🔔 ¿Seguimos esperando a que la creatinina sérica suba para diagnosticar una Lesión Renal Aguda?
Llegamos tarde.
La línea de tiempo conceptual presentada en el #ERA26 demuestra que la creatinina y la caída del volumen urinario son marcadores de disfunción clínica tardía, no de daño temprano.
El estrés renal inicia mucho antes con la parada del ciclo celular, detectable inmediatamente tras el insulto mediante biomarcadores ultrasensibles como TIMP-2 e IGFBP7.
Cambiar nuestra mentalidad del diagnóstico funcional al molecular es imperativo para la nefroprotección crítica.
#Nefrología #MedicinaCrítica #ERA26 #AKI #NefroTwitter
#lesionrenalaguda #dañorenal #IRA #AKI
#ERA26
🚨Results of the study:
🍀HDx was non-inferior to OL-HDF for a composite cardiovascular outcome and showed similar safety and mortality profiles.
🍀HDx presents as an alternative to OL-HDF in settings where optimal convective dosing cannot be consistently achieved
One of the most awaited talks for this #ERA26
MOTheR HDx Study: A MOPR Study to Explore Morbidity and Mortality in Patients Dialyzed with Theranova HDx Compared with OL-HDF
🗣️ @DePsequera
Late breaking clinical trials 2:
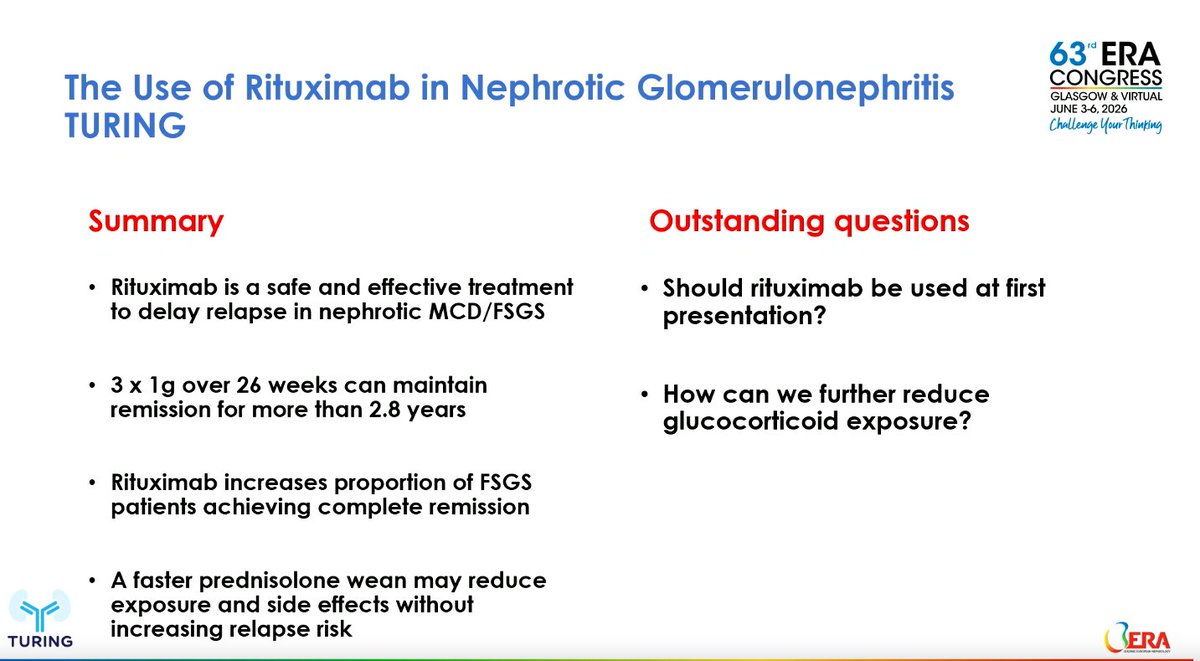
The Use of Rituximab In the treatment of Nephrotic Glomerulonephritis (TURING): a multicentre, double-blind, randomised, placebo-controlled trial
By Lisa Willcocks (Cambridge, UK) &
Megan Griffith @megan_griffith1 (London, UK)
#ERA26
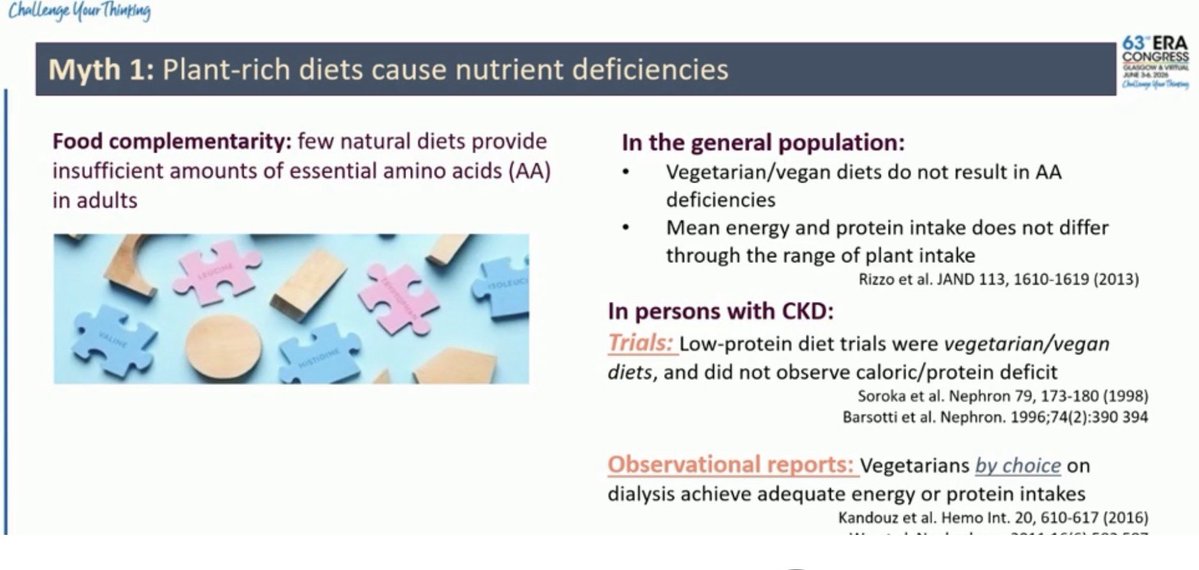
Starting strong with controversies in nephroprotection #ERA26@jjcarrero1 talking about potassium 🍌🥑
📍Plant-rich diets do not inherently cause protein deficiency in CKD.
Plant phosphorus is less absorbable, so plant-based diets may ⬇️ phosphate burden despite similar phosphorus intake
📍The evidence supporting routine restriction of fruits and vegetables to prevent hyperkalemia is weaker than traditionally believed
📍Focus on food quality and individual risk, not automatic avoidance of plant foods.
3/ Role of parietal epithelial cells
⏩ Parietal epithelial cells act as podocyte progenitors
⏩ Females generate more podocytes throughout life.
⏩ Estrogens drive podocyte regeneration
⚠️The proximal tubular phosphate transporter Npt2a may be more than a phosphate carrier‼️
💡In experimental AKI, Npt2a inhibition ➡️
📌restored mitochondrial fusion,
📌improved mitochondrial function and
📌attenuated kidney injury,
This highlights a novel Npt2a–Klf15–mitochondrial axis.
#ERA26 #AKI #KidneyResearch
🧵—Open your mind: New therapeutic opportunities in inherited kidney diseases
#ERA26@ERAKidney
1/🧵Overcoming Barriers in Rare Disease Drug Development
🗣️Speaker: Olivier Devuyst
1/ 💊 #ERA26
-Only a few rare genetic diseases have affordable treatment.
-Lysosomes are fundamental for cell cycling and promising targets for certain diseases.
Orgullosos de la participación activa de nuestra Unidad de Trasplante en el Congreso SET 2026.
📍Adjuntos y residentes compartiendo experiencia, aprendizaje e investigación en uno de los principales encuentros nacionales sobre trasplante💙🩺
#SET2026#Trasplante#Nefrología
#POCUS#echofirst answer: 1️⃣ Subxiphoid short axis view at the aortic valve level 2️⃣ RVOT Doppler
RVOT Doppler is one of the most underused but high yield tools.
● Tracks RV stroke volume and cardiac output
SV = CSA × VTI
CO = SV × HR
VTI alone works well for serial trends
● Estimates pulmonary vascular resistance
PVR = (TRV ÷ RVOT VTI) × 10 + 0.16
● Screens for pulmonary hypertension even when TR jet is absent
AccT <105 ms suggests PH
AccT ≤60 to 80 ms raises concern for acute PE
● Waveform shape gives physiology
Parabolic is normal
Early peaking and notching suggest rising PVR and help phenotype disease
● Distinguishes acute PE from chronic PH using AccT and notching patterns
● Provides insight into RV pulmonary arterial coupling
RVOT VTI ÷ PASP as a simple coupling metric
● Useful in congenital heart disease
Grading RVOT obstruction and serial follow up after repair
● Tracks response to therapy noninvasively over time
CWD complements PW when velocities are high
● Grades pulmonic stenosis using peak velocity and gradients
Severe if peak gradient >64 mmHg or velocity >4 m/s
● Estimates pulmonary pressures from PR jet
mPAP = 4(V peak PR)² + RAP
PAEDP = 4(V end diastolic PR)² + RAP
● Identifies multi level RVOT obstruction
Double contour envelope suggests infundibular plus valvular disease
● Detects dynamic RVOT obstruction
Late peaking dagger shaped signal
● Enables global RV performance assessment
Tei index combining TR and RVOT flow
● Monitors conduit or bioprosthetic valve gradients over time
🤓 AKI in the ICU is not just kidney failure.
It is a hemodynamic and congestion failure.
🚨 Reality check
👉 AKI occurs in:
▪️ 13-36% of acute HF patients
▪️ Up to 80% in cardiogenic shock
👉 Dialysis needed in up to 13%
👉 Strongly linked to mortality
⚠️ The key mistake
We treat AKI as a creatinine problem
💥 But it is actually:
👉 A perfusion + congestion problem
🧬 Core physiology
Renal perfusion pressure = MAP - CVP - IAP - airway pressure
📌 The nephron needs ≈ 40 mmHg to function
🔥 So what kills the kidney?
Not just low pressure
But:
▪️ Venous congestion (↑CVP)
▪️ Fluid overload
▪️ Intra-abdominal hypertension
▪️ Low forward flow
🧩 Step-by-step mindset
1️⃣ Confirm congestion
👉 JVP, no fluid responsiveness, VExUS ≥1
2️⃣ Optimize hemodynamics
👉 Maintain MAP ≥65 mmHg
3️⃣ Decongest
👉 Diuretics = cornerstone
4️⃣ Escalate
👉 CRRT if failure
📌 It’s a flow-pressure-congestion algorithm
💊 Pharmacology reality
❌ “Renal-dose dopamine” → useless AND harmful
❌ No drug prevents AKI
✔️ Loop diuretics → first-line
✔️ Sequential nephron blockade if resistance
⚡ Diuretic resistance = turning point
👉 Think:
▪️ Gut edema → poor absorption
▪️ Hypoperfusion
▪️ Tubular dysfunction
👉 Solutions:
▪️ Higher doses
▪️ Combination therapy (thiazides, acetazolamide)
▪️ Consider hypertonic saline strategy
🚨 CRRT is NOT first-line
👉 Indications = AEIOU:
▪️ Acidosis
▪️ Electrolytes
▪️ Intoxication
▪️ Overload
▪️ Uremia
👉 Early CRRT?
❌ No mortality benefit
✔️ Wait-and-see + optimize first
🧠 Advanced insight
👉 The kidney fails more from:
✔️ Congestion than hypotension
✔️ Venous pressure than arterial pressure
🔥 Take-home
AKI management in ICU is:
✔️ Hemodynamic
✔️ Congestion-driven
✔️ Stepwise
🚨 Final message
👉 Don’t chase creatinine
👉 Don’t reflexively dialyze
Treat:
Perfusion + Decongestion + Time
📚 Riccardi et al.
European Heart Journal Acute Cardiovascular Care, 2025
https://t.co/OLnrbCQ8Y2
LESIÓN RENAL AGUDA EN CIRROSIS ‼️
📌LRA en cirrosis ( Criterios KDIGO) :
a) aumento de la creatinina sérica ≥0,3 mg/dl en 48 h o ≥50% del valor basal que se sabe o se presume que ocurrió en los 7 días anteriores y/o producción de orina ≤0,5 ml/kg durante ≥6 h
🔴 ¡Empezamos con el Módulo 1️⃣!
➡️ Fundamentos de la Hemodiálisis▪️Principios biofísicos▪️Composición del líquido de diálisis ▪️Acceso vascular @EmiliSanAlv@mf_slon@DePsequera@Florijaviesther👇
🔄 ACTUALIZADO en #Nefroaldía@nefroaldia
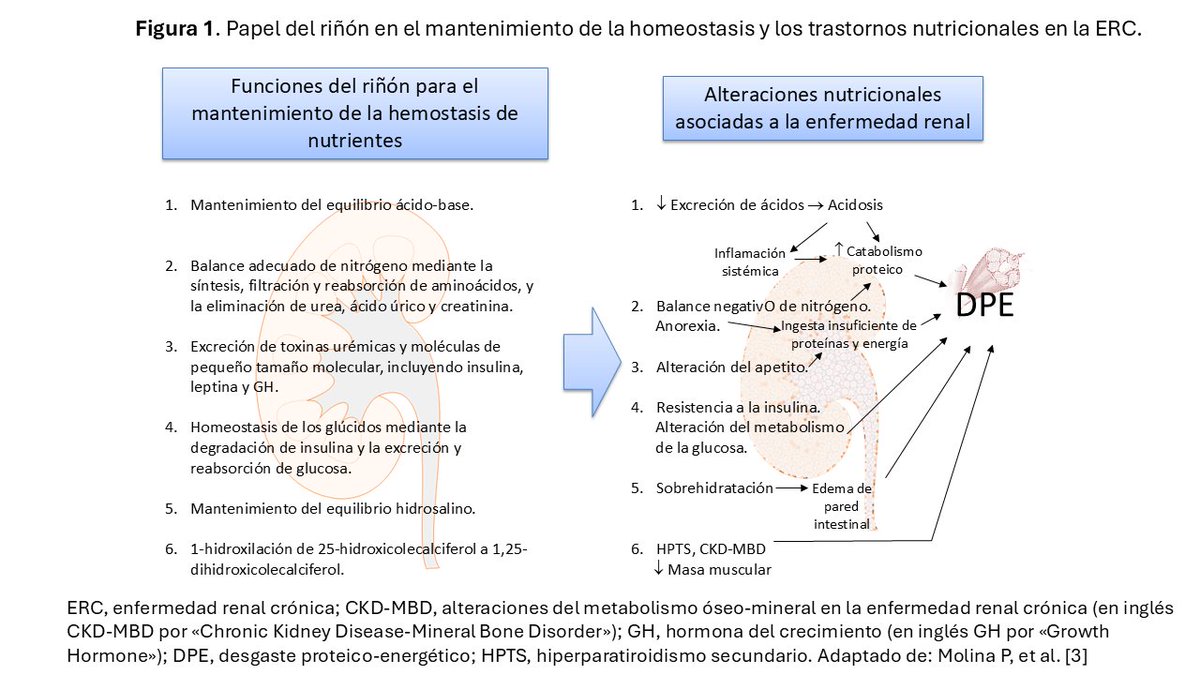
🥗 "Nutrición en Nefrología. Conceptos generales y estimación de los requerimientos nutricionales"
✍️ Por Pablo Molina @MolinaPab, Emma Huarte @emma_huarte y Macarena Arancibia
🔗 https://t.co/0HHR556aoT