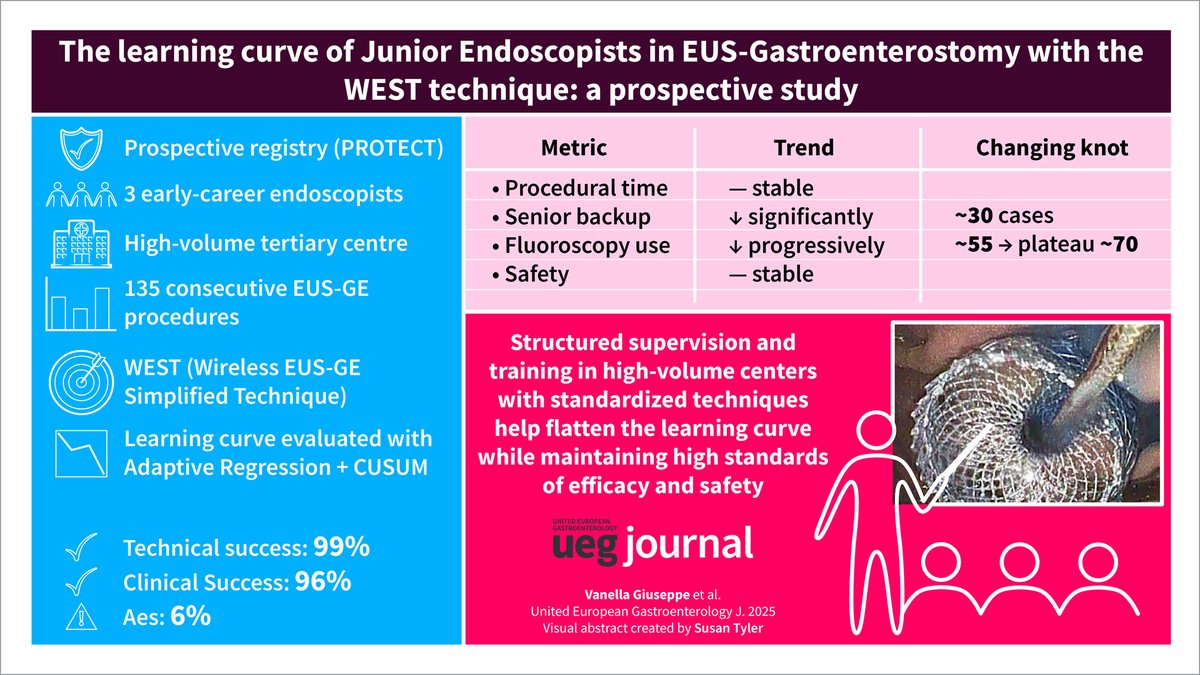
An 8 cm stent may not remain 8 cm after deployment!
A crucial concept in stent selection: Foreshortening
Most commonly used SEMS are braided (e.g. WallFlex).
As they expand, they shorten in length—sometimes by as much as 40%.
In contrast, laser-cut stents are fashioned from a single metal tube and exhibit minimal foreshortening.
The tradeoff? Greater axial force and often more patient discomfort.
Paciente que debutó con esta lesión en cola de páncreas. En la EUS se aprecia su componente sólido. Nótese la cercanía con la glándula suprarrenal izquierda.
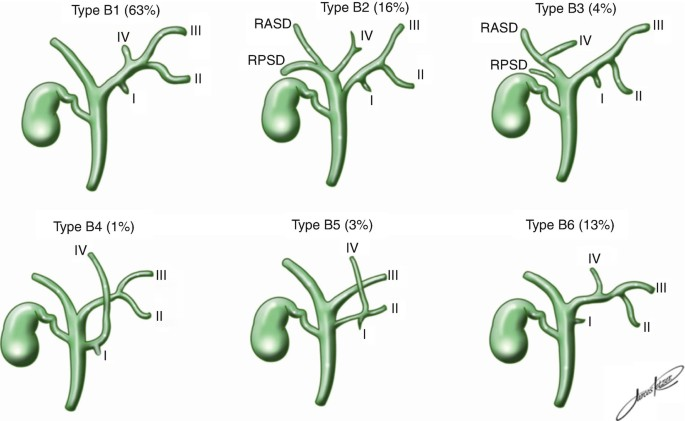
The biliary "variant" framework undersells how individualized biliary anatomy actually is. Unlike vertebral count or hepatic arterial trunks, bile ducts develop via stochastic branching morphogenesis. Every cholangiogram is one of a kind.
Thank you for coming to my TED talk.
Si haces EUS-gastroenterostomía en estenosis duodenal infranqueable: ocluye el píloro con balón para distender el asa yeyunal. Facilita colocar el LAMS. Detalle técnico que marca la diferencia.
🔗 https://t.co/mf7Q1fCZuK
#EUS#Gastroenterostomía#TipEndoscopia
Dos casos de coledocolitiasis diagnosticados por ultraaonografía endoscópica , luego de resultado de resonancia negativo y persistencia de sospecha diagnóstica .
28/F with 2.4 cm cyst in head of pancreas. EUS shows a nodule within cyst which takes up contrast. Biopsy shows abundant mucin and columnar epithelium. MPD is not dilated. Surgery or observe?
#GITwitter
Chong et al compare "Contrast-enhanced endoscopic ultrasound versus conventional endoscopic ultrasound–guided fine-needle biopsy with macroscopic on-site evaluation for solid pancreatic lesions: a multicenter randomized trial." https://t.co/fmLlASZWYU
#GITwitter
Nice video from a freehand EUS guided gastrojejunostomy in the setting of malignant outlet obstruction.
We did a NAJA assisted EUS GJ this week (first EVER in the state of Colorado!). Suspect NAJA will be preferred way to do these.
#gitwitter#surgery@bsc_endoscopy@KristenHaeck
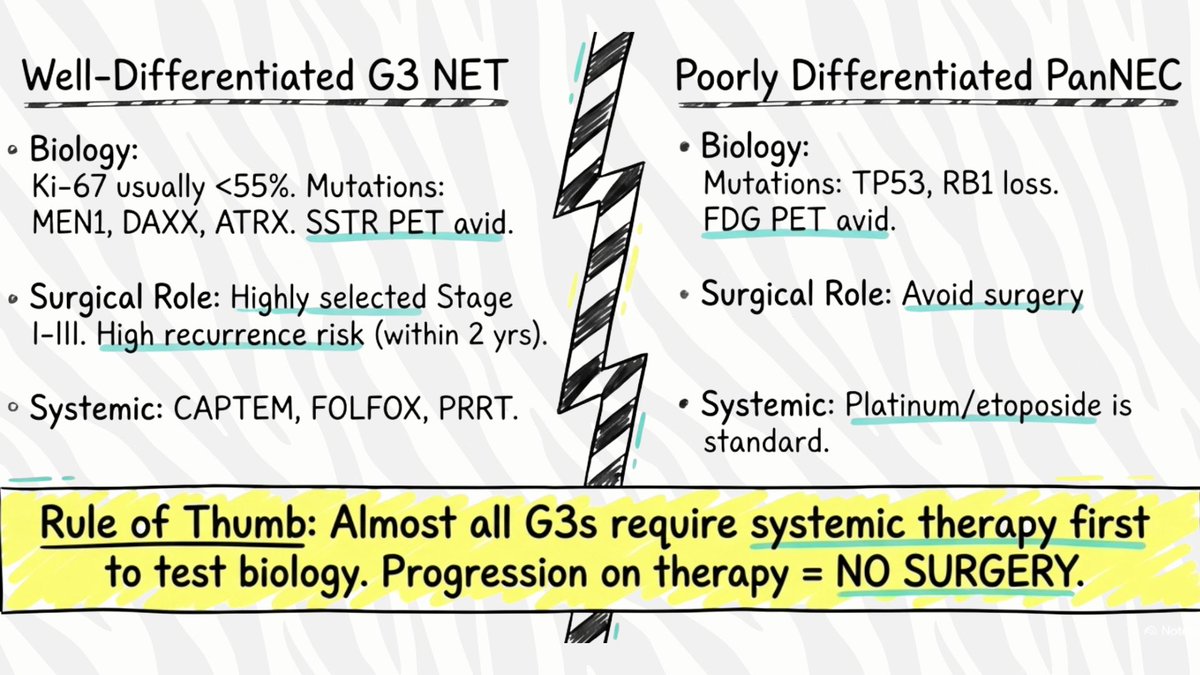
🦓PanNETs @BJSurgery Commission: G3 PanNENs
🔬G3 NET vs NEC is EVERYTHING
🧬Molecular profile (MEN1, DAXX, ATRX) can help risk-stratify
🔪Surgery only for highly selected localized G3 NETs
⚠️Recurrence expected: systemic therapy 1st
🔗https://t.co/fqS90z6MkO
@spartelli
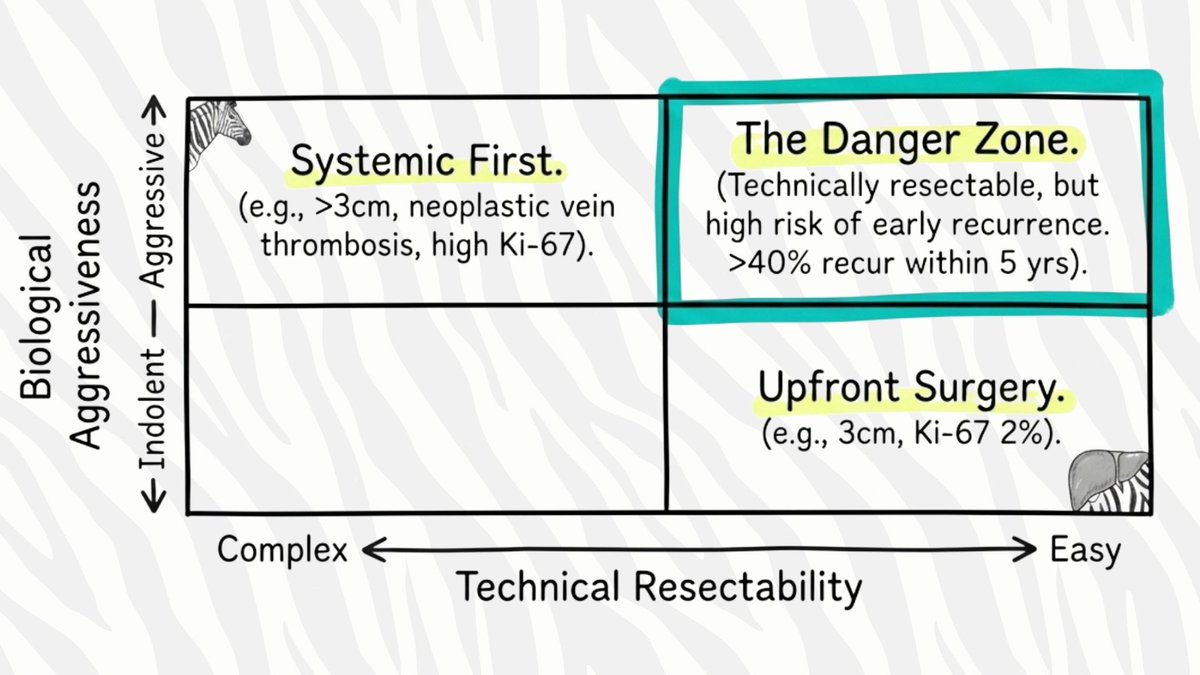
🦓PanNETs @BJS_Surgery Commission: surgery in NF PanNETs >2 cm?
>40% recur within 5 yrs‼️
🔬Need to define "borderline resectable" biologically, not just technically
💊Preop therapy 🔑 to test biology & downstage
🔗https://t.co/fqS90z6MkO
@spartelli
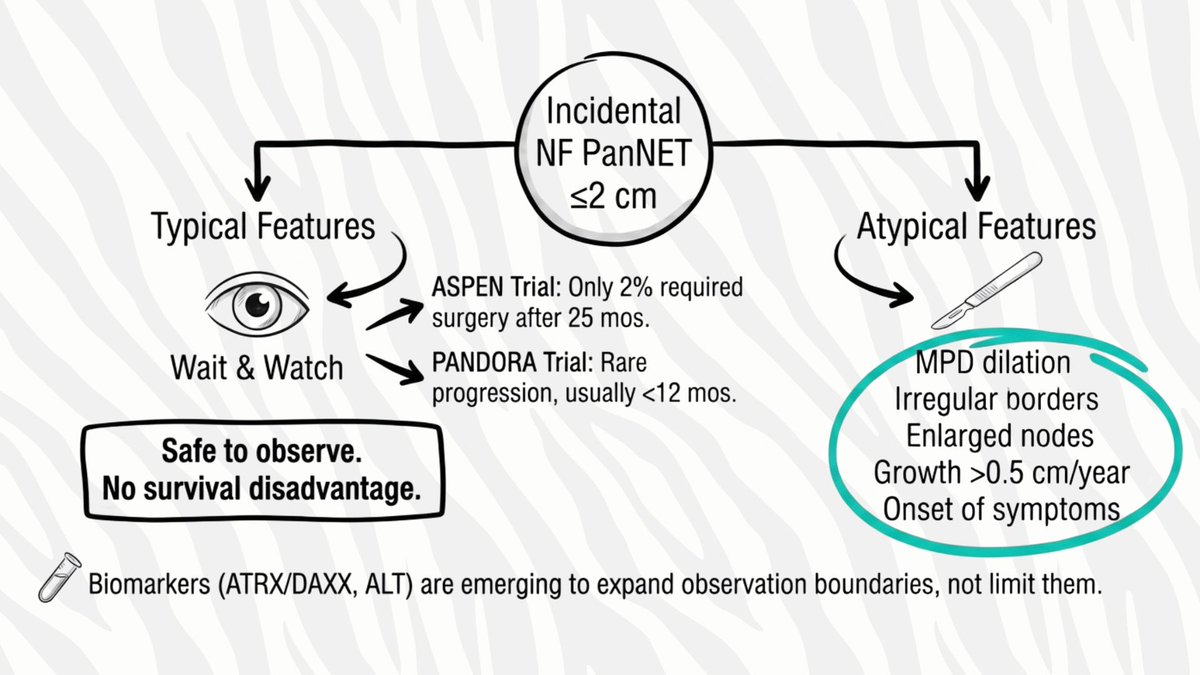
PanNETs @BJSurgery Commission: operate on small NF PanNETs ≤2 cm?
⏱️With typical features - observation safe
📊PANDORA & ASPEN: rare progression, no survival compromise
🔪Surgery for atypical features (MPD⬆️, heterogeneity, ⬆️nodes)
🔗https://t.co/fqS90z6MkO
@spartelli
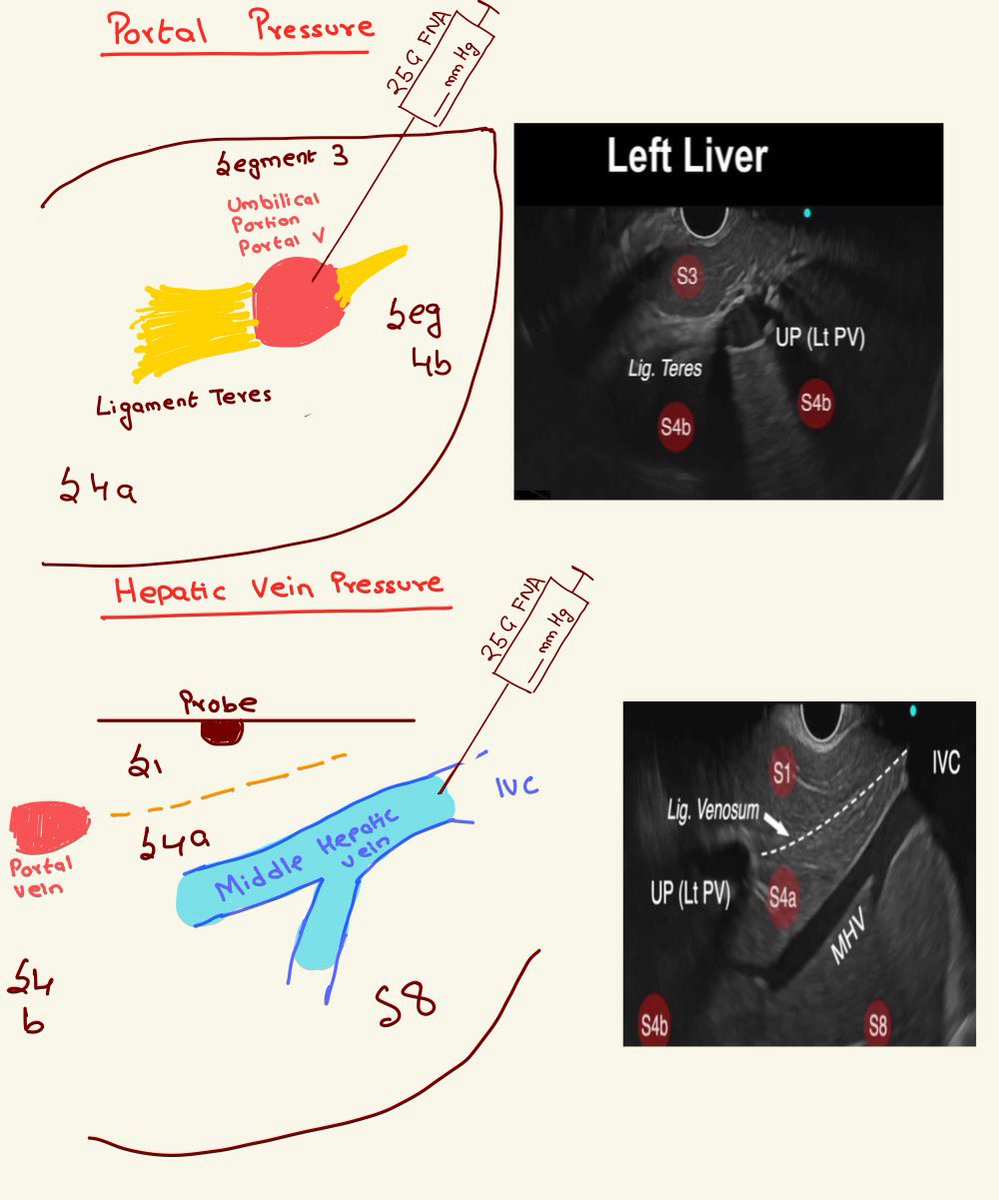
EUS liver examination: Portal pressure measurements
1. Targets are portal V, Hep V from the stomach (see prior tweets on identification).
2. Use 25G FNA needle, heparin flushed, 3 measurements.
3. We prefer umbilical portion of PV, middle hepatic vein for measurement.
Continuing our liver journey:
After identifying Middle Hepatic vein (prior tweet), pull back, clockwise torque-->
1. Right hepatic vein branching from the IVC
2. Segments 1, 7, 8 are identified
All the targets for portal pressure measurements are visualized (more soon!)
EUS exam of left liver continues along left portal vein
1. From umbilical portion of PV-> Clockwise torque
2. Reach Ligament Teres: Hyper echoic, connects PV to IVC
3. Push in, visualize middle hepatic vein: "Elephant Trunk"
With this entire left lobe is examined!