Among extremely #preterm infants, prophylactic acetaminophen for patent ductus arteriosus accelerated ductal closure but did not increase survival without severe #neonatal morbidity at 36 weeks and was associated with higher rates of cholestasis.
https://t.co/3jH3yup2zn
@EBNEO@oelkhateeb@Dr_KSGautham Gautham, congrats, so honored to have your leadership within this important organization @EBNEO that informs clinicians and improves neonatal outcomes through best use of evidence!
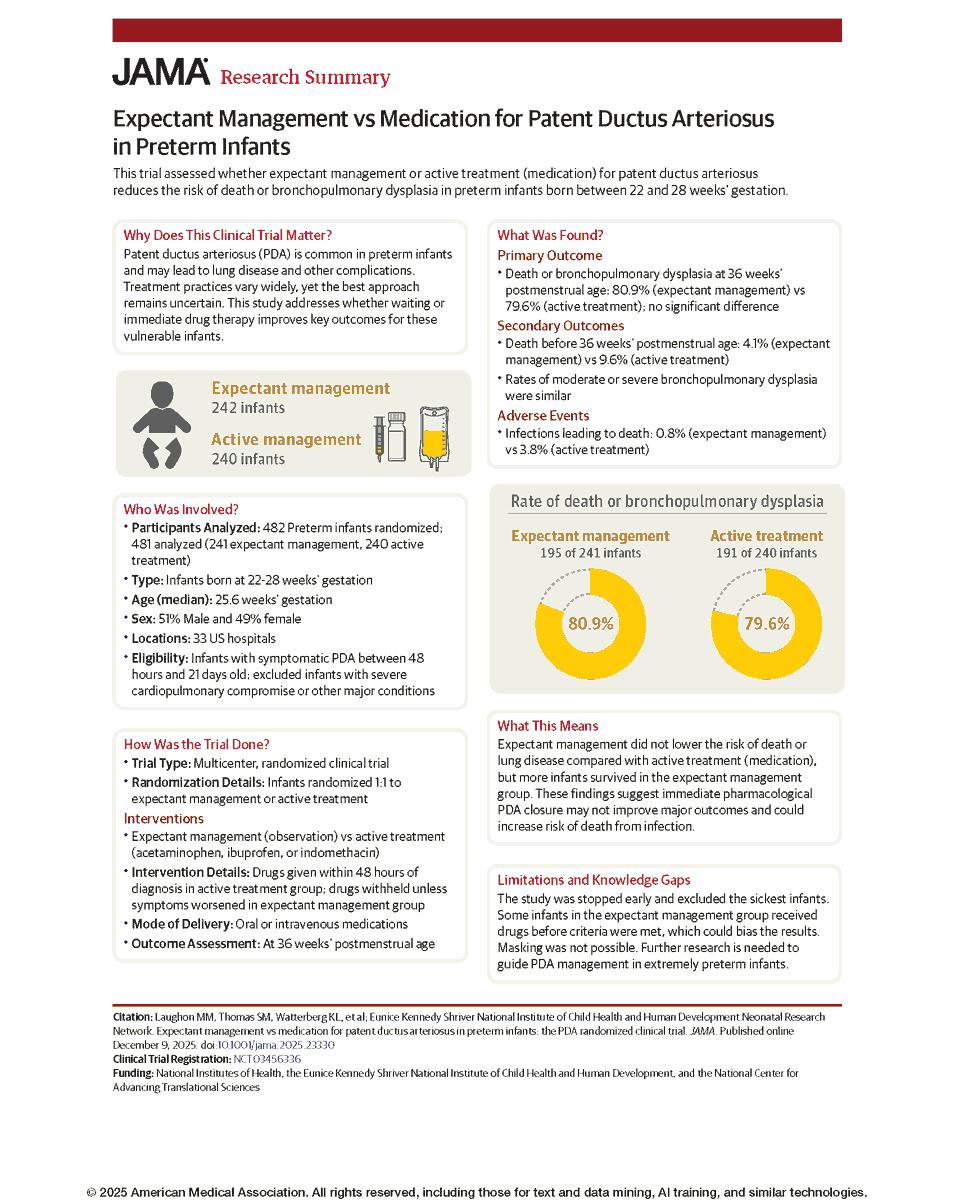
📊 Research Summary: Expectant management among infants with patent ductus arteriosus did not lower the risk of death or BPD compared with active treatment, but more infants survived in the expectant management group.
@Nemours#HotTopicsNeo2025
https://t.co/579xHUMd8u
Among preterm infants born at 22 to 28 weeks’ gestation with a protocol-defined patent ductus arteriosus, does expectant management compared with active treatment decrease the incidence of death or bronchopulmonary dysplasia? #HotTopicsNeo2025
📽️ Watch the video and read the full article: https://t.co/XUQPGromQP
@natetexsun@Dr_KSGautham@X A reminder that we need trials on fluid restriction and increasing PEEP as well. I am skeptical that fluid restriction helps, especially if on full enteral feeds. Clinically it's a reasonable option, but we need data
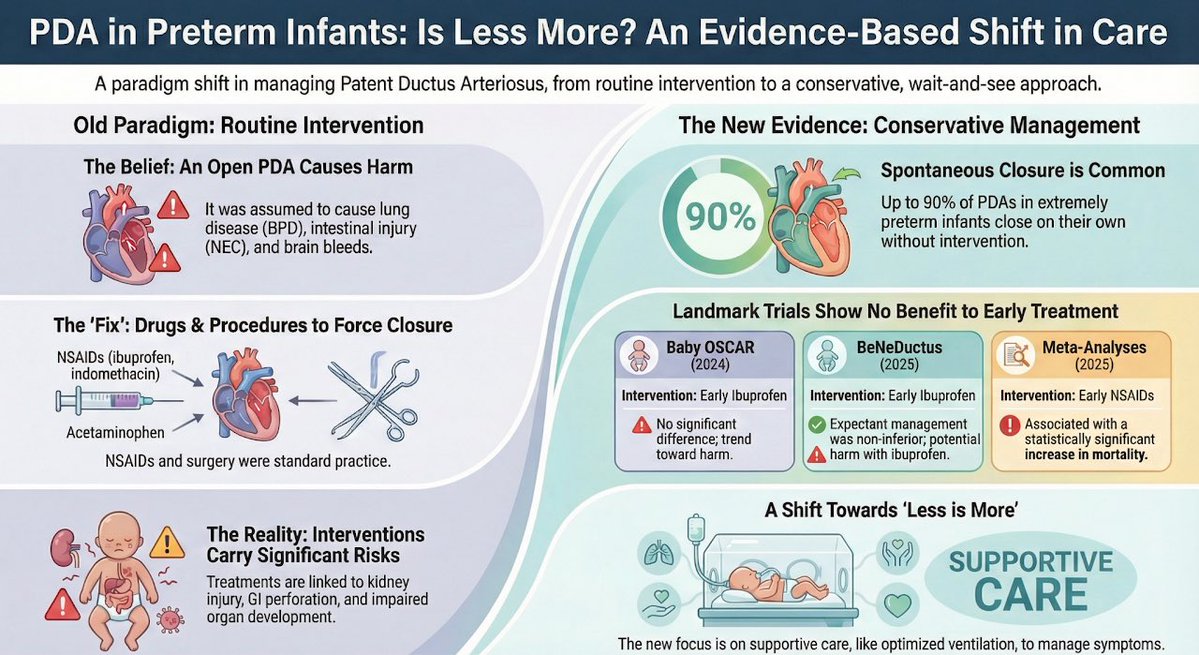
With the publication of the NICHD PDA Trial, we revisit PDA in Prematurity: Rethinking a Decades-Old Debate (2025). In 482 infants (22–28 wks), expectant management showed no difference in death/BPD vs treatment and higher survival.
https://t.co/cpjPnzAlLT
What’s the best way to manage a PDA? New evidence from Laughon et al.
A summary plus appraisal. Let me know if you notice any errors or have other thoughts about this study.
#neotwitter....From the NICHD NRN (congratulations to Matthew Laughon and others): Expectant Management vs Medication for Patent Ductus Arteriosus in Preterm Infants https://t.co/bOXsoAvWsm
@Dr_KSGautham@BrianKingNeo@NICU_Musings@HotTopicsNeo Could potentially randomize to a car seat risk prevention strategy with parental counseling on car seats and what to look for when traveling and baby positioning vs all of that plus a car seat (safe transport for baby plus an extra sat check in car seat that may or not help)
@Dr_KSGautham@BrianKingNeo@NICU_Musings@HotTopicsNeo I think parental consent might be the biggest challenge. There was an RCT for anti-epileptics at discharge post-HIE that had enrollment difficulties because parents didn't want to risk a seizure outcome. It might be hard to convince them if a respiratory event were the outcome
@Dr_KSGautham@BrianKingNeo@NICU_Musings@HotTopicsNeo Ultimately the question of discharge on seizure meds post-HIE was answered by a randomized trial emulation (Glass et al) using observational data https://t.co/xG6qmQLyuh
Looking forward to @HotTopicsNeo !
New study out on car seat testing (CSTS) in neonates. Large sample of 2861 CSTS in #preemies before discharge.
After failing a CSTS mean of 2 days to pass and 77% will pass second test!
What does this test tell us?
@BrianKingNeo#neotwitter
Is Academic Neonatology at the Brink of Extinction? How can Departments of Pediatrics recruit and retain excellent clinicians who inspire students and residents to join Neonatal fellowship? @AAPneonatal@WomenNeo https://t.co/ExUSiyFNPL via @YouTube@nicupodcast
Practical perspective on the risk benefit ratio of probiotics in preterm babies 💡 Incidence of probiotic sepsis and morbidity risk in premature infants: a meta-analysis | Pediatric Research https://t.co/GI6afsrycH
@Dr_KSGautham@mkrettiwt I think we need to find clinical problems (ask those on the front line) that need to be solved and design trials that will immediately inform and change practice whether the trial finding is positive OR negative
Upgrade your #causalinference arsenal.
A revision of our book "Causal Inference: What If" is available at https://t.co/3rrh0l8nFu
Thanks to everyone who suggested improvements, reported typos, and proposed new citations and material.
Enjoy the #WhatIfBook. Also, it's free.
Am not sure about the title of the talk, the objectives and the audience. But IMO the key high-level problems with BPD to be highlighted are
1. We are continuing to use a definition based on the treatment given, not on the disease pathology or pathophysiology.
2. The certainty of evidence for how we assess and manage BPD is low. There have been hardly any RCTs on evolving or established BPD. Yet, in the absence of high certainty evidence groups have formulated recommendations and guidelines based merely on expert opinion and low-level evidence. These guidelines have become established in practice, and have created a lack of equipoise for rigorous studies. Every NICU has its own set of beliefs and traditions on how to manage BPD.
3. We know very little about how to transition babies with BPD to the home (or institutional) setting and how to manage them after the transition. This includes care and support of the parents.
If you look back at all the research and experience in Neonatology over the past 30 years, what is the main message that emerges? IMO it is “Less is More”. We used to think that more intervention is better, and more aggressive, earlier interventions are better. Instead we have learned the opposite is true.
#neotwitter
Updated meta-regression by @ProfLexDoyle et al. examines how potential benefit from Dexamethasone and Hydrocortisone changes with baseline risk of BPD among included trials. #neoEBM#neotwitter#EBNEOalerts@JAMAPediatrics
https://t.co/1mJ6SyweN3