Deep gluteal syndrome: role of ultrasound in its diagnosis
A 54-year-old patient with left paravertebral low back pain with gluteal and lower limb radiation of 16 months' duration. In the MRI of the hemipelvis, a fibrous band can be seen that is attached to the anterior face of the sciatic nerve, extending laterally to the greater trochanter and medially to the ischial tuberosity and the quadratus femoris muscle, corresponding to type 3 of the Hernando classification.
Dynamic ultrasound is performed, which shows reduced mobility of the sciatic nerve during knee and hip extension (comparative video of normal neural mobility: https://t.co/NiqvUemcdL).
Ultrasound has little value for the primary diagnosis of visualization of perineural fibrous bands, although it can often be appreciated a posteriori, guided by the findings in MRI. This could be useful for realizing fenestrations of the fibrosis after perineural infiltration using ultrasound control.
The great utility of ultrasound is the assessment of the mobility of the sciatic nerve during neurodynamic exercises, which in cases where it is decreased compared to the contralateral nerve, can be used as a secondary sign for the diagnosis of DGS.
Posterior parietal insufficiency of the inguinal canal (sport hernia): ultrasound diagnosis
The patient has had left pubic and groin pain for three months, which prevents him from hitting and changing direction while playing soccer.
On examination, he presented pain along the inguinal canal, at the insertion of the inguinal ligament on the pubic tubercle, and the insertion of the oblique and transverse muscles on the iliac crest.
To rule out sport hernia, a dynamic ultrasound of the left inguinal canal is performed during Russian twist exercise (which mainly exercises the internal oblique muscle), observing deformity and bulging of the posterior wall of the inguinal canal, unlike the asymptomatic contralateral side.
The patient is referred to the abdominal wall surgery service, which performs an operation that confirms the clinical and ultrasound diagnosis.
Save the date for our 2024 Annual Scientific Meeting!
⨠ Stay tuned for updates at https://t.co/jXKGRL8pSd
🍁
Rendez-vous en 2024 pour la Réunion scientifique annuelle!
⨠ Restez à l’affût des nouveautés sur https://t.co/jXKGRL8pSd
#CanadianPain24#DouleurCanada24
Join us tomorrow November 17th at 815 AM in the Learning center for a live hands on scanning session on Shoulder Ultrasound. @AAPMR @AAPhysiatrists #AAPMR2023
MRI guide to locate the inferior calcaneal nerve, first branch of the lateral plantar nerve (Baxter’s nerve).
There are three possible entrapment sites:
1. Deep or adjacent to the fascial border of a hypertrophied abductor hallucis muscle.
2. Along the medial border of the quadratus plantae muscle.
3. Adjacent to the medial calcaneal tuberosity.
Next, US.
#mskrad
Medial meniscus extrusion is a common painful condition in early knee ostheoarthritis. If correctly diagnosed as the main pain source, ultrasound-guided perimeniscal injection therapy may be helpful!
How and why?
A short thread 🧵
1/n
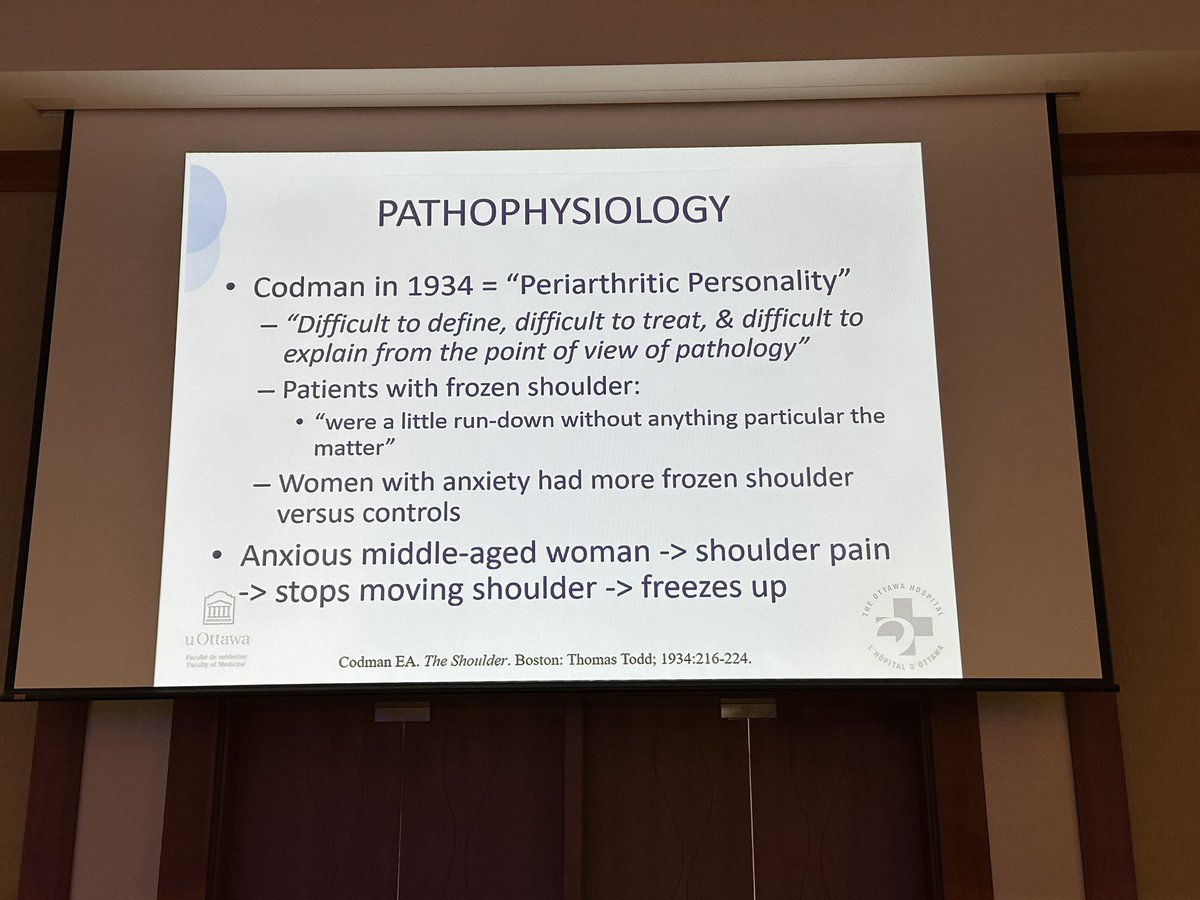
Omg! Frozen shoulder in the 1930’s was thought to be due to “run down histrionic ”women in the literature!!! #adhesive capsulitis. Listening to the expert Dr Jennifer McDonald. @JenniferKShea
Barbotage of calcific tendinopathy (pics from today) is valuable US guided procedure.
Generally, calcific deposits more than 5mm linear width and posterior acoustic shadow are amenable to barbotage. Come join to learn at USG workshop CAPMR 2023 meeting. https://t.co/1laQMeYs0M
@PetitDerek@DrJesseMorse “The little prongs here” are transverse processes (not facet joints). The described “tail bone” is the sacrum.
Had to stop there- didn’t make it to the end.
Let me guess- PRP/stem cells to target the “weak ligaments” is the cure?
@TJQPNI@MismatchN There is axonal loss given the muscle atrophy. I would be shocked if deltoid is normal on EMG. I also see ? Myokymia posteriorly in ? teres major- that is not normally innervated muscle.