🧠 💜 Post-cardiac arrest care has entered a new era: precision over routine.
The management of hypoxic–ischemic brain injury continues to evolve, and this excellent review summarizes the major changes introduced by the 2025 ERC/ESICM recommendations. The focus has shifted from isolated interventions toward a multimodal strategy aimed at maximizing neurological recovery while avoiding premature prognostic decisions.
Key clinical updates:
🧠 Temperature control: Routine therapeutic hypothermia is no longer recommended for all patients. The priority is active fever prevention, maintaining core temperature ≤37.5°C for 36–72 hours.
🫁 Ventilation: Target SpO₂ 94–98% and PaCO₂ 35–45 mmHg while using lung-protective ventilation (6–8 mL/kg predicted body weight). Both hyperoxia and hypocapnia may aggravate secondary brain injury.
🩸 Hemodynamics: A MAP target of 60–65 mmHg is appropriate for most patients, but perfusion goals should be individualized according to baseline hypertension and evidence of end-organ hypoperfusion rather than pursuing universally higher pressures.
⚡ Neuromonitoring: Early EEG (within the first 24 hours) is recommended to detect non-convulsive seizures and identify malignant EEG patterns. Prophylactic antiepileptic therapy is discouraged; treatment should target documented seizures.
🔬 Neuroprognostication: No single test should determine prognosis. Reliable prediction requires waiting at least 72 hours after ROSC, excluding confounders, and integrating neurological examination, EEG, SSEP, neuroimaging, and serial neuron-specific enolase measurements. Premature withdrawal of life-sustaining therapy remains a major source of preventable poor outcomes.
Perhaps the most important message is that brain recovery is a dynamic process rather than a single time point. Modern post-cardiac arrest care emphasizes structured multimodal assessment, delayed prognostication, early rehabilitation, and comprehensive long-term follow-up to maximize meaningful neurological recovery.
Reference 📚
Kortli S, Nasa P. The neurological phoenix: multimodal strategies for brain recovery and prognostication in post-cardiac arrest syndrome—a 2025 clinical framework. Frontiers in Medicine. 2026;13:1775538. doi:10.3389/fmed.2026.1775538
I’m so exhausted with this BS about piptazo being nephrotoxic.
I’ve written blogs on this since 2016
There was never a plausible mechanism for nephrotoxicity
The ACORN RCT validated this
Great example of academics publishing bad studies that cause harm
Please stop. #1/2
Hemorragia intracerebral, una grandísima revisión del último número de Continuum. Algunos puntos importantes:
🔴 El factor más importante: hipertensión arterial. Así que lo más importante para prevención: control estricto (<120/80 mm Hg es mejor para reducir recurrencia).
🔴 Después de un sangrado, es relativamente seguro reiniciar los antiagregantes plaquetarios - lo sabemos por RESTART Trial y E-START Trial.
🔴 En cambio, reiniciar antiagregantes después de hemorragia intracraneal en alguien con fibrilación auricular es un terreno gris, en general no se recomienda. (PRESTIGE-AF Trial)
🔴 Irónicamente, los sobrevivientes de hemorragia intracraneal tienen más riesgo de EVC isquémico e infarto al miocardio (3% por año).
🔴 La recuperación funcional de hemorragia es más lento que de EVC isquémico. Menos de 50% que inicialmente presentan discapacidad grave logran recuperar independencia parcial a los 6-12 meses.
Léanlo completo en el canal (https://t.co/3O93s10lns).
【Top 10 ICU Papers from the First Half of 2026】
I selected 10 ICU-related papers published between January and June that I found particularly important.
The list includes:
• Five RCTs published in the NEJM
• Guidelines on sepsis, pulmonary embolism, and critical care for older adults
• Reviews on rehabilitation and anticoagulation reversal
Let’s get started ↓
🏥😵💫Manejo de la Encefalopatía Hepática en el Paciente Hospitalizado
🔰📚Frontline Gastroenterology 2026
doi:10.1136/flgastro-2025-103330
Enlace a Artículo Completo👇🏻🆓✅
https://t.co/xumUMHaxVK
I used to teach that venous congestion reduces organ blood flow because it reduces the pressure gradient across the capillary bed.
Higher venous pressure.
Lower driving pressure.
Less flow.
Simple.
But I don’t think that explanation survives first principles.
The next article on my Substack will be: venous congestion, back-pressure, and why MAP − CVP does not explain organ perfusion. Stay tuned!
https://t.co/54f9IPVCXf
@ThinkingCC@NephroP@ArgaizR
#OJOALDATO - España solo ha ganado TRES partidos en la Copa del Mundo desde que fue campeona en 2010:
🇪🇸 ESP 3-0 Australia (2014)
🇪🇸 ESP 1-0 Irán (2018)
🇪🇸 ESP 7-0 Costa Rica (2022)
En ese mismo periodo, CATORCE selecciones diferentes han ganado más partidos:
🇫🇷 Francia: 14
🇧🇪 Bélgica: 11
🇦🇷 Argentina: 10
🇧🇷 Brasil: 9
🇩🇪 Alemania: 9
🇳🇱 Holanda: 8
🇭🇷 Croacia: 7
🇺🇾 Uruguay: 7
🇲🇽 México: 6
🇨🇴 Colombia: 6
🏴 Inglaterra: 6
🇨🇭 Suiza: 5
🇵🇹 Portugal: 5
🇸🇪 Suecia: 4
🧠 Hypertonic Saline or Mannitol for Cerebral Edema?
Cerebral edema and intracranial hypertension remain among the most common life-threatening problems in neurocritical care. The Neurocritical Care Society guideline provides several practical bedside recommendations.
🔹 Hypertonic saline (HTS) is generally preferred over mannitol for acute ICP control in TBI and intracerebral hemorrhage due to more reliable and sustained ICP reduction.
🔹 Both HTS and mannitol effectively reduce ICP, but neither has consistently demonstrated improved long-term neurological outcomes.
🔹 In subarachnoid hemorrhage, symptom-triggered HTS boluses are favored over targeting a specific serum sodium concentration.
🔹 In acute ischemic stroke, either HTS or mannitol may be used, but routine prophylactic mannitol administration is discouraged.
🔹 Corticosteroids should not be used for intracerebral hemorrhage, as evidence suggests no benefit and potential harm.
🔹 The major exception is bacterial meningitis, where dexamethasone reduces neurological sequelae and should be administered before or with the first antibiotic dose.
⚠️ Safety matters. Severe hypernatremia (>155–160 mEq/L) and hyperchloremia (>110–115 mEq/L) are associated with increased risk of acute kidney injury and require close monitoring.
Take-home message: Hyperosmolar therapy remains a cornerstone of cerebral edema management, but treatment should be individualized according to the underlying neurological pathology rather than pursuing arbitrary sodium targets.
#NeurocriticalCare #ICU #CriticalCare #TBI #Stroke #SAH #ICH #CerebralEdema #HypertonicSaline #Mannitol #NeuroICU
Reference 📚
Cook AM, Jones GM, Hawryluk GWJ, et al. Guidelines for the Acute Treatment of Cerebral Edema in Neurocritical Care Patients. Neurocrit Care. 2020;32:647-666. DOI: 10.1007/s12028-020-00959-7.
🧠Intracranial pressure management is not “give mannitol and hyperventilate.”
It is a structured prevention of secondary brain injury.
Recent PubMed indexed literature reinforces a tiered approach: protect oxygenation, ventilation, venous drainage, perfusion pressure, temperature, sodium, seizures, sedation, and then escalate to hyperosmolar therapy, CSF drainage, surgery, and advanced multimodal monitoring when needed (Viarasilpa et al., 2024).
First principles matter. Head elevation 30 to 45°, neutral neck position, avoidance of hypoxia, hypotension, fever, seizures, hyponatremia, excessive suctioning, coughing, and ventilator dyssynchrony may be as important as rescue osmotherapy.
Hyperosmolar therapy remains central. Common rescue doses include mannitol 20 percent at 0.5 to 1 g/kg/DOSE IV over 5 to 15 minutes, or hypertonic saline such as 3% NaCl 150 mL over 10 to 30 minutes, or 23.4% NaCl 30 to 60 mL in selected severe crises (Viarasilpa et al., 2024). A 2024 meta analysis found that hypertonic saline and mannitol both reduce ICP, with similar mortality and neurological outcomes, although hypertonic saline may have longer effect duration and shorter ICU stay (Karamian et al., 2024).
Ventilation must protect both lung and brain. Avoid hypoxemia and severe hypercapnia. PaCO₂ around 35 to 38 mmHg is often targeted during ICP crisis; BRIEF hyperventilation may be a bridge in impending herniation, not a chronic strategy (Viarasilpa et al., 2024).
Hemodynamics are brain therapy. CPP is usually targeted around 60 to 70 mmHg in severe TBI, but newer data support individualized CPP guided by autoregulation and multimodal monitoring when available (Bögli et al., 2025).
Refer urgently to neurosurgery when there is mass lesion, hematoma, hydrocephalus, refractory ICP, herniation syndrome, deteriorating pupils, or need for EVD or decompressive surgery.
Always ask yourself, is the brain perfused, oxygenated, decompressed, electrically controlled, and still salvageable?
#ICU #NeurocriticalCare #TBI #IntracranialPressure #CPP #HypertonicSaline #Mannitol #MechanicalVentilation #Neurosurgery #CriticalCareReferences
Bögli, S. Y., Donnelly, J., Ercole, A., et al. (2025). Cerebral perfusion pressure targets after traumatic brain injury: A reappraisal. Critical Care, 29, 192. https://t.co/A3YKMa5OVN
Karamian, A., Seifi, A., & Lucke-Wold, B. (2024). Comparing the effects of mannitol and hypertonic saline in severe traumatic brain injury patients with elevated intracranial pressure: A systematic review and meta-analysis. Neurological Research, 46(9), 883–892. https://t.co/VPqChBkvv2
Viarasilpa, T., Mayer, S. A., & Francoeur, C. L. (2024). Managing intracranial pressure crisis. Current Neurology and Neuroscience Reports, 24, 873–883. https://t.co/0hhCBvXXQN
🤓ICU POCUS should not be learned as “views.” It should be learned as progressive clinical responsibility.
Recent PubMed indexed guidance supports critical care ultrasonography as a bedside tool for septic shock, acute dyspnea or respiratory failure, volume management, and cardiogenic shock (Díaz-Gómez et al., 2025). A 2024 meta analysis also suggests POCUS guided resuscitation may reduce 28 day mortality, vasoactive drug duration, and renal replacement therapy use, although evidence quality remains variable (Basmaji et al., 2024).
A practical ICU curriculum could be divided into levels.
Before entering to ICU: know machine handling, probe selection, image optimization, lung sliding, pleural effusion, basic IVC, free fluid, bladder, DVT compression, FAST and ultrasound guided vascular access.
ICU resident: add structured lung ultrasound, focused cardiac ultrasound, LV/RV function, pericardial effusion, shock phenotyping, fluid tolerance, congestion, pneumothorax, diaphragm ultrasound, ONSD and procedural guidance.
ICU specialist: integrate heart lung vein ultrasound into decisions: fluids, vasopressors, inotropes, ventilation, PEEP, weaning, RV failure, tamponade, pulmonary embolism, TCD, ARDS, and cardiorenal congestion.
Specialized ICU: advanced echocardiography, TEE, strain, advanced TCD, complex valvular disease, mechanical circulatory support, ECMO cannulation and troubleshooting, and quality assurance.
The danger is not using ultrasound. The danger is using ultrasound without competence, supervision, documentation, and clinical integration.
Best practice documents emphasize structured training, competency assessment, image archiving, quality assurance, and local governance (Oto et al., 2024; Patrawalla et al., 2025).
The key question is not:
“Can you obtain the image?”
It is:
Can you acquire it, interpret it, and safely change management because of it?
#ICU #CriticalCare #POCUS #Ultrasound #FOCUS #LungUltrasound #Hemodynamics #Shock #MedicalEducation #PatientSafety
References 📚
Basmaji, J., et al. (2024). The impact of point-of-care ultrasound-guided resuscitation on clinical outcomes in critically ill patients: A systematic review and meta-analysis. Critical Care Medicine. https://t.co/HLHERp2BsJ
Díaz-Gómez, J. L., Sharif, S., Ablordeppey, E., et al. (2025). Society of Critical Care Medicine guidelines on adult critical care ultrasonography: Focused update 2024. Critical Care Medicine, 53(2), e447–e458. https://t.co/LLyXUCdqu4
Oto, B., et al. (2024). Best practices for point of care ultrasound. Ultrasound Journal, 16, 15. https://t.co/I2wkLgUpJl
Patrawalla, P., et al. (2025). Best practices for a competency-based curriculum in critical care ultrasonography. Chest. https://t.co/mtdLj6opqj
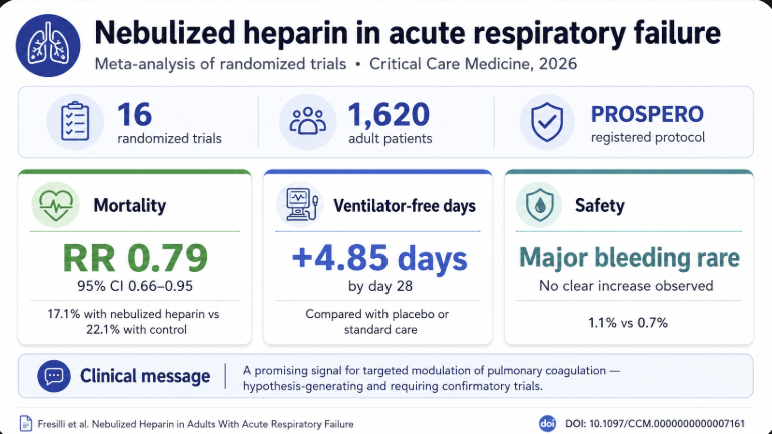
New in @CritCareMed: our meta-analysis of 16 RCTs (1,620 adults) suggests nebulized heparin in acute respiratory failure may lower mortality (RR 0.79, 95% CI 0.66–0.95) and increase ventilation-free days, with no safety signal. https://t.co/PcEnM7kpEn
Lung Volumes & Capacities: The Clinical Story Behind the Numbers
Most students memorize:
TV = 500 mL
FRC = RV + ERV
VC = IRV + TV + ERV
TLC = VC + RV
…and then forget why any of it matters.
The USMLE, ICU, anesthesia, ENT airway management, sleep medicine, pulmonary medicine, and emergency medicine all care about these numbers because they describe what the lungs are physically capable of doing.
Think of the lung as a reservoir.
TV = what you normally use
IRV = emergency reserve above normal
ERV = emergency reserve below normal
RV = untouchable reserve that keeps alveoli open
Everything else is built from these.
---
Case 1: The Healthy Medical Student
A 24-year-old MBBS student is sitting quietly studying.
He breathes normally.
Each breath:
≈ 500 mL
This is:
Tidal Volume (TV)
Definition:
Air entering and leaving lungs during quiet breathing.
Normal:
≈ 500 mL
≈ 6–8 mL/kg
Why this matters
Ventilators are initially set using tidal volume.
ARDS guidelines:
6 mL/kg ideal body weight.
Too high:
volutrauma
barotrauma
pneumothorax
Too low:
hypoventilation
hypercapnia
USMLE favorite:
> Tidal volume remains relatively preserved early in many lung diseases.
---
Case 2: The Athlete Sprinting for a Bus
Same student misses his bus.
Now he takes a huge deep breath.
The air he inhaled beyond normal inspiration is:
Inspiratory Reserve Volume (IRV)
Definition:
Extra air inhaled after normal inspiration.
This is your pulmonary "backup tank."
Why it matters
IRV falls in:
Pulmonary fibrosis
Severe obesity
Pregnancy
Kyphoscoliosis
Reason:
Lungs cannot expand properly.
USMLE clue:
"Difficulty taking a deep breath"
Think reduced IRV.
---
Case 3: COPD Smoker
65-year-old smoker.
He says:
> "Doctor, I can't empty my lungs."
This is not primarily an inspiration problem.
It's an expiration problem.
Air trapping occurs.
After normal expiration he still has excessive air left.
ERV decreases.
RV increases.
This is classic COPD physiology.
---
Expiratory Reserve Volume (ERV)
Definition:
Extra air that can be expired after normal expiration.
Normal person:
Can force out a lot more air.
COPD patient:
Already trapped.
Little reserve remains.
ERV decreases.
Real-world consequence
Difficult extubation.
Difficult anesthesia.
Postoperative hypoventilation.
---
Case 4: The Asthmatic in the ER
28-year-old arrives with severe wheeze.
Chest hyperinflated.
Prolonged expiration.
Air trapping.
Large amount of gas remains inside lungs after maximal expiration.
This is:
Residual Volume (RV)
Definition:
Air remaining after maximal expiration.
Physiological purpose:
Keeps alveoli from collapsing.
Without RV:
Every breath would require reopening millions of alveoli.
Energy cost would be enormous.
---
Why RV is clinically important
RV increases in:
Asthma
COPD
Bronchiolitis
RV decreases in:
Pulmonary fibrosis
USMLE pearl:
RV is one of the few volumes that cannot be measured by simple spirometry.
Because you cannot exhale it.
---
High-Yield Exam Question
Which lung volume cannot be measured directly by spirometry?
Answer:
Residual Volume
Therefore any capacity containing RV also cannot be measured directly.
---
Case 5: The Post-Thyroidectomy Patient
ENT correlation.
After thyroidectomy a patient develops bilateral RLN palsy.
Breathing becomes shallow.
Inspiratory effort weak.
The amount of air inhaled after normal expiration falls.
This is:
Inspiratory Capacity (IC)
IC = TV + IRV
Definition:
Maximum air inspired after normal expiration.
Clinical importance
Reduced in:
Vocal cord paralysis
Neuromuscular disease
Myasthenia gravis
Guillain-Barré syndrome
Patients often describe:
> "I can't take a satisfying breath."
😴Consciousness in the ICU should not be reduced to “GCS 8.”🤔
The Glasgow Coma Scale remains useful because it is simple, familiar, reproducible, and embedded in emergency medicine, trauma, neurology, and ICU communication.But in the ICU, the classic GCS has important flaws.
The verbal component becomes untestable in intubated patients. Sedation, neuromuscular blockade, aphasia, delirium, language barriers, facial trauma, hearing impairment, and metabolic encephalopathy can all distort the score. Most importantly, GCS does not directly assess brainstem reflexes or respiratory pattern, which are central in deep coma and neurocritical care.
Recent evidence supports a more nuanced approach.
The FOUR score appears particularly useful in ICU and emergency patients because it removes the verbal component and adds brainstem reflexes, breathing pattern, eye response, and motor response. A 2025 systematic review found that both GCS and FOUR have strong reliability and validity, but FOUR showed slightly higher overall performance and may be especially suitable for ICU assessment (Brun et al., 2025). Another systematic review found FOUR may be superior to GCS for ICU mortality prediction, with better responsiveness in deeply impaired patients (Schey et al., 2025).
Sedated ICU patients require a different logic. RASS and SAS are sedation scales, not coma scales. They should be used to titrate sedation depth, while CAM ICU or ICDSC should be used when delirium is assessable. A 2025 PADIS focused update reinforces structured assessment of pain, agitation, sedation, delirium, immobility, and sleep in adult ICU patients (Lewis et al., 2025).
The 2025 French expert consensus on severe acute encephalopathy recommends using delirium scores such as CAM ICU or ICDSC, coma scores such as GCS or FOUR, and specifically suggests FOUR over GCS in coma because it better captures brainstem responses and respiratory patterns (Sonneville et al., 2025).
The practical ICU message:
Use RASS to define sedation level.
Use CAM ICU or ICDSC to detect delirium when the patient is arousable.
Use FOUR, not only GCS, in coma or intubated patients.
Use CRS R when prolonged impaired consciousness requires recovery tracking.
Do not interpret a low score without knowing sedation, analgesia, paralysis, metabolic state, and airway status.
The question is not only:
“What is the GCS?”
It is:
What is the patient’s brain doing, and what is the drug doing to the brain?
#CriticalCare #ICU #NeurocriticalCare #Consciousness #Sedation #Delirium #GCS #FOURScore #RASS #CAMICU #IntensiveCare
References
Brun, F. K.. Australian Critical Care, 38(1), 101057. https://t.co/DhIlQ6isvp
Lewis, K., Critical Care Medicine, 53(3), e711–e727. https://t.co/TiOVn3apvR
Schey, J. E., et al. (2025). Neurocritical Care. https://t.co/hdpso6BynF
Sonneville, R. Annals of Intensive Care, 15, 37. https://t.co/JKzksc2e3S