¡REVOLUCIÓN TOTAL EN #ERA2026!
Presentado hoy y publicado en el NEJM, @NEJM el ensayo MAJESTY cambia el paradigma en Nefropatía Membranosa Primaria.
Al comparar Obinutuzumab (anti-CD20 de 2ª generación) frente a Tacrolimus, la diferencia en pacientes libres de recaída tras lograr la remisión es abismal en la semana 104.
Mientras que el grupo de Tacrolimus sufre un desplome drástico en la estabilidad clínica (menos del 40% libre de recaída al final del seguimiento), Obinutuzumab mantiene a cerca del 90% de los pacientes en remisión sostenida.
La depleción de células B profunda y duradera demuestra que la inmunoterapia dirigida es muy superior a la dependencia crónica de los CNIs.
Bibliografía:
Obinutuzumab versus Tacrolimus in Primary Membranous Nephropathy (MAJESTY). N Engl J Med, Jun 5, 2026. https://t.co/cseHqGLlYB
#Nefrología #Glomerulopatías #ERACongress #MAJESTYtrial #NefroTwitter #nefrologia #eraedta #nejm #nephrology
📢 The MAJESTY trial results were published in @NEJM and it's results has been presented in the #ERA26
A major milestone in the treatment of Primary Membranous Nephropathy (MN)
Obinutuzumab 🆚 Tacrolimus —let’s break down the data 🧵👇
🔗 https://t.co/x4t6pG2qaT
#MembranousNephropathy #GlomerularDisease #KidneyDisease #NephTwitter #NephX #Obinutuzumab #PLA2R #ERA26
🚨 La nefrología ya cambió.
iSGLT2, inmunosupresión personalizada, hemodiálisis expandida y más.
📍24 julio
⚠️ Regístrate.
https://t.co/rIO92Ntpwl
Descarga el Programa Académico aquí:
https://t.co/mz5yOiJEyD
En hemodiálisis, realizar sesiones de >4:00hrs, comparado a <3:15hrs; se asoció a ↓27% y ↓19% el riesgo de morir y de hospitalizarse, respectivamente
Kidney Int Rep 2026
https://t.co/kNV4gmtRzJ
3 MINUTOS para estar más preparado 🫰
Enfermedad renal poliquística AD
🔵 Trastorno monogénico que más causa falla renal en adultos (50% falla renal a los 60a)
🔵 Investigar acerca de:
-Dolor crónico (60% a los 40 años)
-Fatiga (50%)
-Trastornos del estado de ánimo (30%)
-Baja autoestima (30-40%)
¿La obesidad empeora el pronóstico de la ERPQAD?
🧐Coffee consumption and chronic kidney disease
https://t.co/8kTB0ASL6J
☕️Current evidence suggests that moderate caffeine intake is probably safe in CKD and may be potentially beneficial
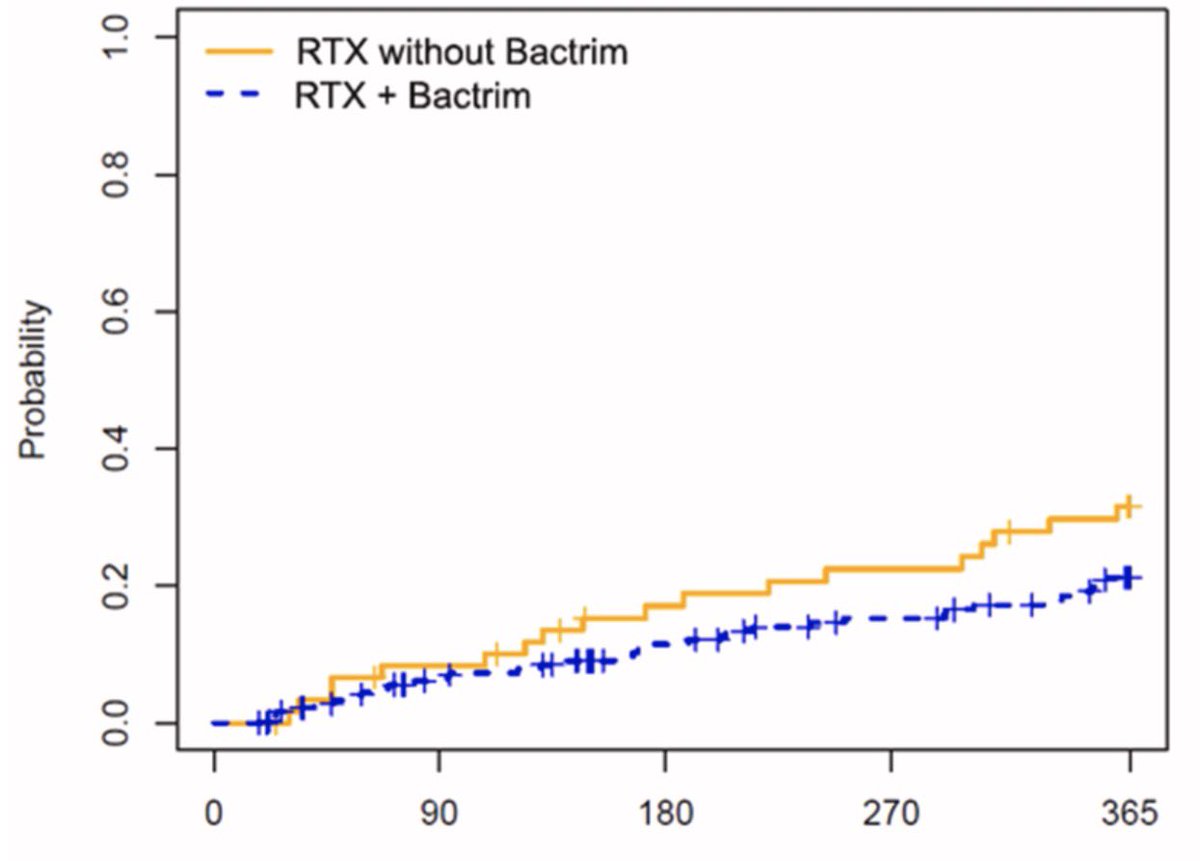
En Vasculitis ANCA tratados con Rituximab, dar profilaxis con trimetropim/sulfametoxazol, comparado a no hacerlo; se asoció a ↓47% riesgo de infección. Esta protección no se observó en otras glomerulopatias
Kidney Med 2026
10.1016/j.xkme.2026.101275
Atención NEFRÓLOGOS 🚨
Se abre la convocatoria para la sexta generación del diplomado de TRRC y soporte Multiorgánico
Pre-registro antes del 10 de mayo 2026
https://t.co/scTdLLZREF
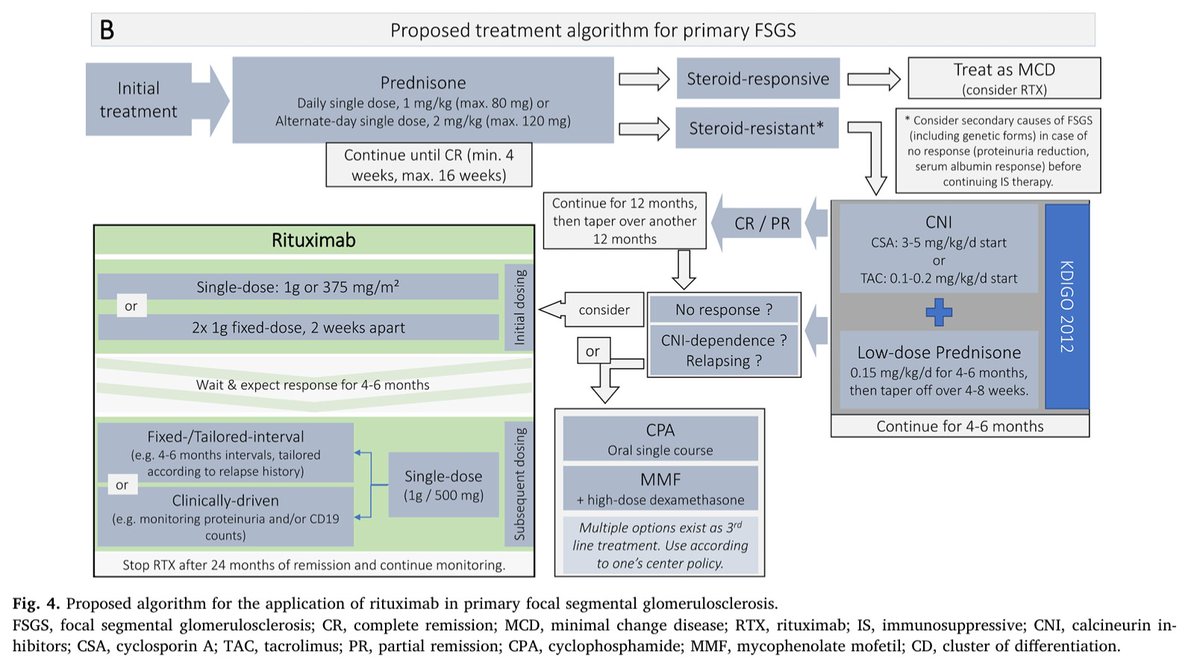
Proposed algorithm for the application of rituximab in minimal change disease (MCD) and primary focal segmental glomerulosclerosis (FSGS) ca. 2020
#Nephpearls
👉 https://t.co/Yqzstab0JT
Este sencillo puntaje predice con certeza del ~80% que pacientes tendrán sangrado posterior a realizar una biopsia renal guiada por ultrasonido
>5 puntos = sangrado en 19% de los casos
Kidney Med 2026
https://t.co/PeCSwtY8Hz
Exciting news for the glomerular community! 📢
The FDA has approved sparsentan for the treatment of FSGS in adult and pediatric patients (≥8 years) without nephrotic syndrome 🐙
💫This is a milestone—sparsentan is the first and only therapy specifically approved for FSGS
🔗 https://t.co/1uyLAZWrWm
#FSGS #FDA #GlomerularDiseases #Milestones #NephTwitter
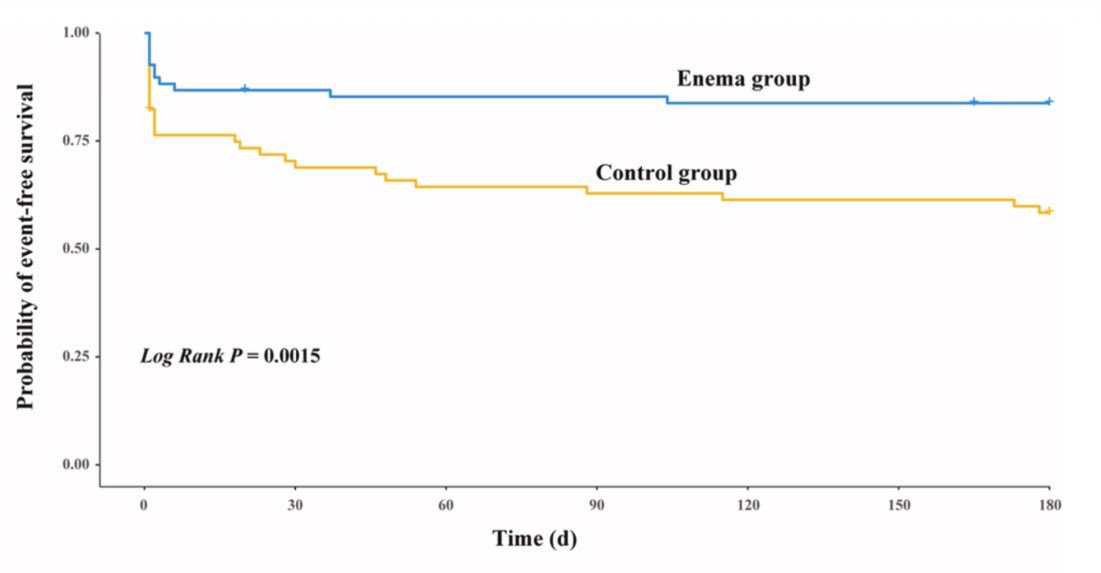
Previo a colocar el catéter de diálisis peritoneal, aplicar enema jabonoso, comparado a no hacerlo; ↓71% el riesgo de disfunción del catéter durante los primeros 6 meses. Mejor aún en los que no tienen constipación
Ensayo clínico
Kidney Int Rep 2026
https://t.co/JE9QvuvUHH
¿Cuál es el futuro de la Nefrología? 🏥
El Dr. Enrique Morales lo tiene claro:
1️⃣ Gran avance de la fisiopatía
2️⃣ Gran revolución de la genética
3️⃣ La Inteligencia Artificial
#EntrevistasSOMANE#SOMANE#Nefrología Medicina
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx