Interesting question.. using 22.5 Gy/3 for lesions < 1 cm and 27.5/5 > 1 cm we have achieved LC around 81% at 1 year without G3 toxicity. The question is if we can use these dose in combination with systemic treatments (immuno, ADCs)
New in #practicalRO: Effectiveness of Regional Nodal Irradiation in Women with a Pathologic Complete Response in the Nodes After Neoadjuvant Chemotherapy with Residual Disease in the Breast. https://t.co/gtYT5RRRB3
SBRT to oligometastatic lesions consistently delays ADT, improves PFS, and in some trials cuts biochemical recurrence.
Phase III data is still maturing. Patient selection varies. Imaging definitions differ. @NatRevUrol@OncoAlert@APCCC_Lugano
This study evaluated the effectiveness of a peer-review process to objectively assess the skills of radiation oncology (RO) resident physicians (RPs) in contour grading of head and neck (HN) malignancies.
Learn more 🧠 https://t.co/7qSf1p9I9i
#RadOnc#RadiationOncology#HNC #HeadandNeckCancer #HeadandNeckCancerAwarenessMonth #ResearchArticle #RadOncEd
New decision analysis: For rectal cancer patients with complete response after chemoRT, choosing surgery over "Watch & Wait" costs ~9 QALYs - almost a decade of perfect health - lost to permanent toxicity (LARS, sexual dysfunction, stoma)
El XXIII Congreso Nacional SEOR 2026 contaremos con la participación del Prof. Steven Frank @SJFrankMD en la sesión magistral: Proton Therapy: new paradigm in the treatment of oropharyngeal cancer
Alicante | 📅 3–5 junio 2026
🔗 https://t.co/SYnFPSz5Fc
#SEOR2026 #OncologíaRadioterápica #Protonterapia
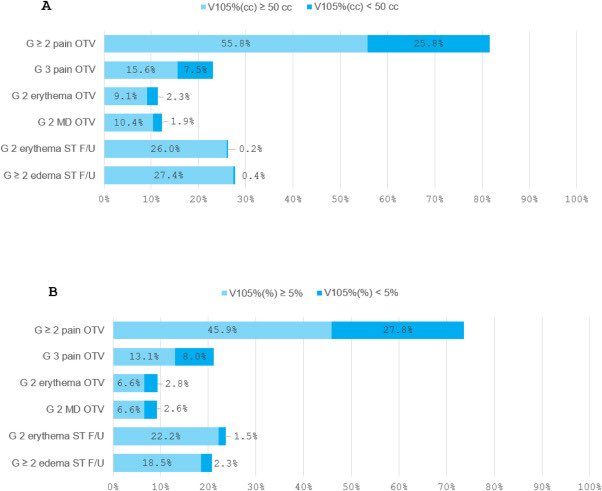
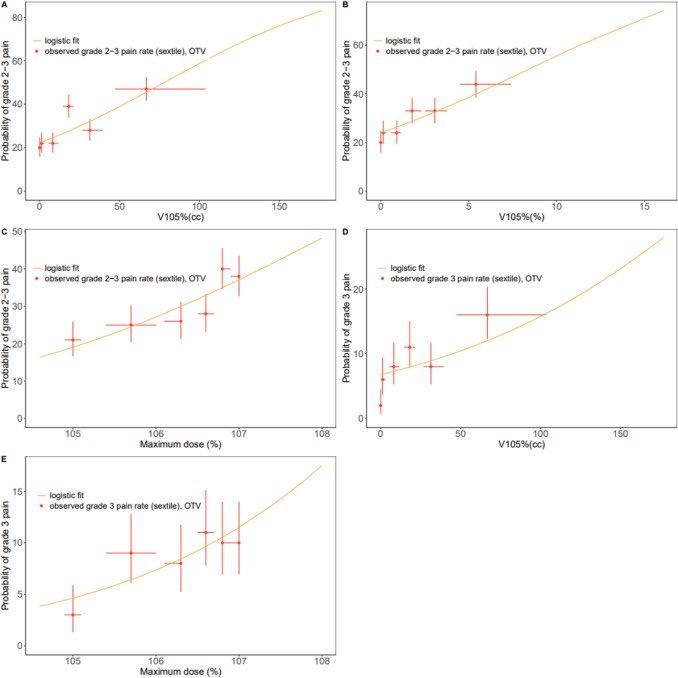
📌 Dosimetric Correlates of Acute Toxicities for Moderate Hypofractionated Whole Breast Irradiation: Implications for ASTRO Planning Guidelines ☢️
🔗 https://t.co/zwENRe7nAU
@VishrutaD@JulianaRunnels@MountSinaiRO@ASTRO_org#BreastCancer#RadOnc
🔸 600 patients treated with HF WBI (42.56 Gy in 16 fractions or 40.05 Gy in 15 fractions) between 2018 and 2023 using 3D conformal field in field planning.
🔹 V105 % (cc) ≥ 50 cc and V105 %(%) ≥ 5% were strong, independent predictors of pain and other grade ≥ 2 toxicities
🔸 Keeping V105%(cc) < 50 cc and V105%(%) < 5% markedly reduced toxicity rates, supporting incorporation of relative dose-volume metrics into future guideline updates.
🔹 Optimizing dose homogeneity remains essential to improving patient comfort and quality of life
"Como los días a tu lado son de fantasía, te doy este totem.
Así siempre sabremos que esta felicidad no es un sueño, sino la realidad que estamos construyendo."
Excellent commentary on the LU005 results just out in @JCO_ASCO.
💡 Key insights on the optimal timing of ICIs with RT across multiple tumor types, specifically regarding general avoidance of simultaneous initiation of ICI with standard RT.
📊 Includes a high-yield table with results from multiple randomized Ph 2/3 trials and highlights the importance of correlative studies for future combinations.
🔗 Commentary: https://t.co/WLgeD3dMsj
🔗 LU005 Paper: https://t.co/ZnSvy5cb0c
@KatiekeaneMD@AdamJSchoenfeld #RadOnc
Científicos del MIT demostraron que las ondas de WiFi son capaces de detectar personas, posiciones e incluso posturas corporales, sin necesidad de cámaras. 📡
Las señales rebotan en el cuerpo y regresan alteradas, permitiendo que una inteligencia artificial trace siluetas tridimensionales y reconozca posturas humanas con notable exactitud.
Este avance podría revolucionar la atención médica, la seguridad doméstica y la asistencia a personas mayores… pero también despierta un nuevo temor: ¿qué pasará cuando la red que te conecta sea la misma que te observa? 👁️⚡
#RadOnc history lesson! The first patient treated with the linear accelerator at Stanford in 1957 (at 2 yrs old) was cured of his cancer, and is still alive (as of 2024). He developed a osteosarcoma in the 1980s and received re-treatment w/ heavy ion RT. Link below for reference.
In locally advanced rectal cancer, short course RT (25 Gy/5 fx) was less immunosuppressive than long-course RT, despite more advanced disease. SCRT showed faster lymphocyte recovery, lower NLR and higher intratumoral CD8+ and FOXP3+.
This immune preserving profile provides a biological rationale for SCRT-based radio-immunotherapy strategies.
https://t.co/Rfd0Hhd3d0 @OncoAlert
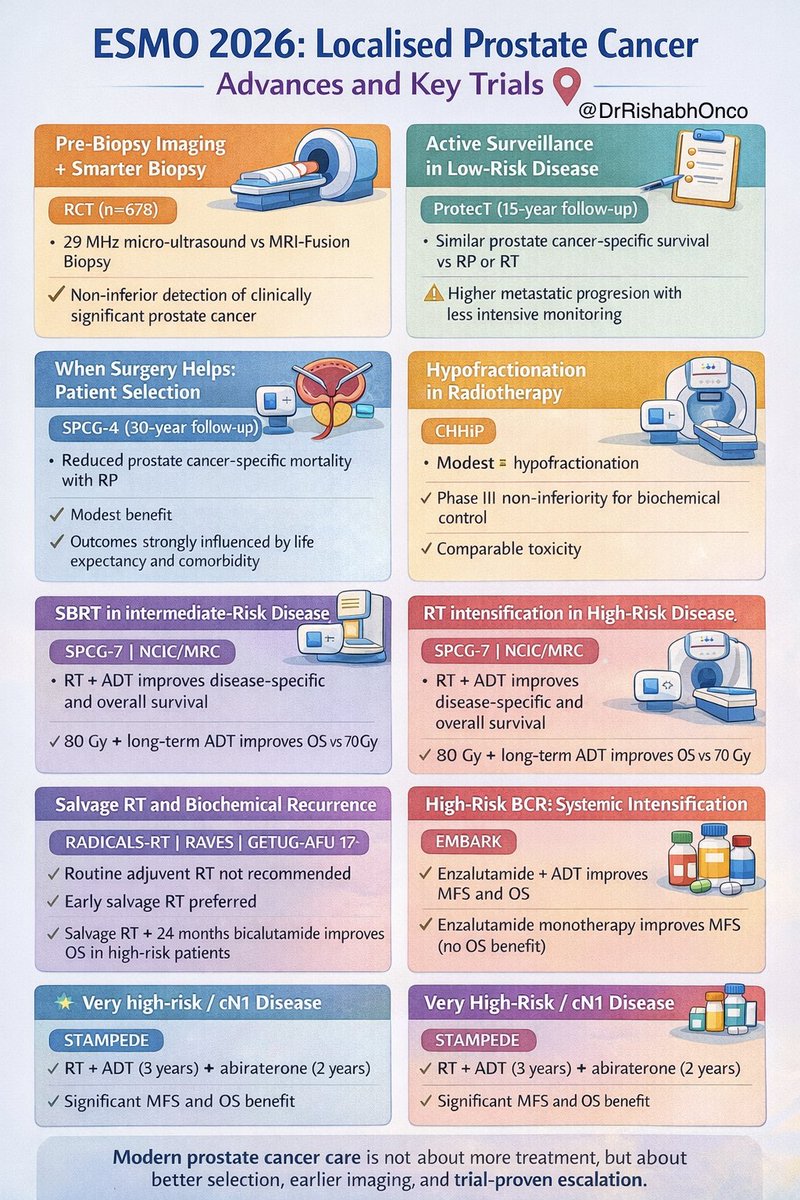
Localised prostate cancer just changed. Again.
ESMO 2026 brings clarity on who to observe, who to escalate, and which trials actually matter 👇
🧠 Diagnosis
MRI before biopsy is standard
High-resolution US is a valid alternative (RCT n=678)
🧭 Low risk
Active surveillance is safe
ProtecT 15-yr data shows similar survival vs RP/RT
☢️ Radiotherapy
Shorter is better
CHHiP ➜ moderate hypofractionation
HYPO-RT-PC ➜ ultra-hypofractionation
PACE-B ➜ SBRT works in selected IR disease
📈 High risk
RT + long-term ADT saves lives
SPCG-7 | NCIC/MRC
Dose escalation improves OS (GETUG-AFU 18)
🚨 Very high-risk / cN1
RT + ADT + abiraterone is the new benchmark
STAMPEDE delivers MFS + OS benefit
🔁 Biochemical recurrence
Avoid routine adjuvant RT
Early salvage RT preferred
RADICALS-RT | RAVES | GETUG-AFU 17
High-risk BCR? Intensify
EMBARK supports enzalutamide + ADT
🧠 Bottom line
Risk-adapted care > overtreatment
Imaging-driven decisions
Escalate only when trials prove benefit
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #ProstateCancer #GUOncology
@OncoAlert@myesmo@esmo_open@asco@OncBrothers
El sábado compartí esta charla sin expectativas.
Los mensajes recibidos estos días me han recordado algo importante 👇
❌ No va de llegar más alto ⬆️
✅ Va de mantenerse fiel a lo que uno es 🧭
La dejo de nuevo por aquí 👇🎥
https://t.co/xyV6f5fH6H
Salvage metastasis-directed therapy vs elective nodal #radiotherapy for oligorecurrent nodal #prostatecancer metastases (PEACE V-STORM) published in the @TheLancetOncol.
👉 Read it before your patients: https://t.co/eCCQDjSyre
@piet_ost@Mat_Guc