1/Do radiologists sound like they are speaking a different language when they talk about MRI?
T1 shortening what? T2 prolongation who?
Here’s a translation w/an introductory thread to MRI.
🫀🔥 LDL is down. Therapy is optimal. And yet… plaque is still growing.
Report from the presentation of the HURRICANE study at the ECR2026
Proud to be part of this study that sheds more light into a very hot contemporary topic.
That’s the uncomfortable reality highlighted by new data presented at ECR 2026.
👉 Statins were working.
👉 Guidelines were followed.
👉 LDL was controlled.
And still:
📈 Atherosclerosis progressed.
💡 This is the blind spot we’ve been ignoring:
👉 Residual cardiovascular risk
Driven by:
✔��� Inflammation
✔️ Metabolic factors
✔️ Genetics
👉 Things LDL alone does NOT capture
🚀 Enter Photon-Counting CT (PCCT)
For the first time, we can:
✔ Quantify plaque volume
✔ Differentiate plaque components
✔ Track progression over time
👉 Not just detect disease…
👉 Measure its evolution
⚠️ And this is where it gets disruptive:
Patients who are “well-controlled” on paper
may still be:
👉 biologically active
👉 progressing silently
🧠 This changes the entire paradigm:
❌ Treat LDL → assume success
➡️ becomes
✅ Treat disease → verify with imaging
🎯 Clinical implication
We may need to move from:
Lipid targets
➡️ to
Plaque targets
From:
Surrogate biomarkers
➡️ to
Direct disease measurement
🚨 Bottom line
Statins treat risk.
👉 PCCT shows reality.
And sometimes…
they don’t match.
⚡ The future is not:
“Did we lower cholesterol?”
It’s:
👉 “Did we actually stop the disease?”
🧠 We optimized the stent. We forgot the disease.
Two major NEJM trials just dropped.
Both asked the same question:
👉 Does IVUS-guided PCI improve outcomes vs angiography alone?
The answer?
❌ No.
📊 Trial #1 – Complex High-Risk PCI (IVUS-CHIP)
IVUS: 13.9% events
Angio: 11.1% events
HR 1.25 → trending worse
📊 Trial #2 – Left Main PCI (OPTIMAL)
IVUS: 33.7% events
Angio: 30.9% events
HR 1.11 → no difference
Let’s be honest.
💡 IVUS did exactly what it’s supposed to do:
✔️ Better sizing
✔️ More post-dilation
✔️ More “optimized” stents
And yet…
👉 No clinical benefit.
⚠️ This is the uncomfortable truth:
We’ve been chasing procedural perfection,
thinking it would translate into patient outcomes.
It doesn’t
(and yes I know the comparator is highly skilled PCI operators/centers; but does this appears as inclusion criteria?)
Because events are NOT driven by:
❌ stent expansion
❌ lumen gain
❌ apposition metrics
They are driven by:
🔥 plaque biology
🔥 disease burden
🔥 patient-level risk
Even more interesting:
👉 The “inferior” arm (angiography) was already excellent
👉 Modern PCI is already optimized
👉 There’s very little left to gain mechanically
💥 So what did these trials really show?
Not that IVUS is useless.
But that:
👉 The paradigm is wrong.
🧬 We are:
✔️ optimizing millimeters
✔️ while events come from microns of biology
🚨 The future is NOT:
“optimize the stent more”
It is:
👉 identify disease earlier
👉 quantify plaque, not stenosis
👉 treat-to-plaque, not treat-the-lumen
💬 Final thought:
We spent 20 years perfecting PCI.
And almost none of that effort touched the disease that actually kills patients.
#Cardiology #PCI #IVUS #CardiacImaging #PhotonCountingCT #PreventiveCardiology #TreatToPlaque
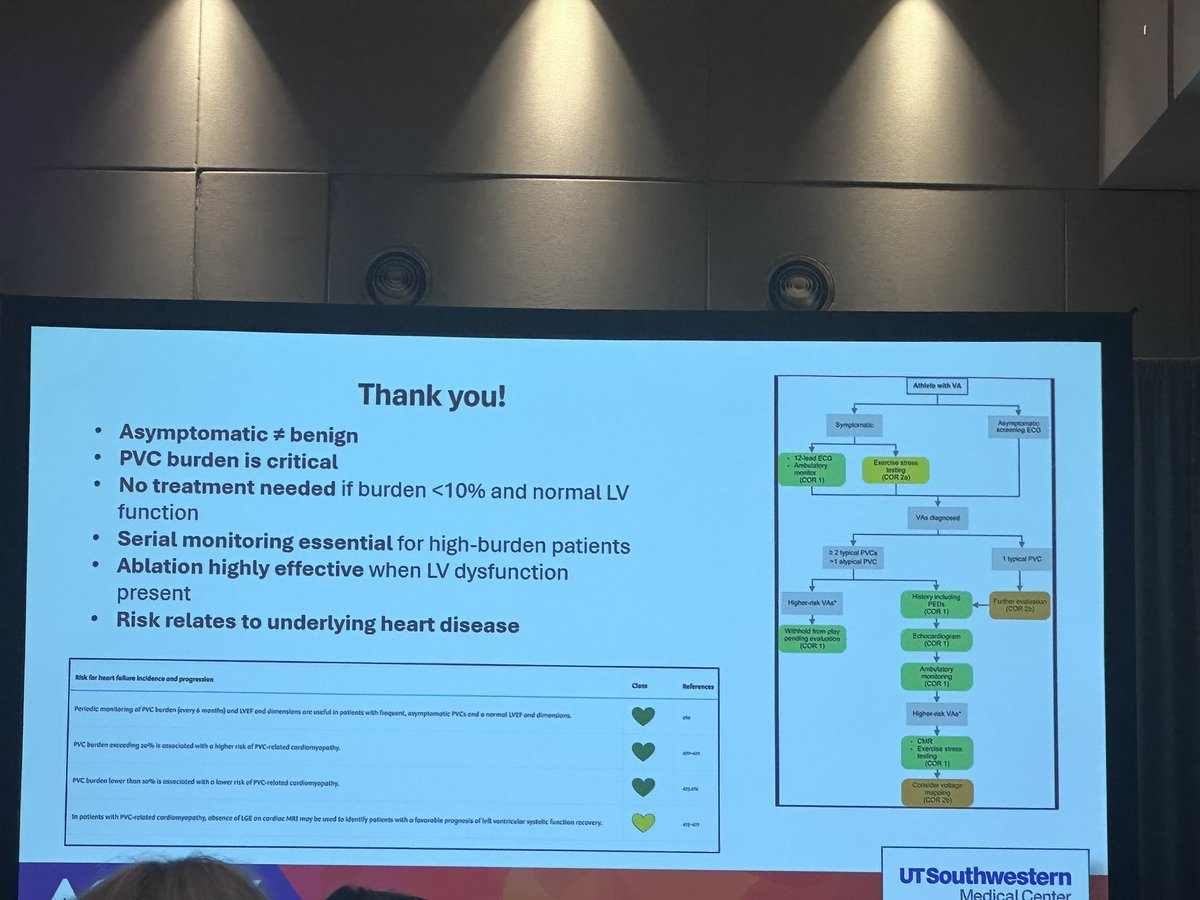
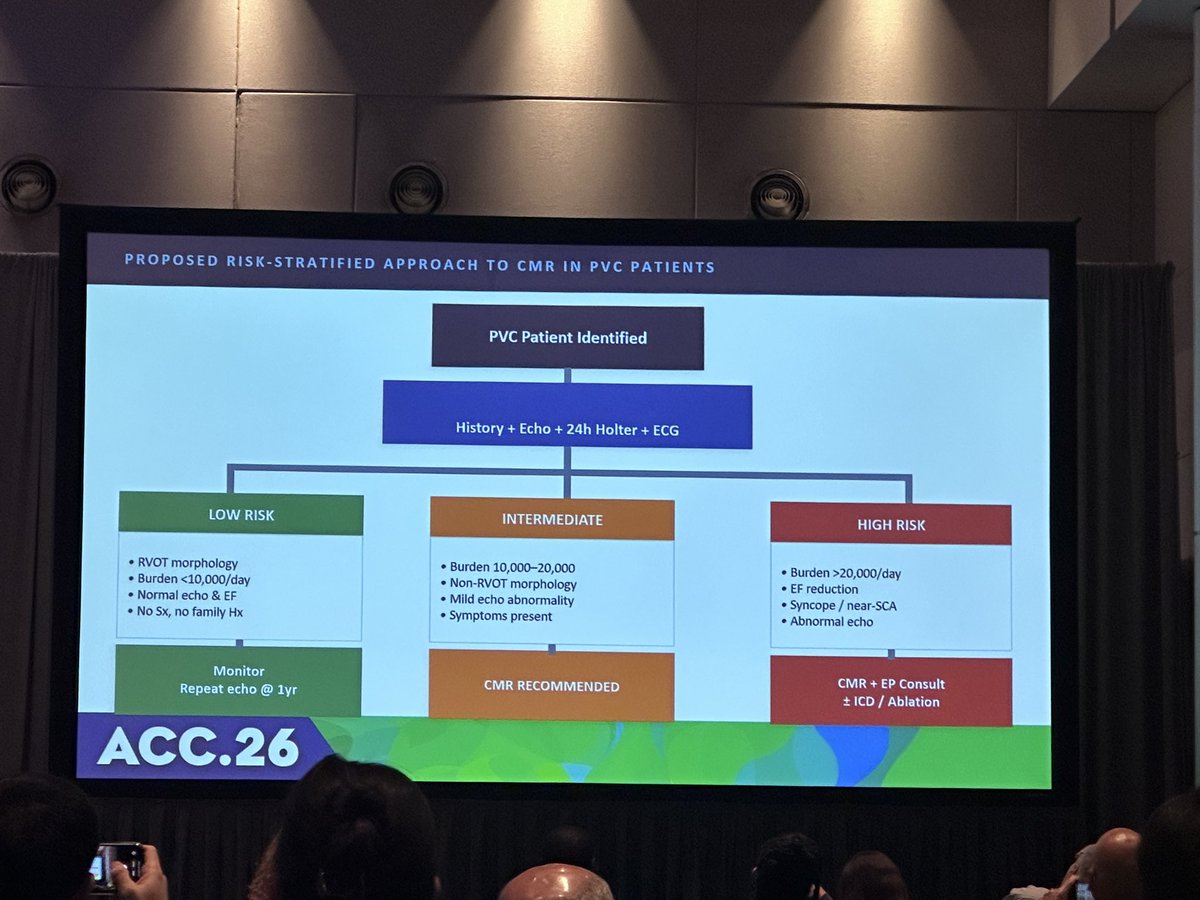
What a wonderful session on PVCs at #ACC26 ⚡🫀
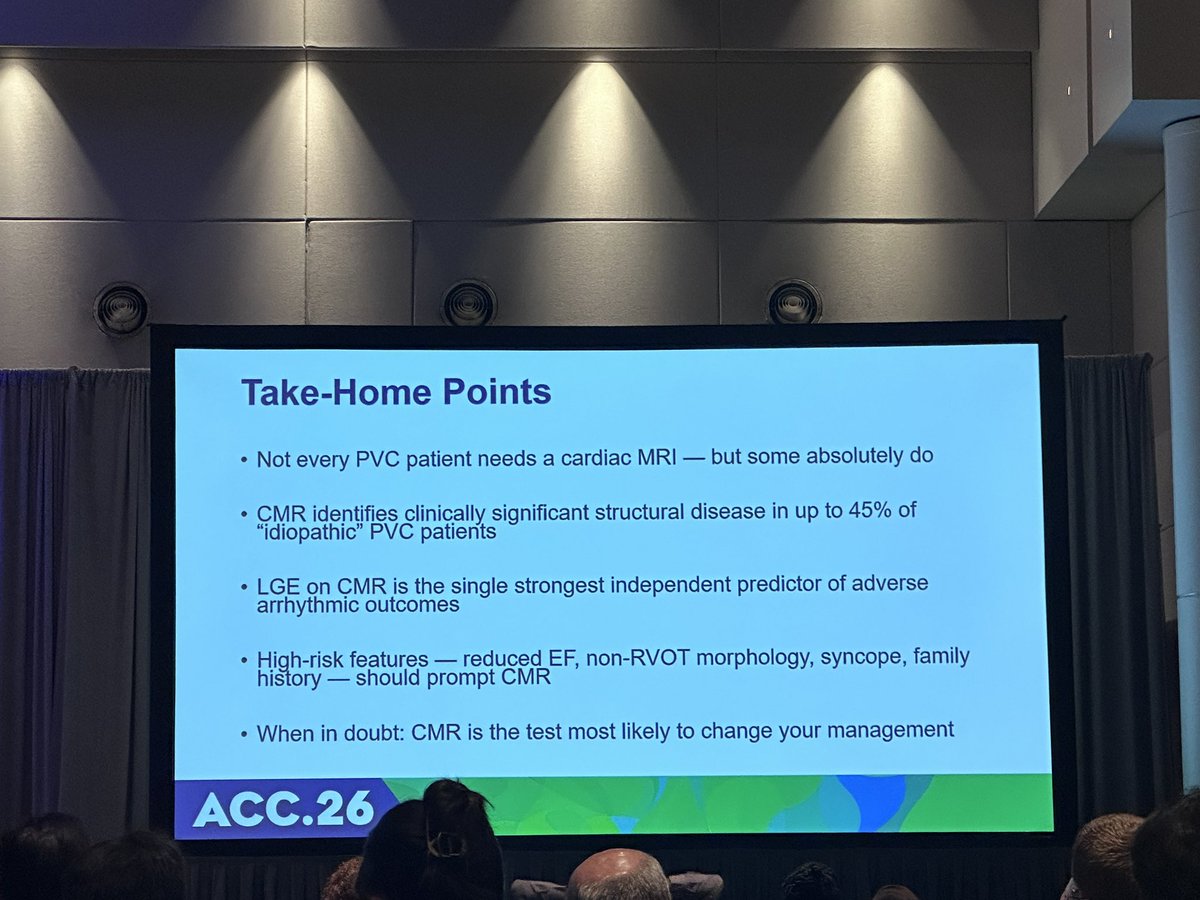
❓Should every patient with frequent PVCs get a cardiac MRI?
❓What to do with Asymptomatic PVCs?
Key insights below 👇
#CardioTwitter#EPeeps#ACCEP
Just published: 📄 protocol of the Mexican Cardiogenic Shock Registry (REMECHOQUE). A national, multi-institutional collaborative effort with impact across Mexico and Latin America.
@ErasmoPA@GTorreAmione@TecSaludMX@TecCardiology
https://t.co/b481mHydDK
@TwindadFrank@Artedeingenio Same question, Found this
In AI image generation, SREF stands for Style Reference.Used in platforms like Midjourney that allows users to apply overall artistic aesthetic (colors, textures, lighting, etc.) of a reference image or a specific numerical code to their generated images
Wrapping up two inspiring days in Cancun at the 3rd Cardiogenic Shock LATAM Symposium!
An incredible gathering dedicated to one of cardiovascular care’s greatest challenges.
Grateful to our speakers & participants for driving collaboration, innovation, and progress in CS
Fellows and early careers: Please submit you challenging CS case and get a chance to win a trip to present it in person this year at the Cardiogenic Shock LATAM Symposium in Cancun, Mexico.
@TecSaludMX@cardiotecdemty@TecdeMonterrey
It was an honor to lead the Cardiogenic Shock Symposium with TecSalud at #CITIC2025—bringing together top national & international experts to tackle one of the biggest challenges in cardiovascular care.
Thanks to the organizing committee!
See you at #CITIC2026.
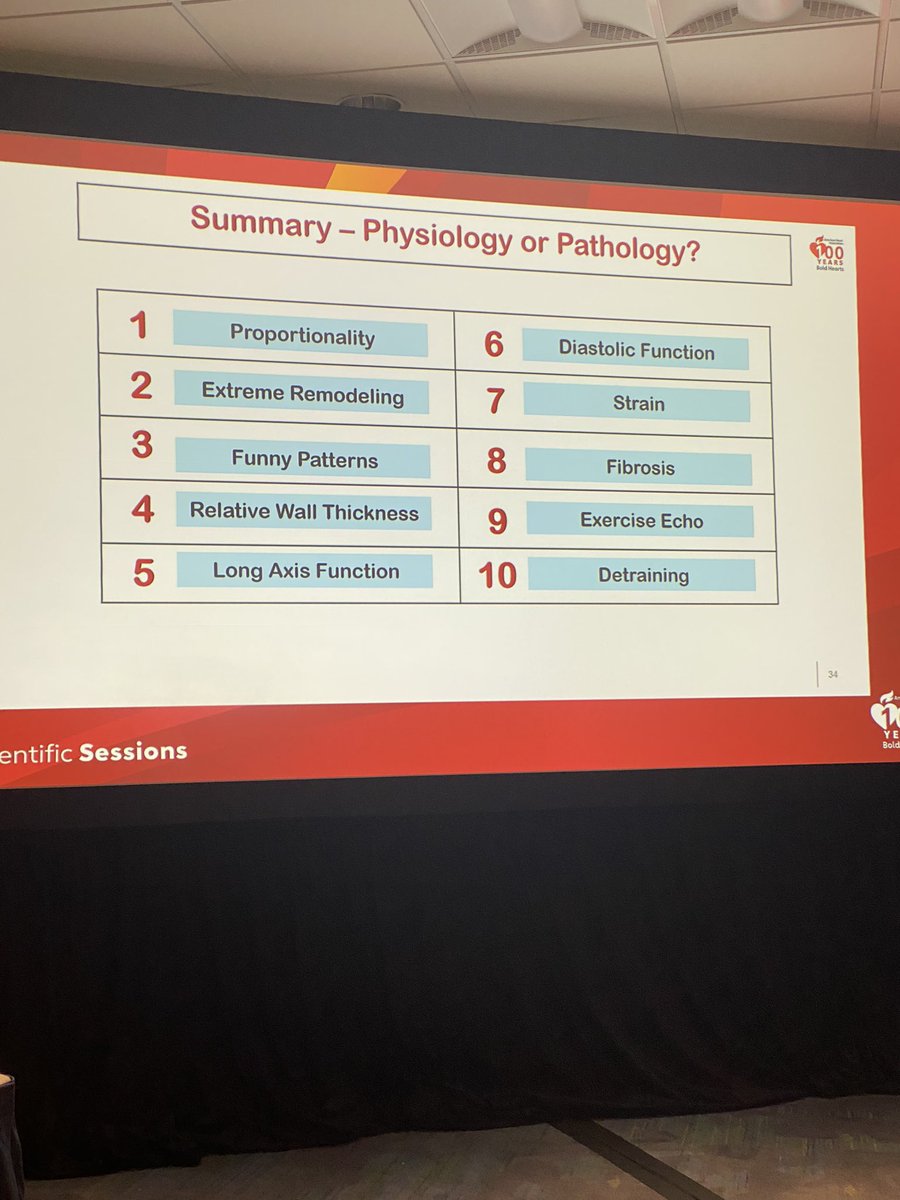
Thank you Dr Abbas Zaidi from Wales, UK. Probably the best talk that I have ever heard on imaging features that distinguish #Athlete#Heart from #cardiac#disease! Was worth staying here @AHAScience#AHA24 for the final session to hear his talk. 🤗