Different surgical techniques can result in a stable knee. This study compared a novel ITB + gracilis tendon technique against the most common hamstring + LET technique for ACLR.
#knee#ACL#reconstruction#clinicalstudies#KSSTA
Read here: https://t.co/I4uIZNbk8Q
Leaky wounds and dressings are topics not frequently heard in meetings.
In this KSSTA (open access)article , the authors describe an algorithm for leaky wounds. They achieved a commendable >90% success in preventing a DAIR.
I use iNPWT frequently.
https://t.co/O0NuwKKh1F
As augmented repairs increasingly become the standard for large/massive cuffs, there are a lot of different options to consider. Check out this technique for a nanofiber patch as an interpositional scaffold. Full video at https://t.co/wxSeUaECKm #rotatorcuff#cuffrepair#biologic
Un usuario de MacBook acaba de descubrir que puede escribir con la voz al pulsar dos veces la tecla de función. "¡Hace años, esto habría sido un gran ahorro de tiempo!" 🥹
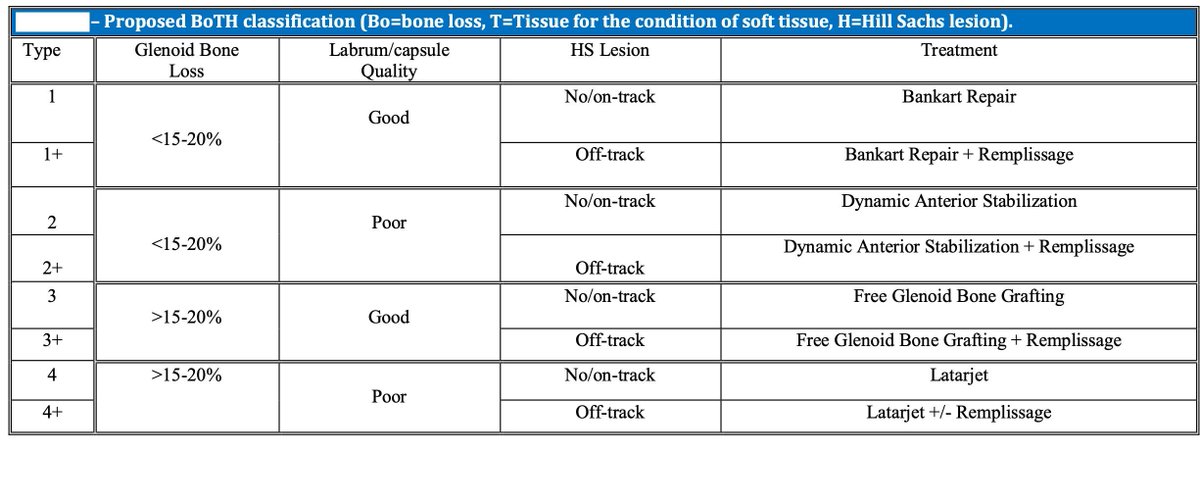
the BoTH classification for shoulder instability. This system focuses on three key aspects:
Bo: Bone loss
T: Condition of soft tissue
H: Hill-Sachs lesion (a type of bone injury that occurs in some cases of shoulder dislocation)
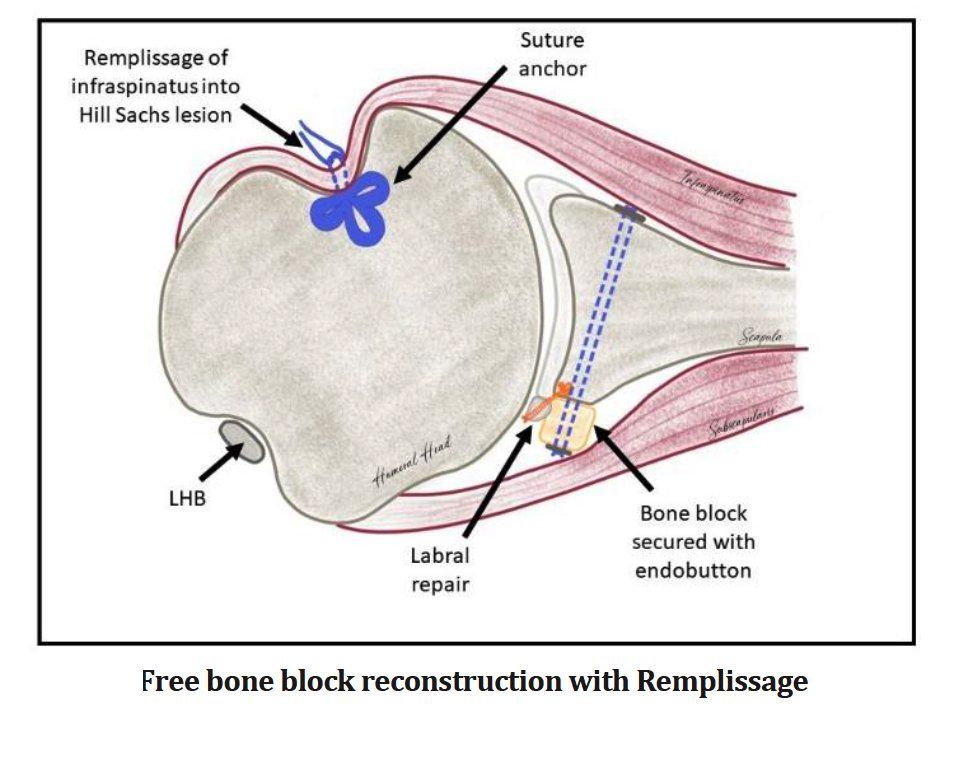
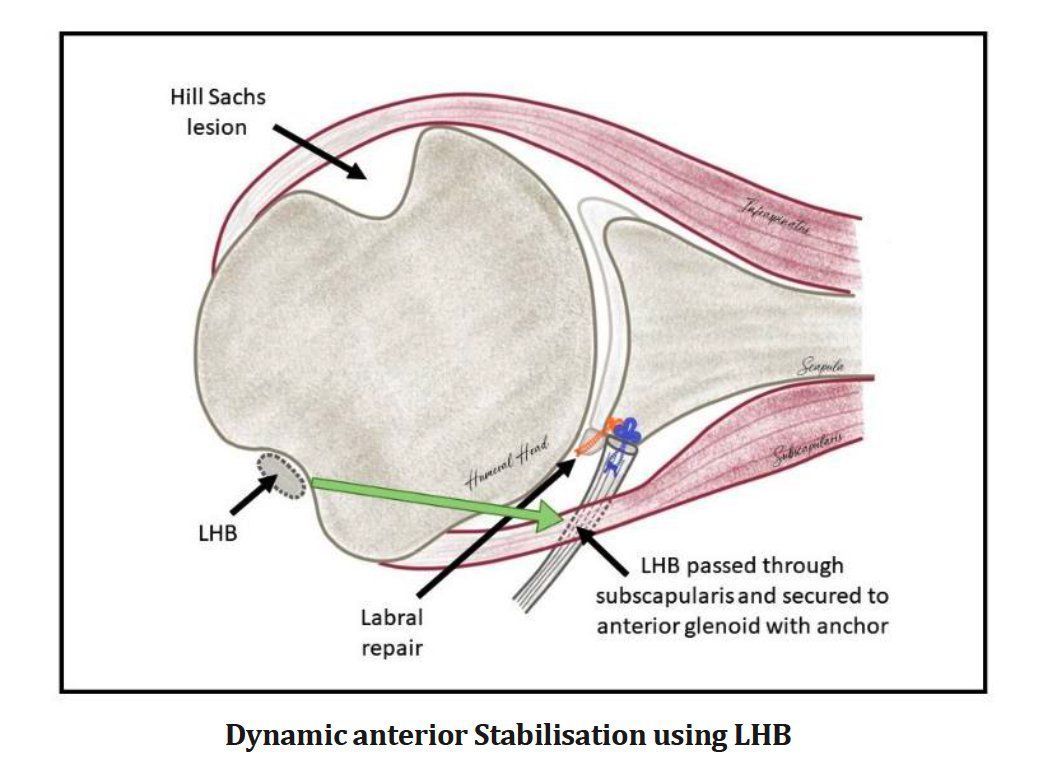
By incorporating these modern techniques, the BoTH classification system provides a more comprehensive approach to determining the best treatment path for each patient.
Read the whole paper: https://t.co/uL6qkOhThA
This cadaveric model investigation found that anteriorly shifted #LET insertion point restored internal tibial rotation after anterolateral insufficiency to the native state while decreasing the overconstraint of internal tibial rotation #Lemaire#Knee#Arthroscopy
The Lasègue test, or Straight Leg Raise Test (SLR), is one of the most commonly used maneuvers in clinical evaluation of sciatica pain and lumbar radicolopathy. This test is based on the tension of the sciatic nerve and its peripheral branches (tibial nerve and peroneal nerve), providing a clear indication of possible compression at the level of the lombosacral nerve roots.
How is the test performed ?
The patient is in superior position. Therapist passively lifts the extended lower limb while keeping the extended knee. The angle of elevation is between 40° and 50°, because at this stage the sciatic nerve enters maximum tension. If the patient reports pain radiated along the sciatic nerve course, the test is positive and suggests possible compression or root irritation.
Awareness test: foot reflexion
To increase the specifics of the test, the clinician may add a passive dissipation of the foot. This gesture causes a further stretching of the sciatic nerve, intensifying the pain in case of nerve irritation.
Why is it important ?
If dorsiflexion increases pain, the likelihood of lumbar radicolopathy increases. Instead, if the pain remains unchanged or is located only at the lumbar level, it could be a musculoskeletal or myofascial dysfunction (for example, piriform syndrome or better sciatic-pelvic functional neuropathy*).
What does the Lasègue test say to us?
Pain between 30° and 70° elevation → possible lumbar disc hernia compressing the root of L4-L5 or L5-S1.
Pain above 70° → less likely root involvement; could be ischiocrural muscle tension.
Pain that reduces by flexion of the knee → probable involvement of the sciatic nerve and not other muscle structures.
Link with the lumbar root diseases
As shown in the image, a protrusion or herniated disc between L4 and L5 can compress the L5 nerve root, causing pain radiated down the course of the sciatic nerve to the foot.
Common symptoms associated with L5 radicolopathy
Lower back pain radiating down the lateral face of the thigh and leg.
Deficiency of dissipation of the tooth and the foot.
Alterations of the sensitivity in the back of the foot.
If instead the hernia involves L5-S1, the pain radiates down the back of the thigh and leg up to the lateral margin of the foot.
Is Lasègue's test enough for diagnosis?
Nope! Lasègue’s test is an indicator of radical suffering, but alone is not enough to make a diagnosis. It must be associated with other neurological tests (reflexes, muscle strength, dermatomeric sensitivity assessment) and, if necessary, confirmed with imaging (lumbar RM).
Conclusion
The Lasègue test is a fundamental tool in the assessment of lumbosciatalgic pain, allowing to differentiate between a problem of nerve origin and musculoskeletal dysfunction. However, it should always be interpreted in a broader clinical context to avoid misdiagnosis and inappropriate treatment.