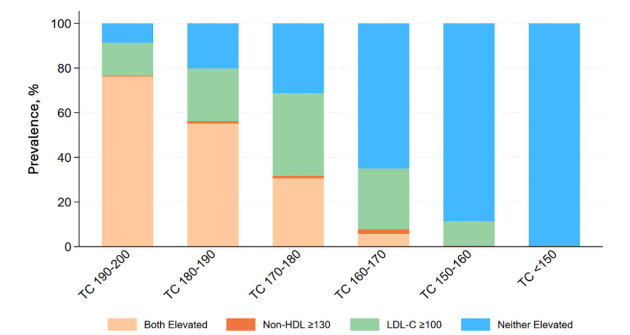
Is total cholesterol <200 mg/dL really "normal"?
In 82.6 million U.S. adults without ASCVD and TC <200 mg/dL:
→ 47.5% had LDL-C ≥100 mg/dL
→ 30.8% had non–HDL-C ≥130 mg/dL
→ 43% aged 40–75 were statin-eligible
But among adults with TC <150 mg/dL, virtually none had elevated LDL-C or non–HDL-C.
The historical TC <200 mg/dL threshold falsely reassures patients and clinicians. Public health messaging and lab reporting should prioritize atherogenic cholesterol and reflect that optimal TC is closer to <150 mg/dL.
Paper in @JClinLipidology (open access): https://t.co/6zE2gjXK2m
Grateful to @kfaridiMD for mentorship, and to coauthors @SethShayMartin@ErinMichos@rblument1@estyale@YaleCardiology@CiccaroneCenter@SmithBIDMC
We are thrilled to partner with the @CAUSALab for our upcoming symposium on external controls for causal inference!
Be sure to register soon - spots are limited: https://t.co/zKkHP56Zvp
Cardiogenic shock is associated with high early mortality. Prompt revascularization in infarct-related cardiogenic shock improves outcomes, and mechanical circulatory support may reduce mortality in specific groups.
Read the Review Article “Cardiogenic Shock” by Holger Thiele, MD (@thiele_holger), and Christian Hassager, MD, from Heart Center Leipzig at Leipzig University, Leipzig Heart Science, Rigshospitalet, and the University of Copenhagen (@koebenhavns_uni): https://t.co/V9IfEFDaYw
solid foundation in statistics is even more important in the age of AI.
This interactive app explaining statistic concepts is great
https://t.co/dO0YSMF9hf
The problems with this analysis:
The CTA findings are the covariates affected by prior treatment and influencing subsequent treatment. Patients who were already taking statins before imaging likely had slower plaque progression, which means their calcium score, plaque extent, or degree of obstruction on CTA partly reflected earlier exposure. Those same CTA results then shaped later treatment decisions, since clinicians are more likely to start or continue statins in patients with visible disease and to stop them in those with normal scans. In this way, the CTA phenotype becomes a time-varying confounder affected by prior statin use that also guides future prescribing (time-varying treatment), creating the classic treatment-confounder feedback loop and introducing selection bias.
Furthermore, the immortal time bias created by the "cumuluative statin use" will further bias the results.
Should we really answer such question, we need to align eligibility, treatment assignement, and start of follow-up.
Clinicans should continue prescribing statins based on the clinical indication and/or predicted risks.
Statin efficacy to decrease #MACE depends on #CAD phenotypes and increases with the extent and severity of disease and in the presence of high-risk plaques. Patients without CAD have no benefit from statin therapy regarding MACE. https://t.co/OUpvgkgOBv
#JACCIMG#cvCAD
Clinical decision making in mental health 🧠
Alejandro Szmulewicz @HarvardChanSPH continues the Methods Series @karolinskainst in 2 weeks.
📆 Nov 4, 2025
⏰ 15.00 CET/9.00 ET
📍 Online
Attend online:
https://t.co/p4tKqGZSnc