and then observational data is used to support the change. How many interventions showed no benefit and then were pulled w/o publication? pts could have been harmed by “progressive” guidelines
@ssk040 I think it’d be irresponsible to not review your pcg given what happened. Any quality case, even if it isn’t yours, should cause you to make sure what ur doing is standard. If u r making changes bc you were using old terms and unsafe practices from years ago there’s a problem
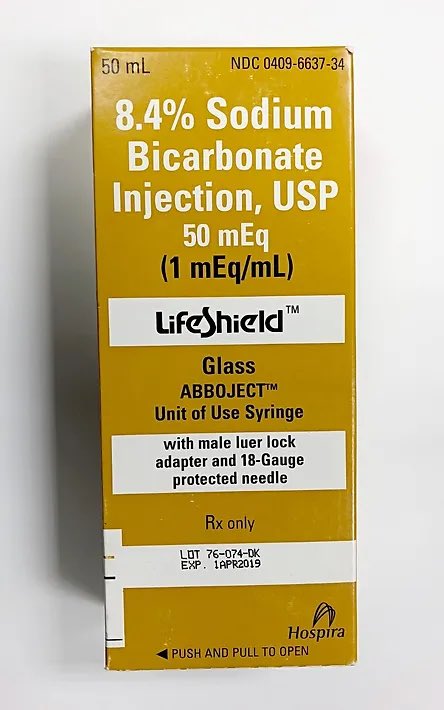
You've probably heard that Bicarbonate has to turn into CO2 to raise the pH. “Don’t give bicarb if you can’t increase ventilation.”
But how much CO2 is there in an amp of sodium bicarbonate?
A bicarb 🧵
1/
@jwoodard_md @AmerGeriatrics Curious about checking orthostatic vitals. A lot of the EM literature says these aren’t helpful. What’s the lit saying on your side? What do you use them for in delirium?
@fyreman2006@JonEMTP@dkirch888 I’d say many physicians probably haven’t yielded a syringe in many years depending on specialty so the more idiot proof these can be the better. Many people who might be helping out have little to no experience actually drawing up meds.
1983 study from Milwaukee Co EMS showed the use of calcium in cardiac arrest reduced ROSC from 38% to 10% & concluded its use was “highly suspect.” Paper is great but so old you can’t find it online! -M. Frakes #CCTMC23
@_JaceMullen "Well, we'd tube them but since their mouth opening sucks we'll just place an SGA" or "We'd tube them but since their mouth opening sucks we can just BVM them." I think a good airway assessment helps you pick the right airway strategy for the right patient.
@_JaceMullen I think I get what you're trying to say but your tweet is worded weird. Considering all EMS airways as difficult is great but your 2nd phrase sounds like you're arguing an airway assessment shouldn't be utilized to determine airway mgmt strategy which I doubt is your point.
Doctors are going to sell to PE, that’s not going to stop, but that decision should preclude appointment to leadership positions in organizations which exist to advocate for physicians and patients.