Can sirolimus eluting balloons redefine complex #PCI strategies?
In this interview, @Simoneccles66 discusses with @gmcioffi about the evidence from the SELUTION DeNovo trial and the evolving role of drug-eluting balloons in complex coronary interventions. 🫀📈
#EuroPCR #interventionalcardiology
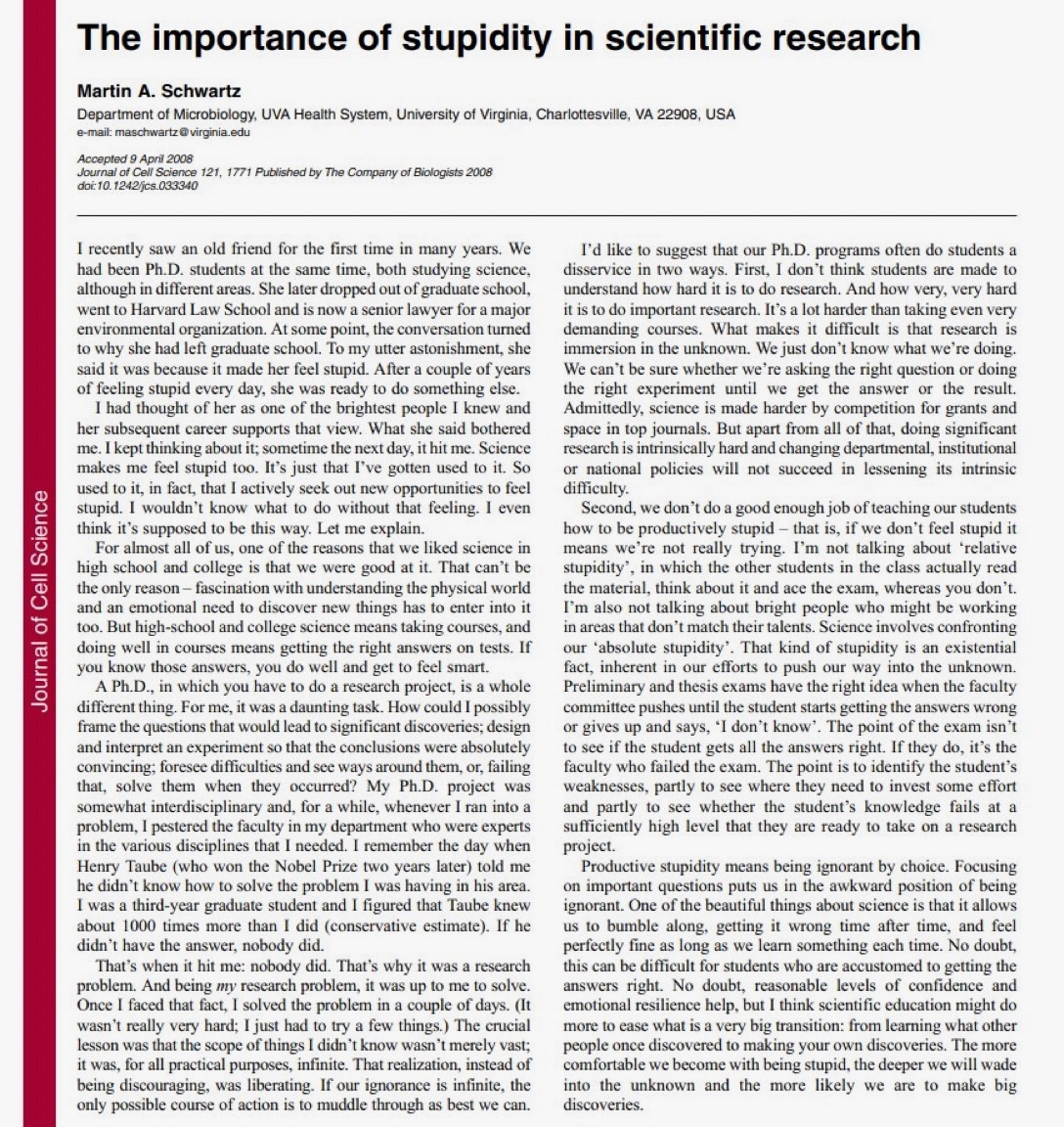
This article should be mandatory reading for every medical student, PhD candidate, researcher—and honestly, for anyone who mistakes expertise for certainty.
“The importance of stupidity in scientific research” sounds provocative, almost offensive. But Martin Schwartz is not glorifying incompetence. He is describing the real operating system of discovery.
Science is not built on knowing.
Science is built on tolerating not knowing.
That distinction matters.
Most of education rewards correctness.
School teaches us to answer.
Exams reward speed, certainty, and precision.
You feel intelligent when you get things right.
Research is the opposite.
Real research begins exactly where competence ends—at the frontier where nobody knows the answer, including the people you thought must know.
That moment is psychologically brutal.
You ask the expert.
The expert shrugs.
You assume you’re missing something.
Then you realize: no—this is the work.
You are not failing.
You are standing at the actual boundary of knowledge.
That feeling—“I must be stupid”—is often not a sign of inadequacy.
It is often the first sign that you are finally asking an important question.
Medicine struggles with this.
We train doctors to avoid uncertainty, to fear being wrong, to perform confidence.
But the best clinicians and the best scientists know how to sit inside ambiguity without collapsing into fake certainty.
This is why AI in medicine also deserves caution.
Systems trained only to reproduce established answers may become extraordinarily good at passing exams while being terrible at discovering what matters next.
Guideline intelligence is not the same as scientific intelligence.
Discovery requires productive stupidity:
the willingness to stay with the uncomfortable,
to look ignorant,
to ask naïve questions,
to be wrong repeatedly without protecting your ego.
Most people want the authority of expertise.
Very few want the humiliation required to earn it.
But progress lives there.
Not in certainty.
Not in performance.
Not in sounding smart.
In the quiet discipline of saying:
“I don’t know… yet.”
And continuing anyway.
10/ My last and most important message
It isn't just your hard work that built your interventional career- it's also the sacrifice, blood and sweat of those who love you
By far the best evidence for short term safety of DCB compared to DES in a real world setting imo, well done @CorballisTash and the team. @Simoneccles66
https://t.co/9z6kCWtCz6
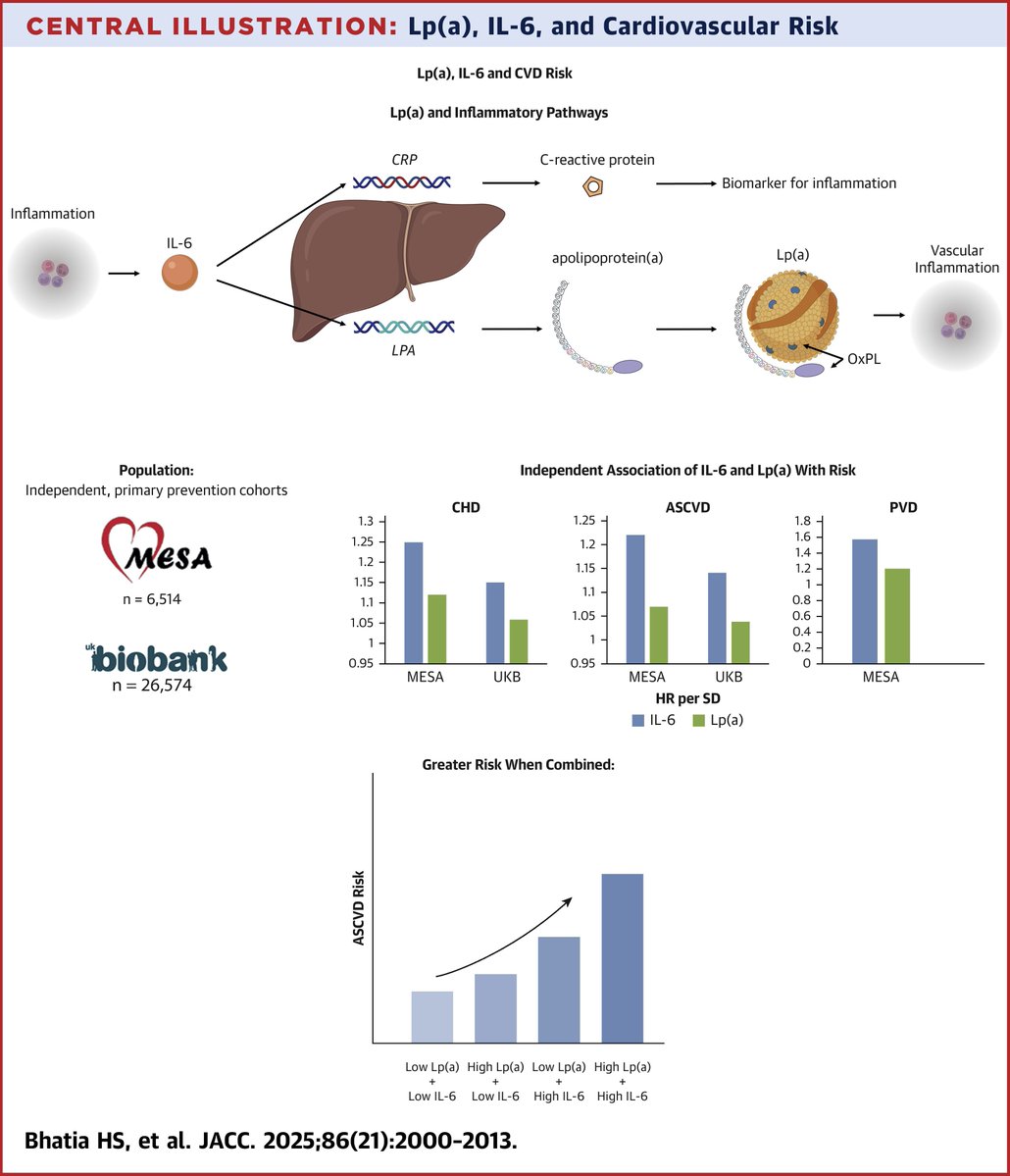
In 2 independent primary prevention cohorts, Lp(a) and IL-6 were independent predictors of #ASCVD risk, and their combination identified individuals at the highest risk. https://t.co/THvcjm9SJu
#JACC#cvLipids
#BCISACI this is data from my national audit report presentation that is happening live now around #DCB use in the UK. Close to 20% of all PCI cases are DCB with wide variation amongst centres. Each centre is represented as a dot
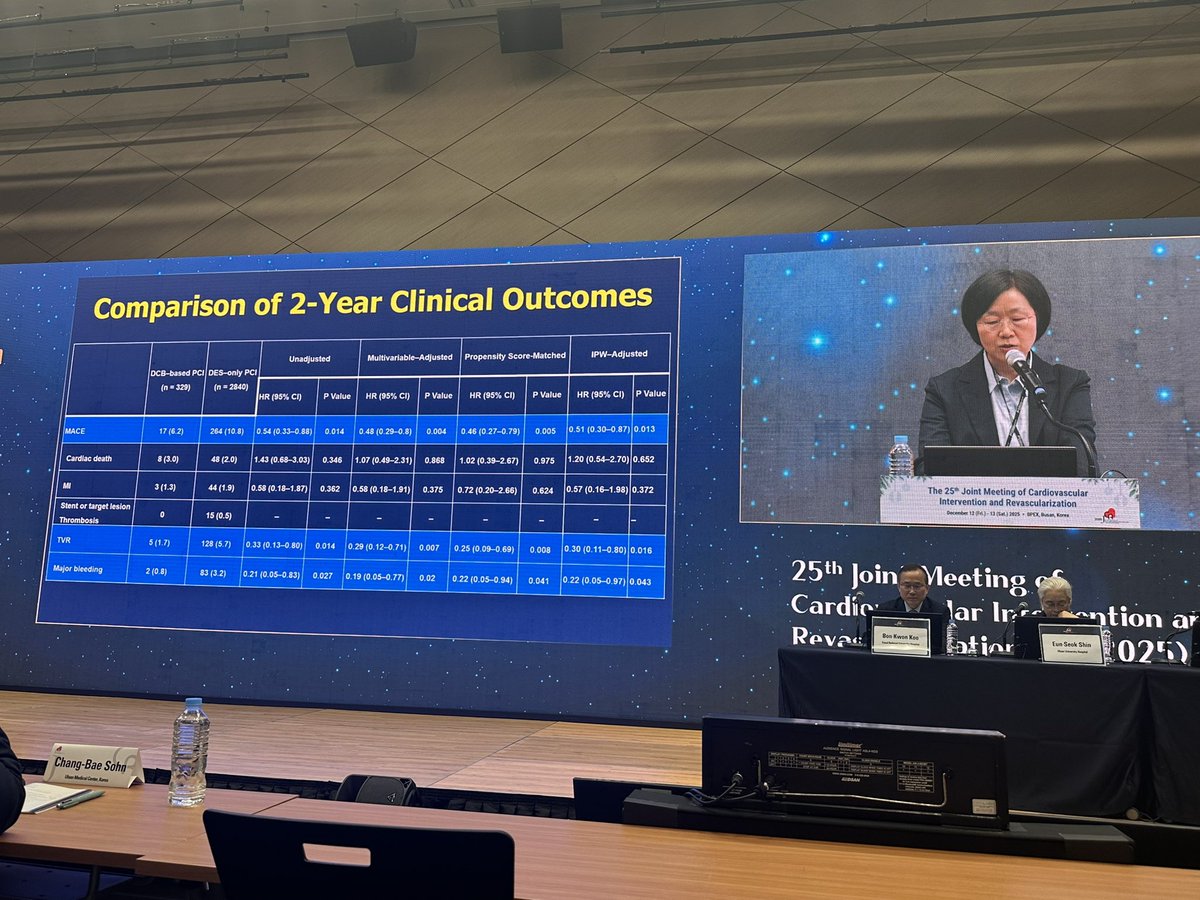
Ay-Young Her presenting JCR-DCB registry analysis of STEMI outcomes in DCB vs DES in STEMI showed better outcomes with DEB st 2 yrs. im sure that there are unmeasured confounders at play given even size- but i think it still is a viable strategy in selected pts.
We need a dedicated RCT