Andrew and I are in Washington, D.C. today, where I had the honor of testifying before the FDA on behalf of cancer patients everywhere.
We’re fighting to bring #ANKTIVA and natural killer (NK) cell therapies into the spotlight, giving hope and new options to those who need them most.
Please watch the testimony. I hope it resonates with you.
Together, we’re pushing for real progress. @bullishbruk@DrPatrick
If you missed the FDA hearing about the Commissioner’s National Priority Voucher Program where @LoriMills4CA42 I gave comments, here is what I said:
Good afternoon, distinguished panelists and members of the FDA. As Henry Ford said: “We need a faster horse.”
My name is Karol Hansen. I am a Stage IV breast cancer patient with Mets to the bones. I have been fighting cancer for 10 years. In that time, I have undergone chemotherapy twice, radiation three times, and more than 25 surgeries. The cancer has recurred over 11 times.
10 years ago, Nuelasta was prescribed to me before I even had neutropenia because it’s medically known that chemotherapy causes Netropenia. Neutrophils are an inherent part of the body’s immune system that provide rapid, broad, innate protection against infection and injury. Lymphocytes form the core of the adaptive immune system and are responsible for precise, targeted and long-lasting immunity.
Neulasta, and its biosimilars, is given prophylactically to protect neutrophils. ANK TIVA, manufactured by Immunity Bio in California protects lymphocytes, but it is NOT YET approved by the FDA for all cancer types.
During these years of relentless treatment my Absolute Lymphocyte Count remains critically low — below the threshold associated with increased infections, weakness, treatment failure, and shortened survival. There are millions of cancer patients whose ALC looks just like mine. RIGHT NOW, at the Chan Soon-Shiong Institute for Medicine there are 15,000 patients waiting in line to receive ANK TIVA.
ANK TIVA is the first therapy designed to restore and activate lymphocytes through its IL-15 mechanism. It is the missing piece of immune boosting protection — ANK TIVA is the equivalent to lymphocytes as Neulasta is to neutrophils.
I have intractable, treatment-resistant cancer that has failed standard therapies. If ANK TIVA had been available as standard supportive care a decade ago, I might have been spared years of immune collapse, repeated recurrences, and the physical and emotional toll of more than 25 surgeries. Now I am out of time, out of strength and out of options. The 15,000 patients waiting for ANK TIVA can only get it if an opening is available in a narrow group of clinical trials or through the Extended Access Program, which the clinic has to process one at a time, on a case by case basis. A VERY SLOW process. It took almost a year for me to get approved. That’s not POLITICS, that’s imminent death for critically ill patients.
Ladies and gentlemen, we HAVE the cart, which is ANK TIVA. But, as Henry Ford said, “WE NEED A FASTER HORSE!” The Commissioner’s National Priority Voucher Program IS THAT FASTER HORSE!
Immunity Bio is delivering groundbreaking immune-restoring therapy of ANK TIVA but the FDA needs to approve it as a first line of defense for patients with lymphopenia.
The CNPV Program was created to accelerate exactly these kinds of innovative therapies that address critical unmet needs and can transform patient outcomes. I urge the FDA to prioritize ANK TIVA for full approval and label expansion so that every cancer patient undergoing chemotherapy or radiation can receive lymphocyte support proactively — not as a desperate final measure after years of fighting for survival.
It is TIME for a faster horse at the FDA. Streamline the review process. Provide a patient conduit directly to CNPV. Give us a voice. Speed up access to ANK TIVA. Give future patients the CHANCE at a fuller life that I, and others who have died while waiting, have been denied.
Thank you for listening to my story and for the work you do every day on behalf of patients like me
Is ANKTIVA the next big longevity drug?
Dr. Robert Lufkin breaks down how this FDA-approved IL-15 superagonist (from Dr. Patrick Soon-Shiong) could combat lymphopenia, boost immune function, and target multiple hallmarks of aging — beyond its current use in bladder cancer. @bullishbruk@DrPatrick
Watch here: https://t.co/Bxlyv3nG1R
So what is next on the NantWorks platform as we emerge from 15 years of stealth. Remember Diabetes? Remember Abraxane..albumin bound paclitaxel. Well imagine Albumin linked GLIP-1 at one tenth of the dose? This is the program now nearing completion at Nantworks and trials completed ex -USA. Will share news over the next 6 months
New MiNK data presented at #ATS2026 and published in Clinical Immunology Communications showed pathogen suppression, lung immune-cell recruitment and tissue repair pathway activation following sequential agenT-797 + Anktiva® (N-803).
Read more: https://t.co/JEtcHAWLQX
$INKT #ARDS #iNKT
I am really wondering what the FDA is going to do now.
Will it give approval to bladder cancer in situ? Will the FDA act soon, or will it delay the only logical decision as long as possible - again?
Does the FDA plan to regain its former status of an independent regulator? Or do they really not care what the public thinks of them?
Emerging NSCLC data are adding to the growing evidence that ANKTIVA and the broader $IBRX immune-restoration platform may be much more than a niche bladder cancer story.
Recent NSCLC data showed:
• Objective response rate improved to 56% vs 33% • Median overall survival improved to 34.7 months vs 20.2 months • Hazard ratio around 0.5 • No major increase in adverse events
Even more interesting, the mechanism may not simply be “tumor killing,” but immune restoration itself:
• reversal of lymphopenia • restoration of NK/T-cell activity • broader immune reactivation
ASCO26 data across bladder cancer, GBM, and NSCLC are starting to make the “one indication story” look increasingly outdated.
The emerging thesis may be far bigger:
not just oncology, but immune restoration across multiple disease settings involving immune dysfunction.
Great news for cancer patients and long-term $IBRX investors.
Thank you @DrPatrick and the entire ImmunityBio team for pushing this science forward.
#ASCO26
#IBRX
#CancerResearch
#Immunotherapy
#NSCLC
#GBM
Same Clone, Different Code
The FDA's own experts just demolished the regulatory fiction that kept me from my drug.
In March I wrote about what I called the Bladder Preservation Tax — the toll extracted from cancer patients by the distance between settled science and regulatory action. I am a fifty-one-year-old attorney in North Carolina, seven consecutive cystoscopies clear, alive with my bladder intact because of an immunotherapy called Anktiva — the first meaningful improvement to BCG, the intravesical immunotherapy that has been the standard of care for bladder cancer, in nearly fifty years — and a two-month guerrilla campaign against my own insurer to obtain it. I described the insurance denials, the appeals, the Orwellian phone calls, the two-floor elevator ride from the urologist who prescribed the drug to the oncology department that was the only place financially capable of administering it. I described a system that rewards intermediaries for complexity and punishes patients for biology.
On May 18, the FDA held a workshop that proved my case more efficiently than I ever could. On May 19, the agency accepted ImmunityBio's application to approve the drug for patients with my exact disease — and gave itself until January 6, 2027 to decide. I have thoughts about that timeline.
The workshop was titled, with the bureaucratic poetry only a federal agency can muster, "Contemporary Issues in Non-Muscle Invasive Bladder Cancer Trial Design and Interpretation." What it actually was, to anyone paying attention, was the FDA's own invited witnesses testifying against the FDA's own regulatory position. The panelists — thought leaders in the field, the physicians who actually treat this disease — told the agency three things, each more damaging than the last to the distinction the FDA has maintained since Anktiva's original approval in April 2024.
First, they told the FDA that carcinoma in situ and papillary disease arise from the same cancer-inducing clone. They are not two diseases. They are two phenotypic expressions of one disease — CIS being the flat form, papillary being the raised, grape-like form that may simply represent a further growth phase from CIS that was never identified. Same clone. Same biology. Same disease. The regulatory line the FDA has drawn between them is not a scientific boundary. It is an administrative convenience that became an administrative prison for approximately 80,000 Americans diagnosed with papillary bladder cancer each year.
Second, they revealed a statistic that should embarrass every stakeholder in this system: only approximately 6% of urologists in the United States use the blue-light cystoscopy that can reliably detect CIS when it coexists with papillary tumors. Six percent. For two years, insurers across the country have denied thousands of patients coverage based on a diagnostic distinction that 94% of the physicians in the relevant specialty do not have the equipment to make. I was told I had papillary disease "without CIS." The honest clinical statement, according to the FDA's own panelists, is that I had papillary disease without anyone having looked properly for CIS. These are not the same thing. One is a diagnosis. The other is an artifact of underfunded urology practices and a reimbursement system that doesn't pay for the better scope.
Third — and this is the one that should end the debate — the FDA asked its panelists what they actually do when they identify a patient with papillary disease alone. The answer, delivered without hedging, was: we prescribe off-label the therapies the FDA has already approved for CIS and papillary disease. Because the FDA has never approved anything for papillary alone. Several panelists stated that once they find high-grade papillary, they do not even bother to look for CIS, because its presence or absence does not change their treatment decision. The real-world standard of care has already outrun the regulatory framework by two years and counting. The FDA is not being asked to approve something novel. It is being asked to ratify what is already happening at the bedside, in practices across the country, every day ��� off-label, without reimbursement certainty, and over the objections of insurance companies quoting a billing code distinction that the physicians treating the disease have already abandoned.
The day after that workshop, ImmunityBio announced that the FDA had accepted its supplemental biologics license application for review. The agency assigned a decision deadline — known in regulatory jargon as a PDUFA date — of January 6, 2027. In plain English: the FDA has given itself roughly seven more months. During those seven months, approximately 80,000 more Americans will be diagnosed with papillary NMIBC. The NCCN — a panel of some thirty thought leaders from NCI-designated comprehensive cancer centers — already voted in March 2026 to designate Anktiva plus BCG as a Category 2A guideline for papillary disease alone. The clinical data are published in the New England Journal of Medicine and The Journal of Urology. The three-year numbers from the QUILT-3.032 trial show 96% disease-specific survival, greater than 80% bladder preservation, and near-95% progression-free survival at twelve months. The clinical consensus is not emerging. It has emerged. What remains is paperwork.
Journalist Mindy Kitei (@CFSCentral) made the point with admirable precision: the January 6 deadline is a ceiling, not a floor. The FDA has the discretion to act before it. It has exercised that discretion before when the evidentiary case was overwhelming. I would submit — as a patient, as an advocate, and as an attorney who has spent a career reading evidentiary records — that the evidentiary case here is as overwhelming as it gets. The agency's own witnesses said so, on the record, the day before it accepted the application.
I owe a debt of gratitude to Dr. Patrick Soon-Shiong (@DrPatrick) and to ImmunityBio for this drug and for the relentless persistence required to drag it through a regulatory apparatus that does not make persistence easy. ImmunityBio received a Refusal to File letter in May 2025. A lesser company — or a more rationally self-interested one — might have walked away, run a five-year randomized trial the FDA seemed to want, and let the patients absorb the delay. ImmunityBio did not walk away. It submitted additional data. It engaged the agency. It showed up at the workshop. Dr. Soon-Shiong, who attended the May 18 session, has been vocal, public, and unrelenting in pressing the case that bladder cancer patients deserve access to this drug now, not on a bureaucratic timetable calibrated to a distinction his science has rendered meaningless. These are not rent-seekers. These are the people who took the risk — scientific, financial, and reputational — that the system is supposed to reward and mostly doesn't.
I wrote in March about the intermediaries who profit from the complexity of this system— the insurers who have industrialized denial, the hospital billing architectures that relocate patients between floors to satisfy a ledger, the regulatory apparatus that cannot always distinguish between protecting patients and protecting the administrative status quo. I called them rent-seekers, and I used that term with its full Ricardian weight. I do not need to reprise the argument here. The May 18 workshop made it for me. When the FDA's own panelists confirm that 94% of urologists cannot make the diagnostic distinction on which the entire reimbursement architecture rests, the toll booth is visible to everyone.
Let me be plain about what those two months of insurance warfare felt like, because the policy language can sanitize it. It was despair. Not the poetic kind. The clinical kind — the kind where you lie awake calculating whether your bladder will be removed because a claims adjuster in a cubicle has overruled a board-certified urologist on the question of medical necessity. I am an attorney. I have twenty-two years of litigation instincts and a dispositional inability to accept no for an answer. I won. But "winning" should not require a law degree, a combative temperament, a patient girlfriend, and enough disposable rage to treat an insurance appeals process as a second practice. Most patients do not have those resources. Most patients comply with the denial letter. I think about them constantly.
The FDA convened the witnesses. The witnesses testified. The clinical evidence is published. The expert consensus is recorded. The application is accepted. 80,000 patients a year are waiting.
The evidence is in. Act.
David L. McKenzie is an attorney in Raleigh, North Carolina, specializing in intellectual property and First Amendment law. He is a bladder cancer patient advocate.
@BladderCancerUS @mckenzielaw @ChrisCuomo @katiecouric @RandPaul @OncoDailyGU
Congratulations to @DrPatrick, the entire @ImmunityBio team, patients, advocates, and long-term $IBRX investors.
After months of short-driven fear around a potential RTF, FDA has officially ACCEPTED the ANKTIVA + BCG label expansion sBLA and assigned a Jan. 6, 2027 PDUFA date.
A major regulatory milestone and an important step toward expanding treatment options for patients with papillary NMIBC. Now the focus shifts to approval.
Onward and upward.
https://t.co/g05V4Zg2D8
🚨 HE JOKED ON TIKTOK ABOUT BUYING SPIRIT AIRLINES… HOURS LATER $132,000,000 FLOODED IN — NOW HE COULD BE CEO
Spirit Airlines didn’t just struggle… it collapsed.
One of America’s biggest low-cost carriers wiped out.
That’s when this guy stepped in.
The same guy who went viral for flying Spirit Airlines for 24 hours straight on YouTube.
He posted a simple idea on social media:
“What if we all just… buy it?”
His logic?
There are 250M+ adults in the U.S.
If even a fraction chipped in the cost of a Spirit ticket ($30–$40)… you could raise billions.
Then it exploded.
• Millions of views within hours
• Website launched in under an hour
• Traffic crashes it instantly
• Media starts calling (WSJ, CBS, Fox)
• Developers, lawyers, PR scrambling to join
A few hours later?
$132,000,000 in pledges.
(No money collected, just people saying they’re in)
Now he’s pitching something even bigger:
• One person = one vote (not based on money)
• No private equity control
• Airline “owned by the people”
• Him… stepping in as CEO
He admits he’s figuring it out in real time.
It started as a joke but turned into a movement overnight.
People aren’t laughing anymore… they’re signing up.
Would you trust a random guy from TikTok to run this airline… or stick with the people who ran it into the ground?
📹: TikTok/hbpvo
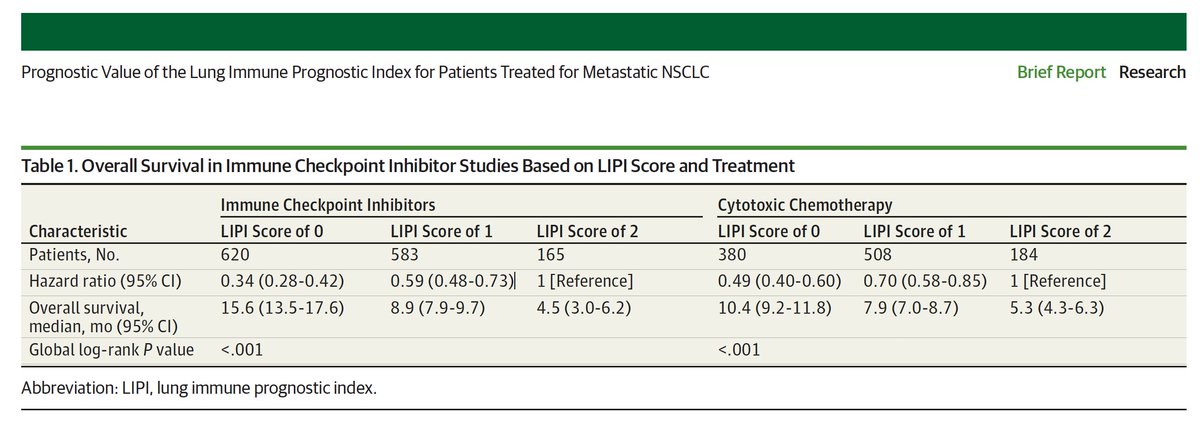
As far back as 2019, Richard Pazdur, then head of OCE at FDA, recognized the importance of lymphocyte count in progression free survival and overall survival in lung cancer. I just discovered this paper today, just as I recently discovered the 2007 NCI workshop report showing the importance of T cell growth factor.
He concludes that "baseline LDH level and dNLR are important prognostic biomarkers irrespective of treatment modality for patients with mNSCLC" meaning that whether the patient receives radiation, chemo, or checkpoint inhibitors, the level of lymphocyte count (ALC) is the critical biomarker for outcomes regardless of treatment modality.
The Saudi FDA recognized this immediately and on that basis approved Anktiva for the treatment of 2nd line lung cancer who relapsed following standard of care.
Pazdur further states "As further prospective clinical trial information is collected, the role of the LIPI score can be better defined." Stay tuned.
#4 Triple Negative Breast Cancer, Metastatic Disease
Coming soon at ESMO, a study by Dr. Aditya Bardia at UCLA and Dr. Hope Rugo at City of Hope - two world class opinion leaders in breast cancer who present results in May 2026 in Berlin at ESMO-Breast, entitled "Pre-treatment neutrophil-to-lymphocyte ratio and impact on immunotherapy efficacy in patients with metastatic triple-negative breast cancer (mTNBC)".
Data is embargoed until then. Stay tuned, ALC matters. High NLR ratio means a high neutrophil with a low lymphocyte count - a bad sign for outcome. Stay tuned.
$IBRX An early-stage breast cancer patient. She gets chemotherapy and pembrolizumab. She achieves pathologic complete response. Her scan is clean. Her oncologist tells her that her cancer is gone.
Then she gets COVID.
Her oncologist is watching her tumor markers, her imaging, her symptoms. Her oncologist is not watching her absolute lymphocyte count.
Eighteen months later, the cancer comes back in her bones.
That population is real. 28,742 patients. UCLA and Mount Sinai. AACR late-breaker, April 21.
They diagrammed what drives breast cancer recurrence: NK cell depletion, T cell exhaustion, lymphocytes lost.
One FDA-approved drug hits every target on the diagram.
Its name isn't in the paper.
THE SENTENCE
The abstract ends with one line, dropped cleanly, without drama:
"Lymphopenia is a potentially modifiable risk factor that warrants prospective study as a therapeutic target."
That is a clinical trial protocol written by an 8-author academic team, published in a peer-reviewed AACR late-breaker, calling for a trial of lymphopenia-correcting therapy in breast cancer patients.
They did not name which drug.
There is one.
WHO WROTE IT
Authors on the poster: Lisa Shiliang Zhang, Eric Yang, Alexis LeVee, Sonia Hui, Gavin Hui, Marla Lipsyc-Sharf, Carlos Cordon-Cardo, and Aditya Bardia.
Lead author: Zhang, UCLA. Senior author: Bardia, UCLA (a renowned breast cancer oncologist). Mount Sinai co-author: Cordon-Cardo, Chairman of Pathology at Icahn School of Medicine.
AACR Annual Meeting 2026. Abstract 5418. Cancer Research 2026;86(7 Suppl). (AACR Journals)
WHAT THEY STUDIED
A multi-institutional retrospective cohort of breast cancer patients from two academic medical centers.
Initial cohort: 36,496. After exclusions: 28,742 in the analysis cohort. Stratified by COVID-19 exposure, by lymphopenia status, and by stage. All patients Stage 1 through Stage 3 (curative-intent early breast cancer, not metastatic).
Outcomes measured: local recurrence, distant recurrence, and event-free survival.
Overlaid onto the clinical data: bulk RNA sequencing from rapid-autopsy studies, used to anchor the mechanism.
This is ~80 times larger than the SABCS triple-negative paper PSS surfaced April 20. Same research team, vastly bigger cohort, and now covering every histologic subtype of early-stage breast cancer rather than TNBC alone.
THE FINDING THAT MATTERS
Read these carefully.
Among all COVID-positive breast cancer patients in the cohort:
- Local recurrence: HR 2.47 (p<0.001)
- Distant recurrence: HR 1.50 (p<0.001)
Now split the distant-recurrence average by lymphocyte status:
- COVID with subsequent lymphopenia: HR 2.46 (p=0.009)
- COVID without lymphopenia: HR 1.11 (not significant, p=0.68)
The distant recurrence risk from COVID is not distributed evenly across all COVID-positive patients. It is concentrated entirely in the subgroup whose lymphocyte counts dropped afterward. The subgroup whose lymphocyte counts held firm did not suffer a meaningful increase in distant recurrence.
Fix the lymphopenia, fix the risk.
In epidemiology, that is a mediation finding. The causal variable has been isolated. And unlike most mediation papers, this one names a variable that is measurable (free, on every CBC), modifiable (lymphocytes can be restored), and already addressable by an existing drug.
THE DIAGRAM
The paper's Figure 4 walks through the proposed mechanism, arrow by arrow:
Local breast disease → COVID-19 infection → four parallel downstream effects:
1. Cytokine storm and inflammation (elevated IL-6, IL-1β, TNFα, IFNγ, IL-10)
2. Lymphopenia and apoptosis (depletion of B cells, CD4+ T cells, CD8+ T cells, and natural killer cells)
3. p53 dysregulation in cancer cells
4. T cell and NK cell exhaustion (elevated PD-1, NKG2A, TIM-3)
All four pathways converge on one endpoint: decreased immune surveillance. And from there, distant recurrence.
This is the cleanest unified framework the breast cancer field has for how post-treatment recurrence works immunologically, rather than just through cancer biology alone.
THE MIRROR IMAGE
Now read ImmunityBio's mechanism language, from the April 21 Saudi launch press release:
"At the core of our strategy is the Cancer BioShield platform, which is designed to stimulate critical lymphocytes, including natural killer (NK) cells, cytotoxic T cells, and memory T cells via our proprietary IL-15 superagonist."
And the Saudi NSCLC accelerated-approval label, quoted verbatim: "Approved under accelerated approval based on the increase of ALC associated with overall survival in single arm study."
Place the two pictures side by side.
Bardia's diagram lists: low NK cells, exhausted T cells, low CD8+ and CD4+ T cells, elevated PD-1 and NKG2A and TIM-3.
ANKTIVA's FDA-labeled mechanism raises NK cells, CD8+ cytotoxic T cells, and memory T cells via IL-15 receptor agonism. Published clinical data across ImmunityBio's program have shown corresponding restoration of absolute lymphocyte counts.
Mirror image.
Bardia's team drew the problem. The FDA label already describes the tool.
The academic team was not required to name a drug class. By calling for a trial of lymphopenia-correcting therapy, they named one anyway.
THE DRUMBEAT
@DrPatrick numbered his posts on this.
#1 (April 20): The UCLA / City of Hope SABCS 2025 paper on early TNBC. N=372. pCR 45.9% vs 63.0% in lymphopenic vs normal arms. (AACR PS4-10-26)
#2 (April 21): The 28,742-patient cohort study above. All early-stage breast cancer. Post-COVID framing. Mediation analysis. Mechanism diagram. (AACR 5418)
#3 (April 22): Same 372 TNBC cohort tracked through treatment. Lymphopenia rises from 9.9% at baseline to 38.7% pre-surgery. In the subgroup whose lymphocytes crash during chemo: 14.9% complete response vs 82% for those who hold firm. p=0.034. (AACR Abstract C040)
Three beats, three days, same senior author, same UCLA / Mount Sinai research program. PSS is explicitly numbering them in sequence. The program is still active.
WHAT THIS IS ABOUT
Remember the woman from the opening. Complete response. Clean scan. Then COVID. Then eighteen months later, the cancer in her bones.
She is one of a population. Approximately 310,000 early breast cancer diagnoses per year in the United States. About 2.3 million worldwide, the vast majority early-stage and curative-intent. A substantial subset experience treatment-related lymphopenia, post-COVID lymphopenia, or both. Some meaningful fraction of their recurrences, this paper argues, is driven by a lab value nobody was watching and that can be raised by a drug already FDA-approved for a different indication.
One drug. Already on the shelf. Already reimbursed by Medicare under its own J-code. Already shipping on three continents. Already funded by a sovereign factory in Riyadh.
Just not approved for her. Not in the country where it was invented and is manufactured.
WHAT SHOULD HAVE BEEN A PRESS RELEASE FIVE TIMES OVER
ImmunityBio's Saudi commercial launch landed April 21. The Saudi label is the first in any jurisdiction to cite "increase of ALC associated with overall survival" as the accelerated approval basis for non-small cell lung cancer.
Saudi regulators just accepted ALC as a surrogate endpoint for survival.
Bardia's team just made ALC a predictor of breast cancer recurrence.
The same biomarker. The same drug class. Two countries, two tumor types, on the public record within the same day.
Also on April 21, RFK Jr., the US Health Secretary, said on camera: "China is now eating our lunch... They went from running 3% of clinical trials to running 30%... we are fast-tracking approvals now in our country at record levels."
PSS reposted that clip to his feed.
Five signals. One week. The frame is no longer emerging. The frame is here.
THE CLOSE
Her scans came back clean.
Then she caught COVID.
Her lymphocyte count quietly dropped.
Nobody was watching it.
Eighteen months later, the cancer was in her bones.
The drug that could have held the line was already FDA-approved when she started treatment.
Just not for her.