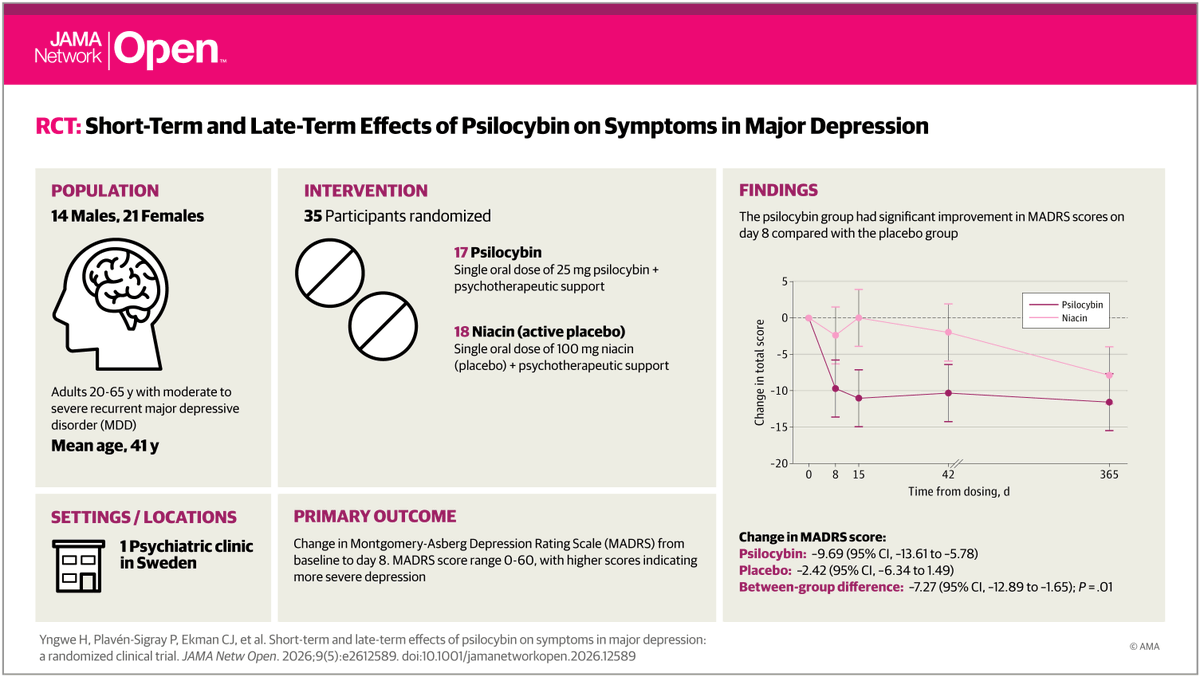
I know its repetitive and boring, but one more time to drive home the point: another #psilocybin trial on major #depression, another missing #placebo response.
This time the placebo response is merely ~2.4 points, which is less than ~1/3 of antidepressant trials. This lack of a placebo response drives the large between-arm effect (~7.3), while the patient improvement after psilocybin is a respectable, but not great, ~10 MADRS units - its about ~12 after antidepressants.
If you are in San Francisco for the @APA conference, come and see my talk this topic on Sunday from 15:45 in room 206!
The #NHS spends £570m/year on management consultants.
New JAMA study found they have essentially no effect on US hospital finances, operations, or patient outcomes.
If this were a therapy, it would be cut. So why do we keep hiring them in #healthcare?
https://t.co/gbx3PyeaIg
https://t.co/utuhfG3HgR
What happens when a survey of patient experience of ECT is representative of the population? 23 facilities in the US surveyed the experiences of 1089 people treated in 2014-15. 85.5% of patients indicated that they benefited or improved and 97.9% stated that they would recommend the facility to others in need of treatment. Let's have more surveys.
A monumental moment in medical history: the first gene therapy for genetic hearing loss is now FDA approved. As a former Regeneron scientist, I feel very proud. I had the opportunity to hear about this programme while it was still in development. It’s one of the few programmes that, every time you came across it, you felt the medical breakthrough in your bones and privileged just to be there while it was happening.
At this moment, it’s important that we look 30 years back when researchers mapped a locus on chromosome 2 to congenital deafness in a Lebanese family (https://t.co/o8ltjHyLNy). They named it DFNB6 (later DFNB9) with no clue about the responsible gene. Three years later, the causal gene came to light: OTOF, encoding a protein called otoferlin (https://t.co/tBGlFPzaQd). Seven years after that, in 2006, pioneering work by Christine Petit revealed that otoferlin is a calcium sensor in the inner hair cell membrane, acting as a molecular trigger that converts sound into electric signals that the brain can read (https://t.co/oxXtifPrTZ). Twenty years fast forward, we now have a successful treatment. Thirty years from discovery to medicine.
OTOF-related deafness is congenital, caused by complete deficiency of otoferlin. In these children, the cochlea is structurally intact, hair cells are there, the mechanics of sound transmission work. It’s just that final step, where hair cells hand off the signal to the auditory nerve through neurotransmitter release, that doesn’t happen. Sound arrives and dies at the synapse. It’s deafness due to a defect in the synapse caused by the absence of a single protein, which is what made this a beautiful, clean target for gene therapy.
The treatment itself is a feat of molecular engineering. OTOF is too large to fit in a single AAV capsid. The team solved this elegantly by delivering the gene in two halves separately, which then get spliced to produce the full functional protein. A single surgical injection into the cochlea, a molecular miracle unfolds. Results from the CHORD trial were striking: of 20 evaluable patients, including children as young as 10 months, 80% showed meaningful hearing improvement, and by 48 weeks, 42% had achieved normal hearing including the ability to hear whispers. Otarmeni is not only the first gene therapy for deafness, it’s also the first dual-AAV therapy to be approved by the FDA.
There are very few things in medicine that come close to giving back a sense like vision, hearing, or touch that a human never had from birth. It’s almost God’s work. A parent witnessing their child who was born deaf hearing their voice for the first time, it’s a joy that no words can describe. Multiply that by the fact that it came from a single injection, a repaired gene, and 30 years of science. We are truly in the golden era of medicine.
Regeneron press release:
https://t.co/6zvdsT2uzI
Below video is from the NEJM publication of CHORD trial (Valayannopoulos et al. NEJM 2025)
https://t.co/YvIqwQ0SDu
Four million physician hours are spent on mandatory modules each year. They represent not just clinical time lost but “evenings reclaimed and cognitive load reduced.”
Redundant training and low-value modules should be a thing of the past.
https://t.co/896bWbZoVQ
Among outpatients with #BorderlinePersonalityDisorder, dialectical behavior therapy and schema therapy produced similar and substantial improvements in symptoms, functioning, and quality of life, with no significant differences in treatment retention. https://t.co/yvdveKFeTh
@seanluomdphd@AllenFrancesMD Sean, we’re both psychiatrists. I’m sure we treat similar things in similar ways. Our discussion is the current risk–benefit of anti-amyloid therapies. They’re not funded across much of Europe, including the UK, for a reason. This isn’t therapeutic nihilism.
@seanluomdphd@AllenFrancesMD No, I advise my patients with dementia based on current evidence, not my ‘feelings’ about the future.
I don’t recommend intensive therapies with marginal benefits, risks and costs. Focus on what truly improves quality of life and future care.
I support trial participation.
@seanluomdphd@AllenFrancesMD I wish my feelings were so optimistic…
Sadly there’s little evidence for this potent prevention signal currently, and the drugs have serious side effects.
I also have an issue with using external historical cohorts (ADNI) as comparators. Hopefully I’m
proved wrong in future.
@seanluomdphd@AllenFrancesMD Their estimated effect is a 0.38 CDR-SB difference - similar to the small effects in approved med trials (0.45 CLARITY-AD).
These are not clinically meaningful.
If this seems dodgy, just check out what the ~20% “prevention” signal is based on:
https://t.co/Ojkj8XD41S
@seanluomdphd@AllenFrancesMD Antibodies are no justification for validity of MCI diagnosis.
Amyloid monoclonals have marginal effects on cognition and significant risks of brain swelling and micro haemorrhage.
I wouldn’t advise any patient or family member with MCI to go on them.
https://t.co/fl63PpX2T2
Our paper is out: By analysing health records from millions of real-world patients from the literature, we can now finally answer the questions about the long-term outcomes of ECT. What we found, consistently, across well-designed studies from the UK, Canada, US, Sweden, Denmark, and Taiwan, is that ECT does not increase the risk for dementia, heart attacks or stroke, and is associated with a significant reduction in overall mortality.
https://t.co/lC13i5ANBD
This gorgeous story of "severe morning sickness" continues to have surprising new chapters, and is a testament to the maternal instinct as a force of Nature - the senior author (Marlena Fejzo) suffered from hyperemesis gravidarum and left no stone unturned in a search for what caused it. Beautiful!
A new paper in @Nature from David Reich, @aliakbari23 and colleagues breaks the conventional understanding of recent human evolution. The field believed that strong selection in the recent past (~10,000 years) was rare, with few exceptions like the lactase persistence locus. In this paper, the authors challenge that belief, showing that we weren't looking at the problem right.
Previous studies that looked for evidence of selection using ancient DNA addressed the problem cross-sectionally, asking if allele frequencies differed across populations more than what one would expect based on genetic drift and migration. Most arrived at the conclusion that population structure primarily explained the observed differences. Here, the authors addressed the problem longitudinally, accounting for when ancient individuals lived by explicitly modeling time as a variable in the analysis. It turns out doing it this way dramatically increases power, increasing the number of genome-wide significant selection signals by 20-fold!
Looking at why accounting for the time variable led to such dramatic changes in results, the authors find that previous studies missed so much because selection often happened not on new variants leading to dramatic sweeps (the conventional model: new variant -> selection -> increase in frequency) but on already existing variants driven by transient environmental pressures. Many of these variants underwent reversals, selected up when a pressure existed, then purged when it disappeared or the trade-off cost became dominant. A great example is the TYK2 variant, where an allele boosting immunity was selected for thousands of years because it protected against TB, then got purged as TB endemicity declined and the autoimmune cost took over.
The scale of what they found is striking: hundreds of loci showing strong selection in the past 10,000 years with a median selection coefficient of ~0.86%. This number is pretty big in evolutionary terms, meaning allele frequencies have been shifting by ~1% per generation in a consistent direction. Previous selection scans found a maximum of 20 loci, and this one finds hundreds. That isn't an incremental change. It fundamentally reframes our understanding of how common strong selection has been in recent human history.
Some of the most striking findings come from polygenic selection, where hundreds of small-effect alleles were pushed in the same direction simultaneously. Polygenic scores based on large-scale GWAS of today predict recent negative selection for traits like body fat, waist circumference and schizophrenia, and positive selection for others like cognitive traits. One important caveat is that GWAS phenotypes are measured in industrialized societies today, and how well they capture what was actually being selected in ancient environments is debatable.
For me personally, these findings have direct implications for drug discovery. When using human genetics to find drug targets, we often fixate on the benefit and risk profiles of variants visible today. But we need to be aware that a variant's benefit:harm ratio might be environmentally contingent, and could reverse when the wrong environment manifests. An evolutionary understanding of a variant's association with traits is therefore essential.
The same logic applies, perhaps even more urgently, to embryo selection. Selecting embryos based on polygenic traits is humans making permanent, heritable decisions for their offspring with a narrow view of today's environment. The ancient DNA record now shows that cost-benefit landscapes flip over time. So, an embryo carrying man-made selections is carrying those changes into an unpredictable future environment.
The broader takeaway is that human evolution didn't freeze in the last 10,000 years. We just lacked the tools and datasets to see its movement. The current findings are based on European populations. I am curious to see these analyses extended to other populations too, like South Asian, East Asian and African populations, which might be holding more surprises to blow our minds.
Akbari et al. Nature 2026
https://t.co/3WWjpTiVgA
74% of people who stopped clozapine because of neutropenia were successfully rechallenged. Only 7% had another episode of neutropenia. https://t.co/1Tb3uP8gZS
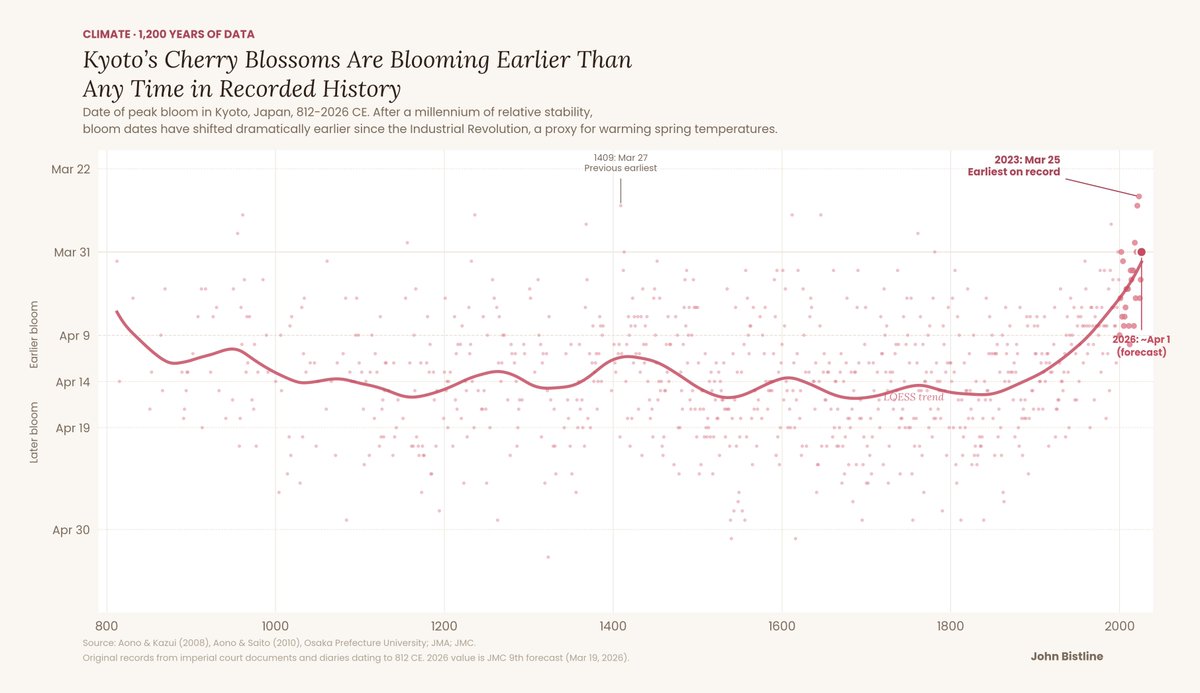
This is my favorite climate change chart. Japanese monks, aristocrats, and emperors kept meticulous records of cherry blossom festivals for 1,200 years and accidentally built the world's longest climate dataset.
The cholesterol wars are over.
LDL won.
New guidelines. Four landmark trials. An oral PCSK9 inhibitor that matches injectables. And data proving we should be treating patients we currently aren't.
Here's everything clinicians need to know. 🧵
Among individuals with severe, treatment-resistant #Schizophrenia, #dementia was common and showed a distinct clinical and genetic profile not explained by #Alzheimer disease, cardiovascular risk, or medication effects.
https://t.co/hkz7MoIENa
✨New Paper✨"Regional Blood Flow Signatures of Opioidergic Modulation of Ketamine in Major Depressive Disorder: A Randomized Crossover Study" | American Journal of Psychiatry https://t.co/qQEecP2DLV