My Quality Improvement Project on Emergency Department PoCUS governance and administration been accepted for publication by @BMUS_Ultrasound@SAGE_Publishing 🙏🏾
So much blood, sweat and tears. All worth it.
@RCollEM@EMTAcommittee very keen to see an improvement nationally
🫀POCUS is no longer just a bedside imaging tool.
It is becoming real time physiological intelligence.
This excellent 2026 review highlights how modern POCUS is expanding into:
• ultrasound guided regional anesthesia
• shock and cardiac arrest management
• AI assisted imaging
• advanced diagnostics
• governance and medicolegal practice
Some of the most provocative concepts: • “Occult VF” detectable only on echocardiography during cardiac arrest
• Ultrasound guided CPR compression positioning
• AI assisted lung ultrasound acquisition by nonexperts
• Handheld devices approaching cart based diagnostic performance
One important medicolegal message: several lawsuits involved failure to perform POCUS when clinically indicated.
The future of emergency and critical care medicine will likely depend on clinicians capable of integrating: physiology + imaging + AI + rapid bedside decision making.
POCUS is not anymore an “optional skill” but “core clinical infrastructure.”
Mani N, Rao S, Kim DJ. Point-of-care ultrasound in the modern era of emergency medicine: a narrative review of the recent literature. Curr Opin Crit Care. 2026. doi:10.1097/MCC.0000000000001358
How should you resuscitate sepsis post Andromeda-Shock 2?
Join us, the investigators on Andromeda-VEXUS, Andromeda-Shock 2 as we have a full throttle webinar (debate? cage match?) and settle this with a discussion of the blend of evidence and physiology.
When: June 10th 3:00pm ET (12:00pm PT)
Free Registration: https://t.co/kkIXy3Oi24
Super pumped for it!
For example, in a study of 96 ED patients undergoing CTPA for suspected PE, 56% of them had an alternative diagnosis identified on lung ultrasound: pneumonia, pulmonary edema, or pleural effusion.
This suggests that more than half of those CTPAs could have been avoided with a prior POCUS exam.
https://t.co/1Dyuilpel7
Doc 1: I did #POCUS. EF is great. I’m done!
Doc 2: Wait… do you want to comment on the LV wall thickness? Could it have implications for fluid therapy? (e.g. associated diastolic dysfunction, SAM depending on the clinical context). What about cardiology referral for further imaging or genetic testing?
#Nephpearls #FOAMed
New in EMJ - free open access:
Endovascular resuscitation: an expert practice review
A practical overview of REBOA, SAAP and ECPR for emergency physicians managing the sickest patients in shock or cardiac arrest.
Please read / comment / share
DOI: 10.1136/emermed-2025-215376
🚨 HOT OFF THE PRESS! 🚨
New guidance from the American Society of Echocardiography @ASE360 for Cardiac Ultrasound Artifacts 🫀📡
➡️https://t.co/UB6Pz1H5NV
👉 A must-read for everyone in #EchoFirst!
🔍 What is an artifact?
➡️ An imaging feature that does NOT reflect true anatomy/pathology
➡️ Common, expected, and rooted in ultrasound physics ⚙️
💡 Why this matters
⚠️ Artifacts can mimic disease → misdiagnosis → inappropriate management
⚠️ Present across ALL modalities:
• 2D 🖥️
• Spectral Doppler 📈
• Color Doppler
• 3D echo 🧊
📘 What this guideline delivers
✅ Standardized, structured approach to artifacts
✅ Clear explanation of:
• Appearance 👁️
• Mechanism ⚙️
• Clinical impact 🏥
• Real-world cases 🧾
• Mitigation strategies 🛠️
🧠 Also covers
🔹 “Artifact-like” phenomena
🔹 Interference from external devices & equipment 📡
🎯 Key takeaway
👉 Artifacts are inevitable—but misinterpretation is not
👉 Mastering them = safer, smarter echo practice
👩⚕️👨⚕️ Who should read this?
➡️ Sonographers
➡️ Cardiologists
➡️ Trainees
➡️ Anyone interpreting cardiac ultrasound
📢 Elevate your imaging game. Recognize. Understand. Mitigate.
#CardioX #Cardiotwitter @JournalASEcho #ACCFIT
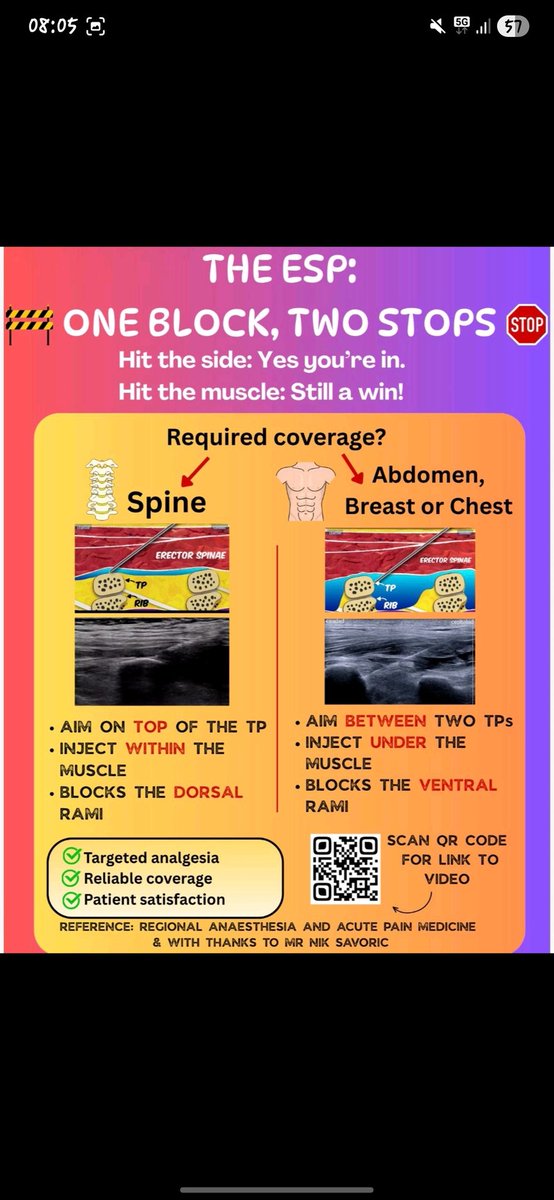
@Anaes_Journal The other aspect with the RCT (Ref 2) to note is, the injecrion is performed at T3. For any thorax indication, I have been told T5-7. So, I am not all all convienced the technique used in the RCT was the correct approach, which could jabe lead then led to the observation made.
@Anaes_Journal This approach is now recognised more and more is the incorrect technique as it only blocks dorsal rami. However if aimed at the tip of the TP (as I see it all the time), it works like magic (proxy to PVB indeed without going into the danger zone) as shown below
• Serratus Anterior and Erector Spinae Plane Blocks for rib fractures
• Popliteal Sciatic Nerve Block for ankle fracture manipulation
Just two of our live sessions daily, on our booth.
Don’t miss these fantastic sessions happening live on our stand (6).
🫀 Hemodynamics is not blood pressure... actually, It never was.
⚠️ The biggest mistake in perioperative & critical care:
👉 Treating numbers instead of physiology
📊 What we were taught
✔️ BP
✔️ HR
✔️ SpO₂
🔥 What actually matters
👉 Flow + oxygen delivery + tissue perfusion
🧠 Core concept
👉 Blood pressure ≠ perfusion
You can have:
▪️ Normal BP → low cardiac output
▪️ High BP → poor microcirculation
▪️ Stable vitals → ongoing hypoxia
💡 Why?
Because:
👉 BP = CO × SVR
Same pressure
→ completely different physiology
🧬 The real pillars of hemodynamics
✔️ Cardiac output
✔️ Stroke volume
✔️ Preload / afterload / contractility
✔️ Oxygen delivery (DO₂)
⚠️ Critical insight
👉 Oxygen delivery = CO × arterial O₂ content
Not:
❌ BP
❌ SpO₂ alone
🔥 This is where advanced monitoring changes everything
👉 From static → dynamic
👉 From guess → prediction
🧠 Dynamic parameters outperform static ones
✔️ SVV
✔️ PPV
✔️ PVI
👉 Predict fluid responsiveness
👉 Avoid fluid overload
💥 Reality check
Only ~50% of unstable patients respond to fluids
👉 The rest get harm
🫀 Next level thinking
👉 Ventriculo-arterial coupling
👉 Cardiac power output
👉 Tissue perfusion markers
🚨 Final message
Stop asking:
❌ “What is the blood pressure?”
Start asking:
👉 “Is the patient perfusing?”
🧠 Because in critical care:
👉 Flow saves organs
Pressure just looks good on the monitor
📚 Demir et al., Aydın et al.
Turkish Journal of Anaesthesiology & Reanimation, 2025
DOI: 10.4274/TJAR.2025.251926
DOI: 10.4274/TJAR.2025.251925
Join me @POCUSUK and @BBraunUSA at the RCEM Annual Conference 2026 at the ICC, Birmingham (Stand 31)! 📍
Don't miss the live scanning on key hip and chest blocks—including PENG Block, FICB, SAPB, and ESPB.
🗓️ When: 28th & 29th April, 3:30 PM - 4:00 PM
Stop press: sterile gowns are no longer mandatory for spinal anaesthesia.
I’m so proud to have been part of this process trying to simplify our practice, making us more efficient, more sustainable without increasing risk to our patients.
https://t.co/JxQoNmkBql
Congratulations to this weeks short clip challange winner Tanner Course!
Q1: A 62-year-old man with a history of diabetes, cardiac amyloidosis, and early onset dementia presents with new-onset shortness of breath. You perform a POCUS exam in the PLAX view. What descriptors could be applied to the left ventricular myocardium?
A1: Granular ; Echodense and Hypertrophic. All the above for the quiz
https://t.co/bs6yBkZAHN
Counting down to this year’s @Royal College of Emergency Medicine conference.
We’re excited to have a live scanning schedule happening daily at our booth led by Dr. Nick Mani.
Don’t miss these insightful sessions on our stand!
@EveryOneNoOne1