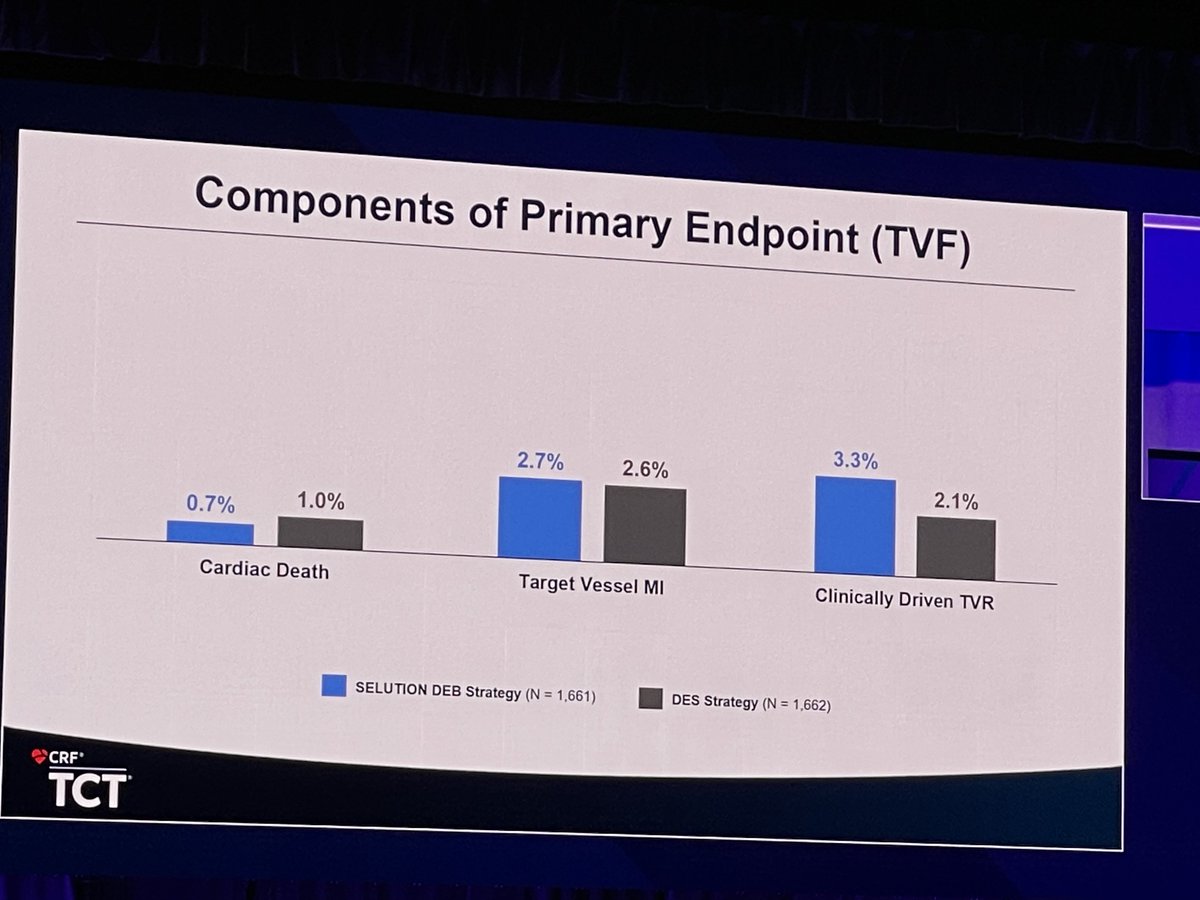
@jonnywatt@evandrofilhobr Ok so you have to trade off a slightly higher 1 year repeat revasc rate for SEB against a slightly higher cardiac death rate in DES
Death is undoubtedly the ultimate endpoint.
A repeat revasc is a choice…
Time to start making choices
@MarqPatton@sbrugaletta That’s not the point. A strategy of DCB first and DES when needed is being tested. The result is 80% fewer patients need a DES and the outcome in non-inferior
Why leave them with a DES if not needed. We all hate ISR and DES-induced ACS - poor PCI outcomes
@djc795@sbrugaletta We have published cost effectiveness already showing even with higher price on DCB that overall procedural cost v similar in a UK setting .
And not longer procedural time
and not more contrast
@djc795@sbrugaletta How many layers of metal are good? One? Two?? Three???
If you want to avoid ISR and worse (stent thrombosis) then you only need the DES for failed lesion prep. If your concern is restenosis just deliver the drug don’t leave metal behind
@MarqPatton@sbrugaletta But that means 80% of your cases can leave the lab stent-free and avoid those documented stent attrition rates seen out to at least 10 years. Why wait 10 years - it is safe and non-inferior at one.
GAME CHANGER😎
Mic drop….
#LBCT - SELUTION DeNovo Trial 🌟
At 1 year, PCI strategy with SELUTION DEB and provisional DES was non-inferior to the systematic use of DES for primary end point of TVF. #TCT2025@crfheart@TCTConference@TCTMD 💙🫶
@DrPascalMeier I will try but don’t use many anyway !😀
Only required for failed lesion prep and a vessel threatening dissection. So good prep and avoiding or modifying those nasty dissections gives you lots of options for a stent free result
@realarainmd Absolutely. Do your best lesion prep then choose the right destination device. We have the choice of DCB, scaffold or DES
PCI is changing (again)