English trainer. Face-to-face in Vienna. Online worldwide.
Discuss long Covid & health.
Dozens of tv paper formats looking for takers.
Creative ideas galore.
The long-term cardiovascular risks of SARSCoV2 infection and reinfections
Your heart is under silent, cumulative attack from SARSCoV2, and every reinfection can reload/worsen the damage.
Here a personal recap of 10 important studies from the last 2 years showing exactly how this virus and its reinfections can/may shape (and shorten) your cardiovascular future.
Evidence is clear, long-term, and growing.
Print and show your Cardiologist.
Let’s connect the dots…
1. Immunothrombosis multi-omics study:
3 months after hospitalisation, long COVID patients still have blood biologically “clot-ready” with persistent endothelial activation and prothrombotic signalling.
https://t.co/9yj7zVbgxO
2. IL-6 & SAA 6-year study:
Higher acute-phase IL-6 and SAA levels independently predict cardiovascular events and death up to 6 years later, the initial inflammatory storm leaves a lasting CV mark.
https://t.co/Vk7FvK9fQc
3. MIS-C long-term outcomes:
Up to 4.5 years later, MIS-C raises cardiovascular disease risk 14× and hypertension 9× in children, with risks still accumulating.
https://t.co/itRENsOlOS
4. Viruses & cardiac disease review:
SARS-CoV-2 stands out for direct cardiomyocyte invasion + explosive damage + relentless accumulation of risk with every reinfection.
https://t.co/fOX07JNW2o
5. Mayo PET long COVID study:
Persistent cerebral hypometabolism in fatigue/PEM patients still detectable up to 2 years post-infection.
https://t.co/puvllNfghC
6. Reinfection CV outcomes summary:
Reinfections worsen cumulative heart damage, arrhythmias, thrombosis, stroke risk and long COVID cardiovascular symptoms.
https://t.co/B3q7DzyxCZ
7. Youth reinfection & long COVID study:
Reinfection roughly doubles PASC risk, with myocarditis up to 3.6× higher, heart disease ~2× higher and increased thromboembolism.
https://t.co/aqN3VV0kMX
8. Mild infection + reinfection risk:
Even mild cases trigger lasting endothelial damage and prothrombotic state (1.5–2× long-term CV risk), each reinfection compounds the burden.
https://t.co/SvPzOBSOx1
9 Mitochondrial dysfunction in long COVID:
Persistent mitochondrial dysfunction and suppressed oxidative phosphorylation remain in long COVID, pointing to durable multi-organ impact.
https://t.co/98MbV19R9r
10. Cumulative reinfection impact on future CV health:
Reinfection stacks additional damage on prior endothelial injury and inflammation, increasing lifetime risk of heart failure, arrhythmias, thrombosis and accelerated cardiovascular disease.
https://t.co/aqN3VV0kMX
11. Extra, my earlier general reminder post on this exact theme: https://t.co/o3QT12nIG4
‼️Overall convergence across the studies:
Immunothrombosis, acute inflammation markers, direct invasion, endothelial damage, and mitochondrial issues create lasting CV vulnerability that reinfections can keep reloading. #L0ngC0vid
The pattern is very clear.
Fewer infections = lower lifetime cardiovascular risk.
You only have one heart.
Protect it!
#AvoidSars2 #AvoidReinfections #CleanAir #VaccineUpdated
Picture reaching for something on a high shelf and coming up short. You don’t give up; instead, you find a stool, carry it over, and climb up. Buried in that action is something remarkable: You held the goal in your mind, identified what you needed, and executed a plan. No training required.
A study suggests bumble bees can do the same—the first demonstration of this kind of goal-directed problem-solving in an insect.
Learn more: https://t.co/srV4TqUTsp
I'm a cardiologist. A 42-year-old mother of two came to my office complaining of jaw pain and crushing fatigue. She ran half-marathons. Her EKG was normal. Another doctor had sent her home with anxiety medication.
When I got her into the cath lab, I found severe microvascular disease — plaque choking the tiniest vessels of her heart, the ones standard angiograms routinely miss.
Her heart had been starving in silence while everyone told her she was stressed.
She is alive today. Too many women like her are not.
Heart disease kills more women than every cancer combined. And medicine is still diagnosing it through a male lens.
84% of cardiologists report having patients in the past year whose heart disease was misdiagnosed by another physician. Women with a STEMI heart attack have a 59% greater chance of being misdiagnosed compared to men. Women with an NSTEMI — 41% greater chance.
The reason is structural. For decades, we screened, tested, and treated women using a template built for men.
Men's heart attacks announce themselves — the crushing chest pain, the clutched fist, the Hollywood collapse. Women's hearts whisper. Crushing fatigue that feels like wearing a lead vest. Jaw pain written off as TMJ. Nausea blamed on a stomach bug. An ache between the shoulder blades blamed on a long week. Shortness of breath blamed on being out of shape.
For years, medicine called these "atypical" symptoms. They are not atypical. They are female-typical. Half of humanity is not a variant.
And the biology runs deeper than symptoms.
Women have smaller hearts and narrower coronary arteries. Plaque doesn't only clog the big highway vessels — it hides in the microvasculature, the tiny branches feeding the heart muscle itself. A woman can have a heart attack with a completely "clean" standard angiogram.
SCAD — spontaneous coronary artery dissection — occurs 90% of the time in women. Often young, fit women with zero traditional risk factors. It's the leading cause of heart attack in women under 50, accounting for roughly one quarter of all cases in that age group. Most doctors have never diagnosed one.
And some of the most dangerous cardiac risk factors are hidden in women's medical histories where no one thinks to look:
Preeclampsia or gestational hypertension doubles to quadruples lifetime heart disease and stroke risk. Pregnancy is the body's first cardiac stress test — and these complications are early warning sirens, not closed chapters.
Autoimmune disease — lupus, rheumatoid arthritis, psoriasis — far more common in women, turbocharges inflammation and plaque formation at any age.
Cardiovascular disease in women aged 20-44 is projected to surge nearly 50% by 2050.
The youngest patients in my practice keep getting younger.
What every woman should ask her doctor — and what every doctor should be asking:
"Given my pregnancy history, autoimmune status, and family history — what is my full cardiovascular risk?" If they don't ask about preeclampsia or gestational diabetes, volunteer it.
"Should I have an Lp(a) test and a coronary calcium score?" Standard cholesterol panels miss too much. Lp(a) is genetic, one-time, and most women have never been tested.
"My tests came back normal but my symptoms haven't stopped — what's next?" Normal stress tests and angiograms can miss microvascular disease, spasm, and SCAD. Persistent symptoms warrant coronary CT angiography or cardiac MRI.
And if something feels wrong — say these exact words to your doctor: "I am concerned this could be my heart."
That single sentence changes the workup. Do not soften it. Do not apologize for it.
80% of heart disease is preventable. But the playbook has to be built for female biology.
Two decades ago, I wrote one of the first books warning that heart disease was the number one killer of women and that medicine was diagnosing it through a male lens. It was recognized by First Lady Laura Bush at the White House during the early years of the national conversation about women's heart health.
I'm haunted by how much of that book I could republish today unchanged.
The science has advanced. The awareness has grown. But the gap between what we know and what happens in the exam room is still costing women their lives.
Share this with every woman you love — and every doctor who treats them. READ MORE: https://t.co/4LRugiY8q2
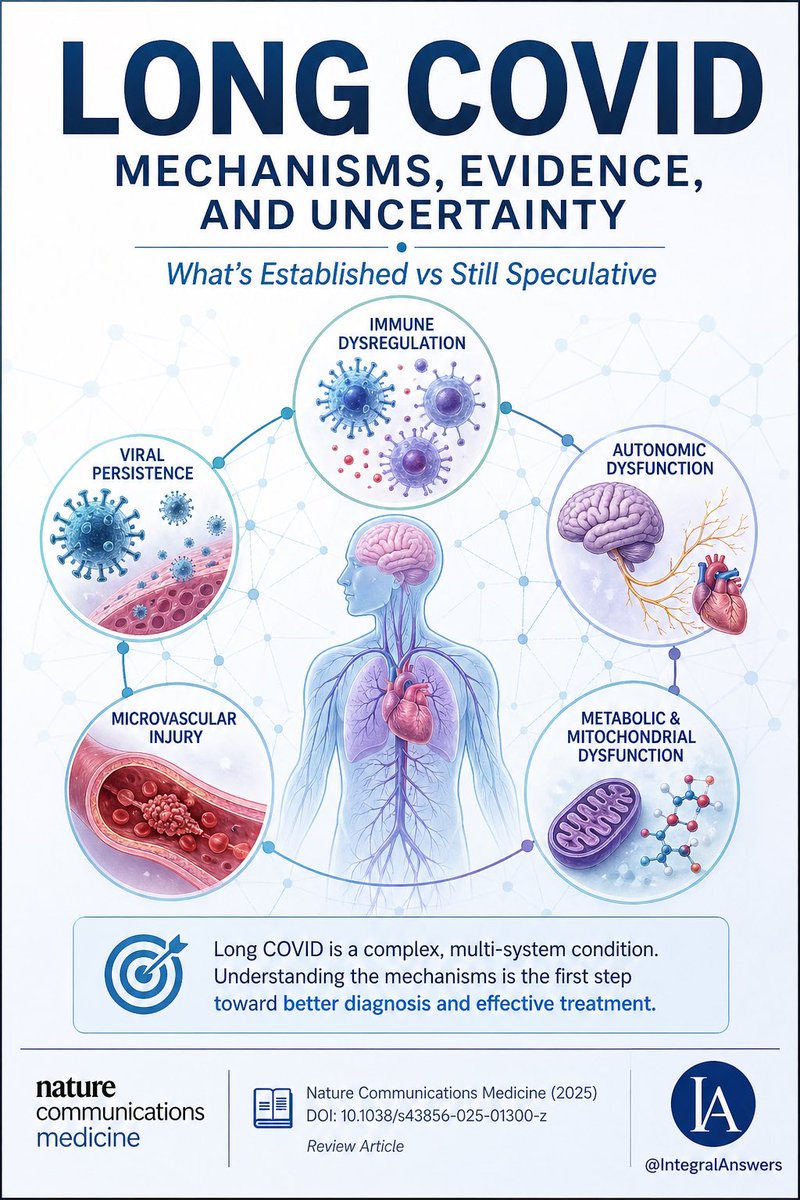
1/ Long COVID is one of the most complex post-infectious syndromes ever studied.
A new review in Nature Communications Medicine attempts to unify the biology.
Here’s what’s established, what’s emerging, and what’s still speculative. 🧵
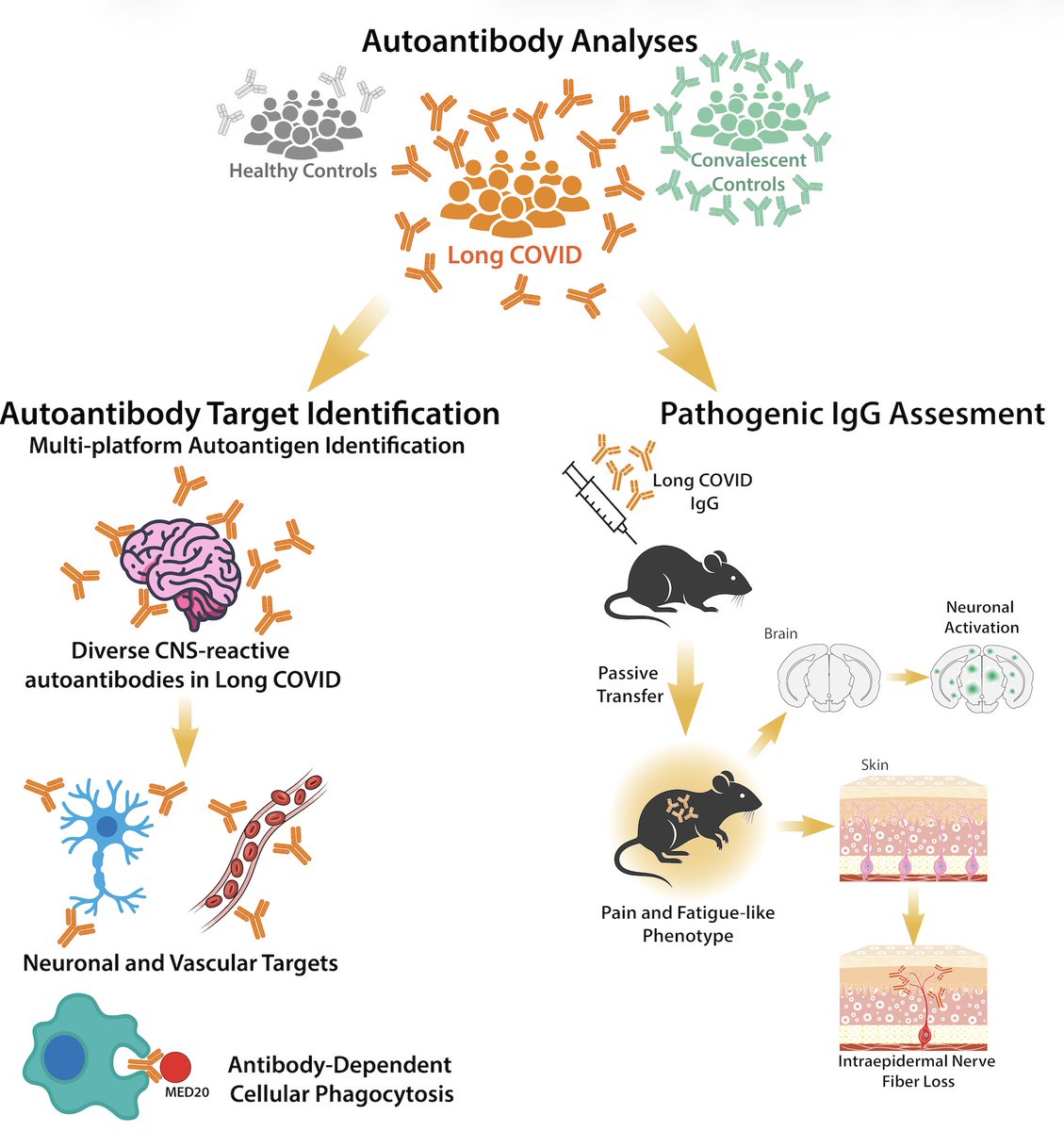
Excited to share our study by @keylas3 et al. on pathological autoantibodies in people with Long COVID. We asked whether IgG in patients with Long COVID bind to human tissues/antigens and cause pathologies when transferred into mice. With @PutrinoLab
https://t.co/tcowCufWyf
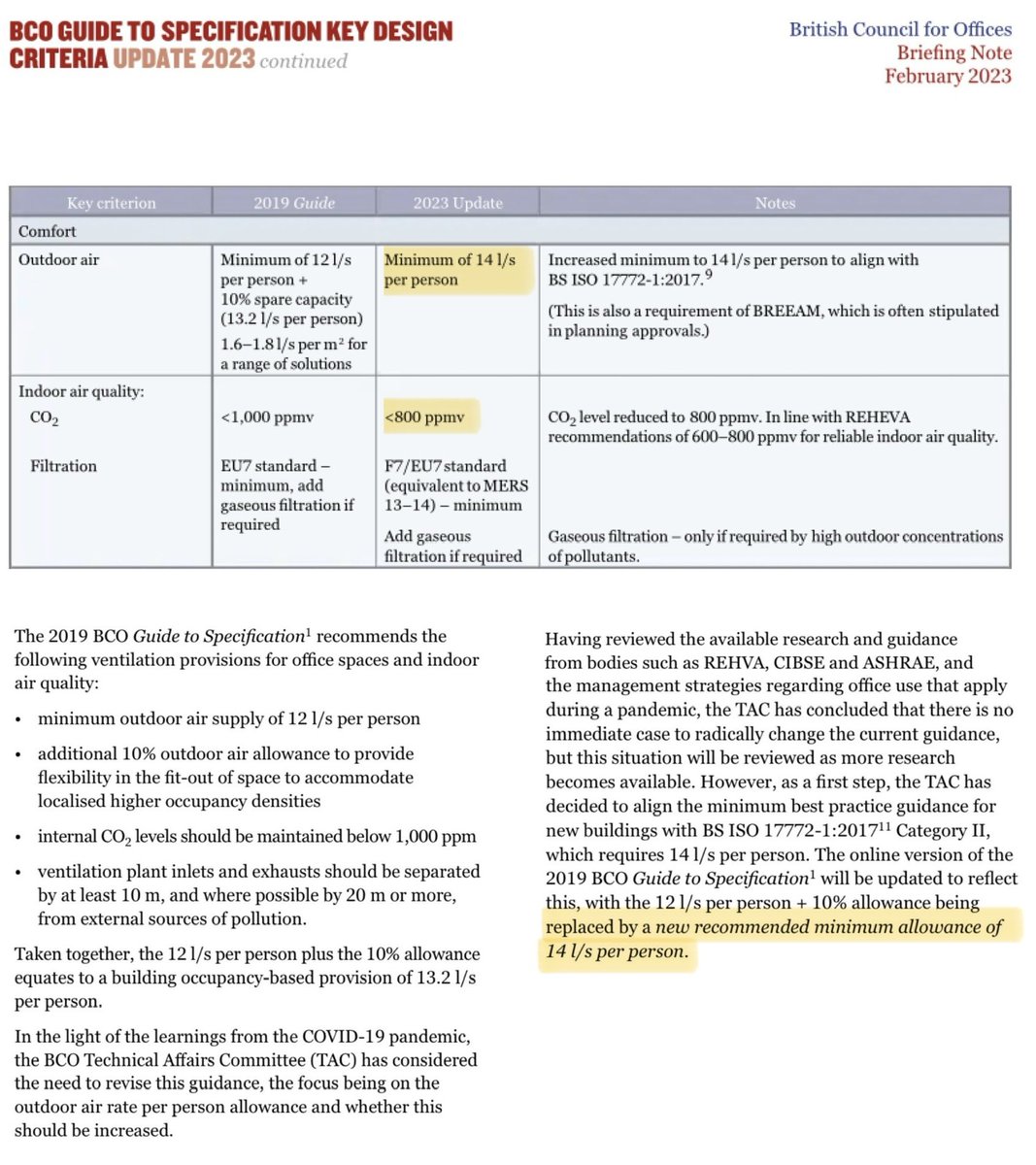
In 2023, the British Council for Offices (BCO) updated the ventilation guidance for offices:
💨 The *minimum* recommended ventilation rate was increased from 12 to 14 litres of outdoor air per sec per person.
Now guess what the ventilation rate is in a typical UK classroom…❓
A friend passed this to me, saying it might be helpful - it's about getting help on Long Covid from your GP, it's for a UK setting, but some of it will be applicable anywhere - read the note at the end for more too.
"I work in AI. I used it to research and write my mum a letter about her Long COVID. Her GP called her the next day after 3 years of being dismissed!
*Reposting here as myself since it blew up in another support group and people really want help with this… feel free to add/DM me.*
So I work in AI, specifically in healthcare tech. So when my mum had been fobbed off by her GP for the third year in a row about her Long COVID, I figured I should actually do something useful with what I know.
This isn't about gaming the system or bending rules. Everything I'm sharing here is publicly available on NHS and government websites. I just used AI to find it, understand it, and turn it into something a GP couldn't easily brush off.
Here's what most people don't know. The NHS publishes detailed guidelines that GPs are expected to follow. NICE published a specific Long COVID guideline called NG188 that sets out exactly what a GP has to do when a patient comes to them with ongoing post-Covid symptoms. Most patients have never heard of it. Most GPs don't follow it unless someone pushes them on it.
The other thing most people don't know: verbal dismissal is easy to ignore. A formal written letter that references specific guidelines creates a paper trail. The GP now has a documented duty of care they're expected to respond to. It genuinely changes everything.
My mum is 61. Not remotely tech savvy. She would never have found any of this herself. I spent about 20 minutes using AI to pull the relevant guidelines, match them to her situation, and draft a letter. She sent it to her GP by email on a Tuesday. Her GP called her on Wednesday afternoon. First time in three years a GP had called her. She now has a referral to a Long Covid clinic and a written management plan, after years of being told it was probably anxiety or just her age.
Posting her letter below with her details redacted. Copy it, adapt it to your situation, send it by email not in person. You need a timestamp. You need a record. That's what actually forces a response.
───
[Her letter, personal details redacted]
████████████████
████████████████
████████, ██████
██ ██████ 2025
Dr ████████████
████████████ Surgery
████████████████
████████, ██████
Re: Formal written request for Long COVID assessment and personalised management plan
Dear Dr ████████,
I am writing to formally request appropriate assessment and management for post-COVID-19 syndrome (Long COVID), and to create a written record of this request for my medical file.
I contracted COVID-19 in ████████ 2022 and have experienced the following ongoing symptoms for over three years:
• Severe fatigue and post-exertional malaise, symptoms worsen significantly following any physical or cognitive exertion
• Cognitive dysfunction, difficulty with memory, concentration, and word retrieval
• Breathlessness disproportionate to exertion
• Heart palpitations and episodes of tachycardia
• Disrupted sleep despite significant fatigue
• Generalised pain and joint discomfort
These symptoms have substantially impaired my ability to work, maintain daily activities, and quality of life.
CLINICAL BASIS FOR THIS REQUEST
NICE guideline NG188, COVID-19 rapid guideline: managing the long-term effects of COVID-19, was developed jointly by NICE, SIGN and the Royal College of General Practitioners. It applies to any patient with new or ongoing symptoms four or more weeks after acute COVID-19.
Under NG188 section 5.2.1, GPs are expected to use a multidisciplinary approach to guide rehabilitation, including physical, psychological and psychiatric aspects of management.
Under NG188 section 5.2.2, GPs must work with the patient to develop a personalised rehabilitation and management plan, which must be recorded in writing. NICE states explicitly that healthcare professionals are expected to take this guideline fully into account. This is not optional guidance.
Under GMC Good Medical Practice (2024), where a GP cannot adequately manage a patient's condition, they are required to refer to a specialist with the relevant expertise.
Under the NHS Constitution, I have the right to be referred to an appropriate specialist where my GP is unable to provide the required clinical management.
I have not received a personalised management plan or specialist referral in three years of presenting with these symptoms.
WHAT I AM FORMALLY REQUESTING
1. A holistic clinical assessment consistent with NICE NG188, including physical, psychological and functional domains
2. A personalised rehabilitation and management plan recorded in writing, as required under NICE NG188 section 5.2.2
3. Referral to the Long COVID clinic or appropriate multidisciplinary rehabilitation service
4. A written response to this letter within 14 days
I would like this letter to be added to my medical record. I am not requesting anything outside published NHS guidelines. I am asking for what those guidelines state I am entitled to receive.
Yours sincerely,
████████████████
Date of birth: ██/██/████
NHS number: ███ ███ ████
Based on: NICE NG188 (January 2024) | GMC Good Medical Practice (2024) | NHS Constitution (2023)
*Verify current guidelines at https://t.co/1G9ny67PrQ before sending.*
───
Same approach works for basically any condition where you're being dismissed. MCAS (I am currently writing myself a letter to escalate my own issues with this), fibromyalgia, EDS, POTS, chronic fatigue. The escalation pathways exist for all of them, most people just don't know how to use them.
If it’s useful I could build a tool that does this automatically for you. You answer a few questions about your condition, it finds the relevant guidelines and drafts the letter for you. If that sounds useful, DM me or comment. Happy to write one manually for anyone in the meantime.
Not medical advice! Keep seeing your GP. Call 111 if anything gets worse."
If covid infections make you *more vulnerable* to almost every other pathogenic infection by multiple mechanisms, then you'd expect increases in almost every other pathogenic infection.
And that's what we see.
Ten completely unsurprising news stories:
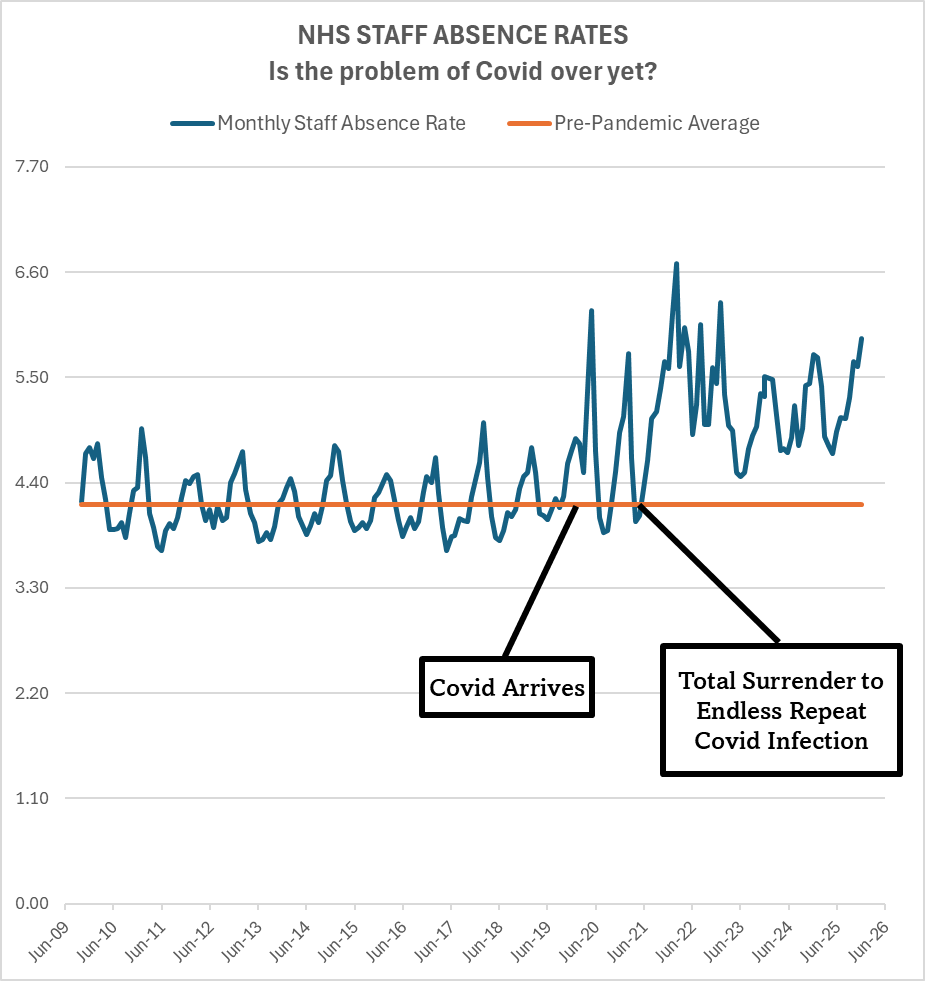
I'm in a lull on twitter without much visibility, so probably hardly anyone will see this, but here's an important thread on "why everyone's sick all the time".
No, you are not imagining it.
Sickness is increasing.
Sickness absence rates are increasing.
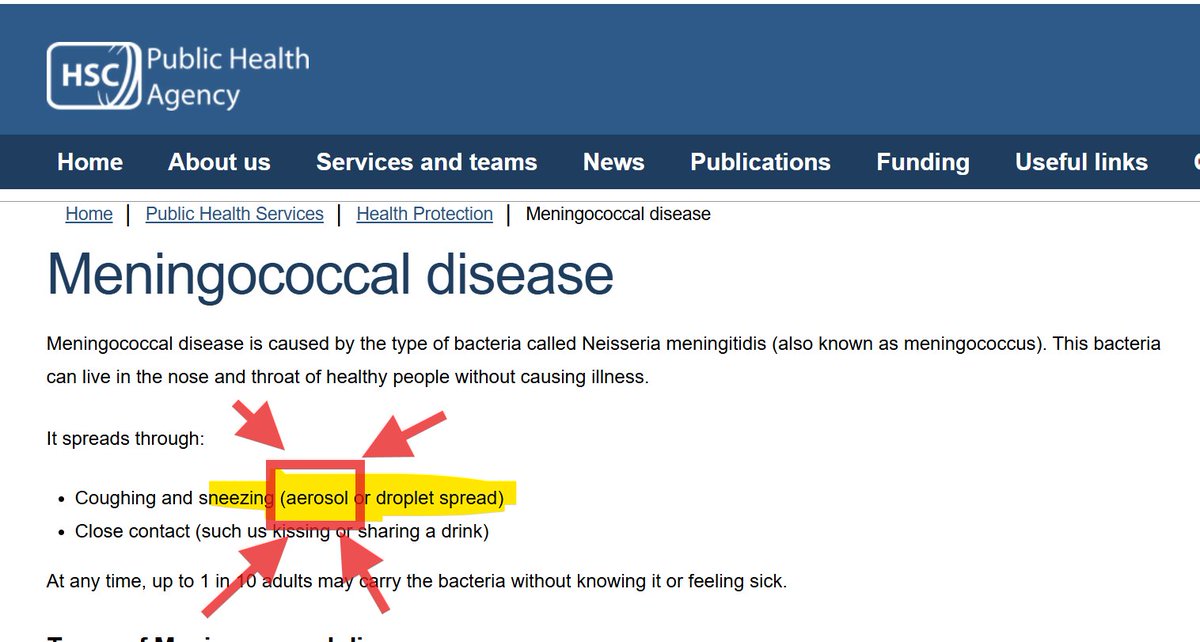
There are a few ways to remove aerosols.
Ventilation & air filtration are good ways.
However, the favoured way by Public Health appears to be just to delete them.
Compare what this page said when crawled in Dec 2025 to what it says today.
7th Dec 2025 pictured.
1/🧵
Them: But if Covid infections lower your lymphocytes wouldn't more people be dying from infections??
Me: Yes, that's right, that's exactly what's happening. 👇
𝗜𝗻𝘁𝗿𝗼𝗱𝘂𝗰𝗶𝗻𝗴 𝗧𝘄𝗶𝗻 — 𝘁𝗵𝗲 𝗔𝗜 𝗰𝗼𝗺𝗽𝗮𝗻𝘆 𝗯𝘂𝗶𝗹𝗱𝗲𝗿.
No setup. Secure. Infinitely scalable.
We just raised a $𝟭𝟬𝗠 𝘀𝗲𝗲𝗱.
After a beta with 𝟭𝟬𝟬,𝟬𝟬𝟬+ 𝗮𝗴𝗲𝗻𝘁𝘀 𝗱𝗲𝗽𝗹𝗼𝘆𝗲𝗱, we’re now opening to everyone.
RT and comment “Twin” — first agents on us. 👇
Him: you need to start living your life
Things he's done in the last month:
Get ill, miss Christmas, recover slowly, get ill.
Things I've done in the last month:
Run up a mountain, swim in the sea, hold someone's hand as they died, hold a 12 hour old baby in my arms, visit five hospitals, six schools, one prison, two nurseries, do a talk for 700 people, sing, research the harm that covid is doing to people who keep catching it.
I think we've let the damage that covid infections do to *linings* slip into the background of all the other problems that covid infections cause.
I think this may be a *big* problem.
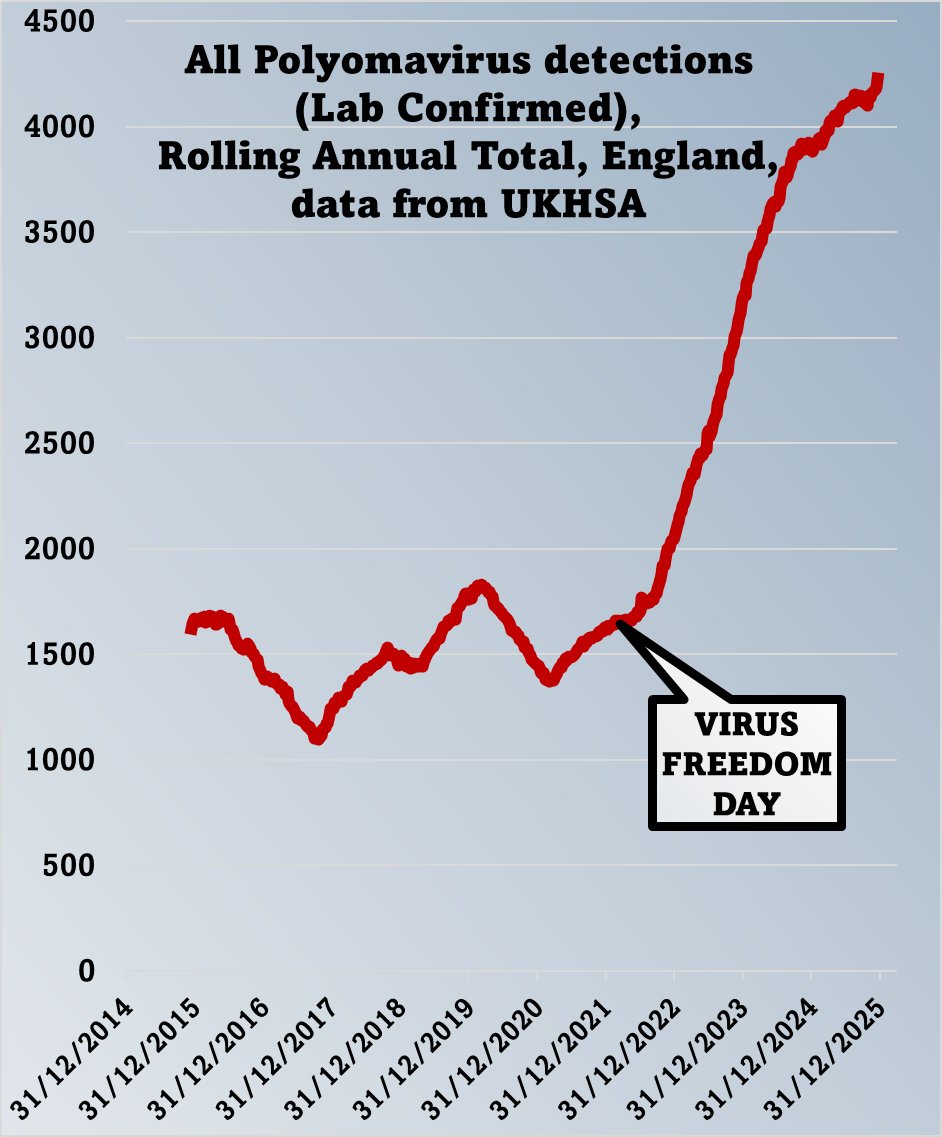
Checking back in on the state of polyomavirus infections.
These are viruses that almost all of us carry for life.
In healthy people they usually sit quietly in the background doing nothing much...
UK DISABILITY STATS
“Disability prevalence among children & working-age adults has risen more sharply since the start of the Covid-19 pandemic”.
Change between 2012/13 & 2023/24:
🚨 16 to 24 yr olds: MORE THAN DOUBLED from 8% to 18%.
🚨25 to 34 yr olds: risen from 11% to 19%.