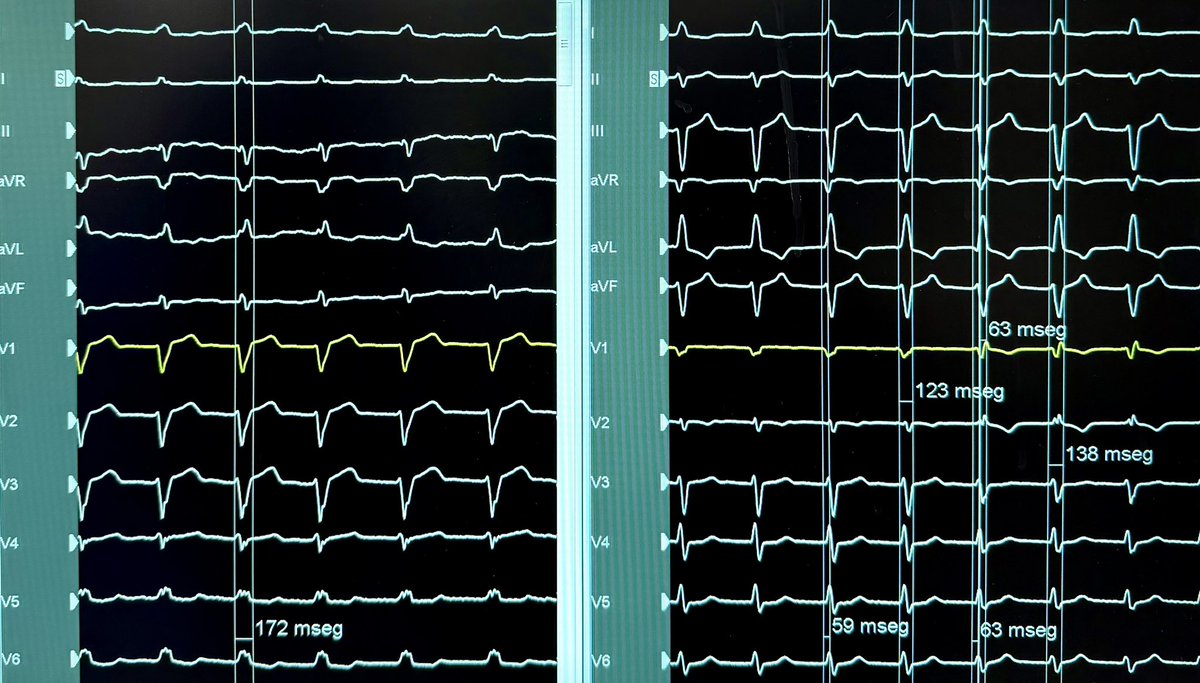
@SzymkiewiczPJ@kellych11 The same general CSP capture criteria. Especially the RWPT (<100 ms in LBBB), the change in QRS width and the transition from non-selective to selective capture during the threshold test.
52 yo M. Non-ischemic DCM. LVEF 22% and LBBB. #CSP
Done with @kellych11
Interesting to get the best QRS by modifying the AV interval in #LBBP. Thus allowing a fusion with the intrinsic conduction of the RBB
Syncope, first grade AV block and LBBB. Paroxysmal Complete AVB during monitoring. #CSP
Done with @kellych11
NS-LBBP and S-LBBP during the threshold test in bipolar mode
🔍 #EHRATopicWeek on Atrial Tachycardias
Atrial Tachycardia is more complex than we once thought
Traditionally, rapid regular atrial arrhythmias were divided into “atrial tachycardia” and “atrial flutter” based mainly on ECG appearance. Today, high-resolution mapping shows these distinctions are often oversimplified.
📌 Current concepts classify all regular atrial rhythms >100 bpm as AT:
• Non-reentrant AT
• Reentrant AT (localized or macro-reentrant)
Importantly, many arrhythmias previously labeled as “flutter” may actually represent different AT mechanisms.
⚡ Differentiating AT from organized AF can be challenging, especially in scarred atria or after ablation. ECGs, EP studies, intracardiac mapping, and even wearable devices all play an important role in diagnosis.
💡 Precise classification matters — for diagnosis, treatment strategy, and improving ablation outcomes.
Find out more in the #EHRA_ESC Consensus document on Management of patients with atrial tachycardia 🔗https://t.co/T5EGaHI51q
@escardio@EuropaceEiC
More than 10 years ago Oussama and I started our journey of investigation, trying to the define the optimal first treatment for patients with atrial fibrillation.
Separately we pursed randomised studies in populations with treatment-naive paroxysmal AF.
Five years ago we presented our RCTs in the paroxysmal AF population, which ended up sitting side by side in the same issue of the New England Journal of Medicine.
https://t.co/DWgHQ2VhiJ
https://t.co/z346xqq0jg
Since then we have been working together to examine the same question of optimal initial therapy, but instead looking at patients with more advanced forms of atrial fibrillation.
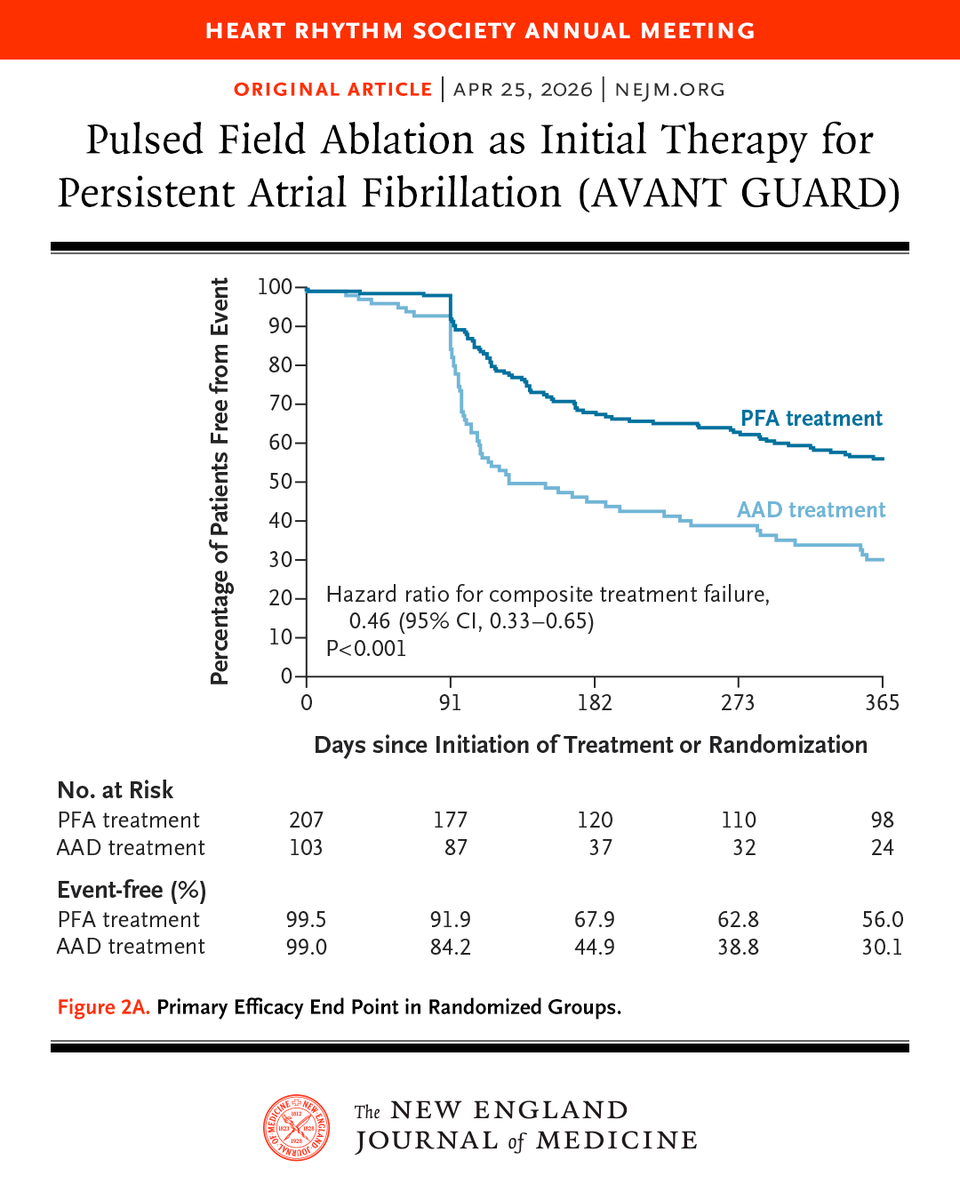
Today Oussama presented the results of the AVANT-GUARD study, which definitively demonstrated the value of initial catheter ablation in the treatment naive persistent AF population.
Like EARLY-AF, AVAT GUARD used implantable cardiac monitors to evaluate arrhythmia endpoints
Like EARLY-AF - initial catheter ablation reduced recurrences in AVANT GUARD by about 50%, which was about 25% in absolute terms. To put this another way, only 4 patients need to be treated with ablation to prevent a recurrence of arrhythmia.
However, binary recurrence doesn’t tell the whole story. Because we had loop recorders we were able to assess the time spent in AF (or AF burden). In this regard significantly more patients had none or negligible burden after ablation (<0.1%), with significantly more AAD treated patients having a very high burden (>5%). This is important as AF burden is associated with clinical outcomes such as hospitalisation.
In terms of risk - the rates of any adverse event or serious adverse event were comparable between randomised arms. Highlighting that persistent AF patients with high CHADS-VASc score are high risk irrespective of treatment provided. This is important as we reflect on treatment options as part of shared decision-making.
Congratulations to Oussama for the presentation and leadership, to the co-investigators and study sites for their participation and dedication, and a huge thank you to the Boston Scientific team for their support and commitment to advancing science.
To end, I want to acknowledge and thank Oussama for this shared journey, I’m grateful for our collaboration and friendship, and look forward to what we will do next.
Presented at #HRS2026:
In patients with persistent atrial fibrillation, first-line treatment with pulsed field ablation reduced the recurrence of atrial arrhythmias at 12 months as compared with antiarrhythmic drugs. Full AVANT GUARD trial results: https://t.co/milHy26ojJ
@HRSonline
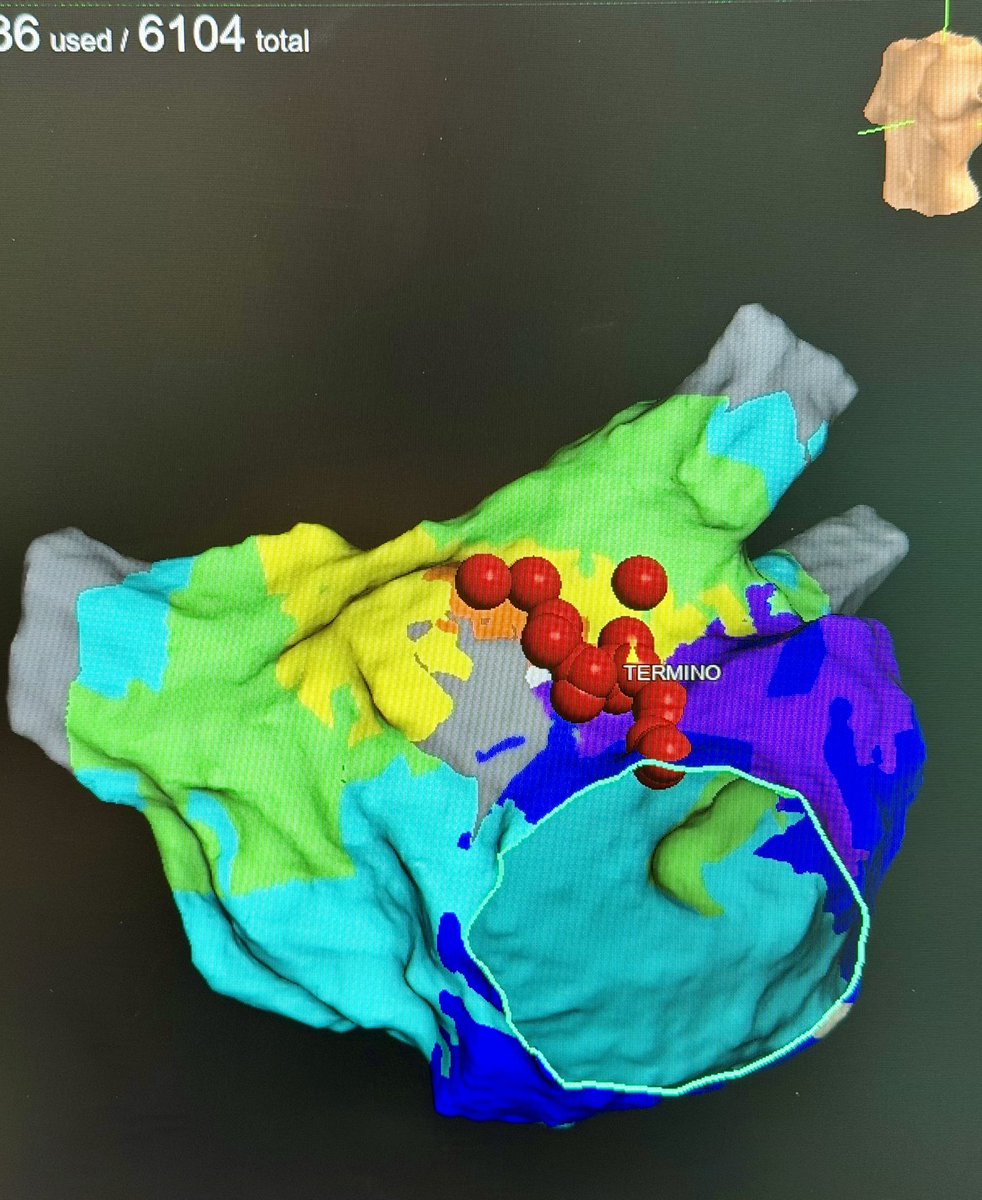
Successful ablation from the posteromedial papillary muscle.
It seems that the catheter is floating and sometimes it is difficult to maintain a stable contact