Are medical students asking you how to scroll through MRI images stacks and select sequences? Our module published in Neurology Education may be able to help. Useful for self-study or lecturing after rounds. Free for all to use!
Introducing the first #NeurologyEd Curriculum Resource Report, a foundational MRI brain module featuring dynamic, scrollable MRI image stacks, allowing students to explore images in a way that reflects clinical practice. Download today at: https://t.co/THXV7tQLsg
@JordanHNewman
Tired of always speculating about MR spectroscopy?
If you've ever looked at an MR spectroscopy & thought: "I have no idea what I’m looking at!"--then this cheat sheet is for you!
Here are the 4 basic rules you need so you can understand the spectrum of basic spectroscopy!
First you need to know the peaks.
3 main peaks: Choline, Creatine, NAA
Remember the order bc a spectrum looks like mountain peaks & it is cold in the mountains. And CHOld CREATures NAp or hibernate in the mountains
Choline
Marker of membrane turnover
Remember: membranes coat or “CHOat” the cell
Choline = ChoLEAN, choline LEANS into the creatine peak, it’s right next to it
Creatine
Marker of energy, basically an internal control
Remember, everyone takes Creatine powder for energy!
Creatine is at ~3—creatine almost rhymes with 3
NAA Marker of neuronal health
N = Neuron
NAA has double As so it is at ~2!
Four rules:
1. Hunter’s angle:
—Most people know that the peaks of the spectrum should go up at you move lateral, called Hunter’s angle
—Most bad things reverse Hunter’s angle
—Ask yourself: Is my arrow pointed up to shoot into the air at the enemy (good) or is point to the ground where it will hit the dirt (bad)
2. TE & spectrum length are inversely related
—Spectroscopy follows the rule: speak softly & carry a big stick.
—Short TE = long spectrum, lots of extra peaks for glutamate/glycine, myoinsitol
—Long TE = short spectrum, mainly the basic 3 peaks
3. Each region has its own unique signature
—Each brain region has its own unique composition of compounds that might alter Hunter’s angle a bit, but not reverse it
—Need a control in contralateral normal brain so compare apples to apples
4. Lactate peak goes like a sine wave
—Lactate peak represents anerobic metabolism—sign of cells in trouble
It’s at 1.3ppm. Remember this bc 13 is an unlucky number & lactate is an unlucky sign!
—It’s like a sine wave: up at short TE (35), down at intermediate TE (144), and up again at long TE (244)
—You can use this flipping to better visualize the lactate peak
—You can remember it’s down in the middle TE bc when you’re caught in the middle, you’re down & out
Just remember these tricks & you will be spectacular at basic spectroscopy!
Feeling unarmed when it comes to evaluating cervical radiculopathy & foraminal narrowing on MR?
Think of the nerve root like a hot dog, sitting between the two buns of the disc/uncovertebral joint & facet.
The more you put in your hot dog, the more the hot dog itself is squished. Same w/the nerve root.
Spurring & degenerative change are like the extra topping that push on the hot dog inside the buns.
A small amount of toppings/degenerative change, leaves the hot dog space. But if you pile on fixings, then the hot dog is taken over.
Ask yourself--how is my hot dog doing?
Mild stenosis is like just a little ketchup & mustard on the bun but hot dog still has space.
Moderate stenosis is when you aren’t just putting on sauce, you are adding things that take up space, like relish.
But there’s only so much relish one can put on, so it doesn’t take up more than half the bun.
Severe stenosis is like a chili cheese dog, where the hot dog is smothered & it has no room in the bun away from the chili or cheese. Here the narrowing is greater than 50%
This is the Kim classification & has strong correlation w/symptoms I like it bc it doesn’t require calipers to estimate a >50% narrowing
So now you know how to both image and assess stenosis in the cervical neural foramen.
Now hopefully rating cervical foraminal narrowing won’t be a pain in the neck!
To call it or not to call it? That is the question!
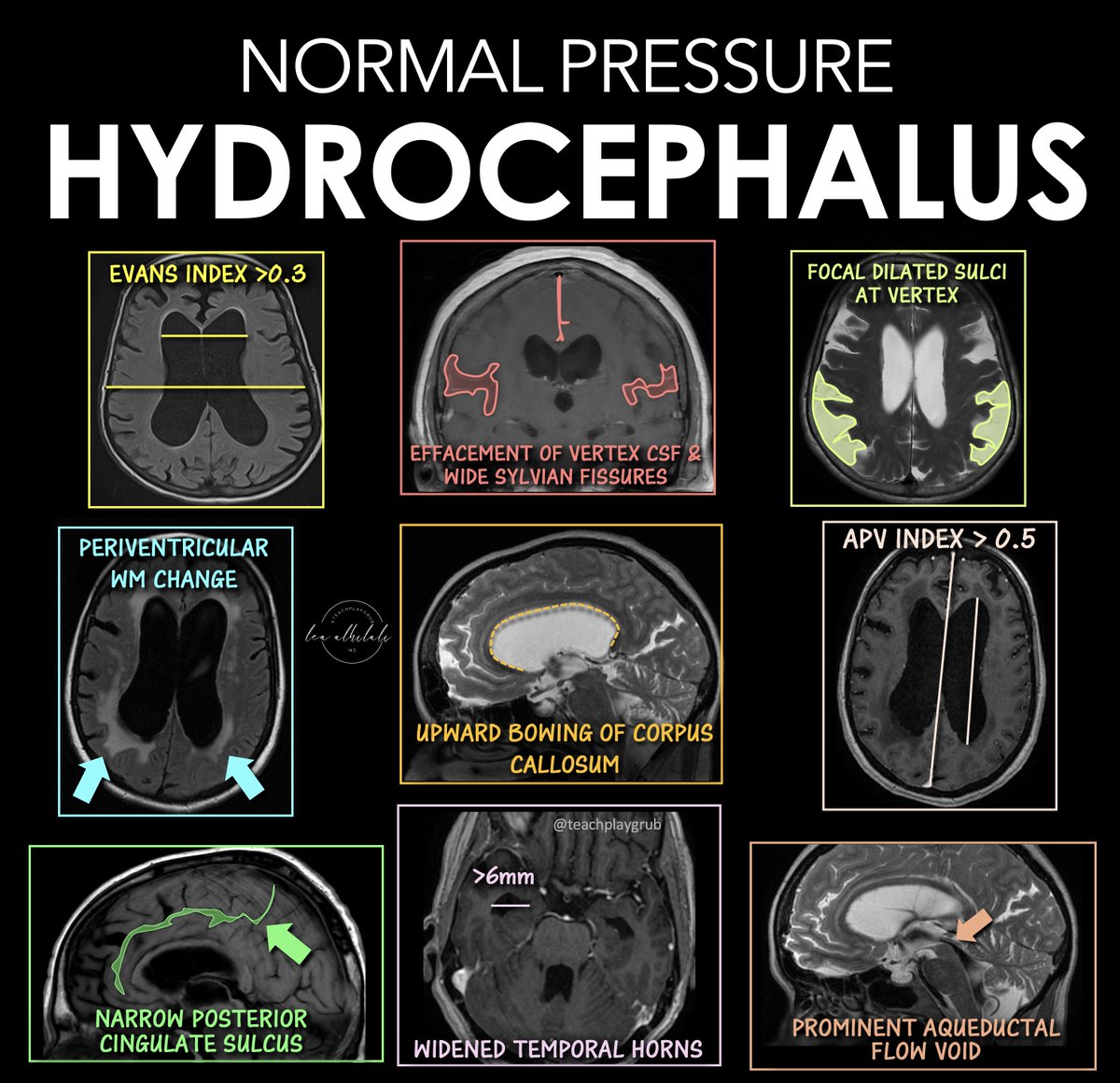
Do you feel a bit wacky & wobbly when it comes to calling normal pressure hydrocephalus on imaging?
You don’t want to overcall it, but you don’t want to miss it either!
Here are the signs of NPH
🔹 Evans Index > 0.3
--Enlarged frontal horns relative to skull width → ventriculomegaly.
Remember it: “One out of three is too big for me!”
🔹 Periventricular White Matter Change
--T2/FLAIR hyperintensity from transependymal CSF flow.
Remember it: “Leaking pressure leaves a glow.”
🔹 Narrowing of the Posterior Cingulate Sulcus
--Tight high-convexity sulci from crowding at the vertex.
Remember it: “The top gets squeezed shut.”
🔹 Effaced Vertex CSF + Wide Sylvian Fissures
--Tight sulci up top but enlarged fissures laterally (DESH pattern).
Remember it: “Dry on top, wet on the sides.”
🔹 Upward Bowing of the Corpus Callosum
--Ventricular expansion pushes the corpus callosum upward.
Remember it: “If the corpus callosum is arched, the patient can’t march (wobbly)”
🔹 Temporal Horns > 6 mm
--Early temporal horn dilation from hydrocephalus.
Remember it: “Big horns before big vents.”
🔹 Focally Dilated Sulci at the Vertex
--Patchy enlarged sulci despite surrounding crowding.
Remember it: “Holes in a leaky roof = too much water on the brain!”
🔹 APV Index > 0.5
--Increased ventricular-to-parenchymal proportion suggesting hydrocephalus.
Remember it: “Glass half full is too much!”
🔹 Prominent Aqueductal Flow Void
--Increased CSF flow through the aqueduct on MRI.
Remember it: “If the aqueductal flow is super black, the ventricles are out of whack.”
Classic NPH imaging theme: enlarged ventricles + tight high convexities + disproportionate CSF redistribution.
Hopefully now you won't wobble on the diagnosis of NPH!!
CTE cannot be diagnosed during life. Our work published today in @NatureMedicine demonstrates that most individuals meeting proposed clinical criteria do not have evidence of #CTE neuropathology at autopsy (1/5)
https://t.co/5euKrqf8vq
@PennNSG@PennMedCSO@WillStewNeuro
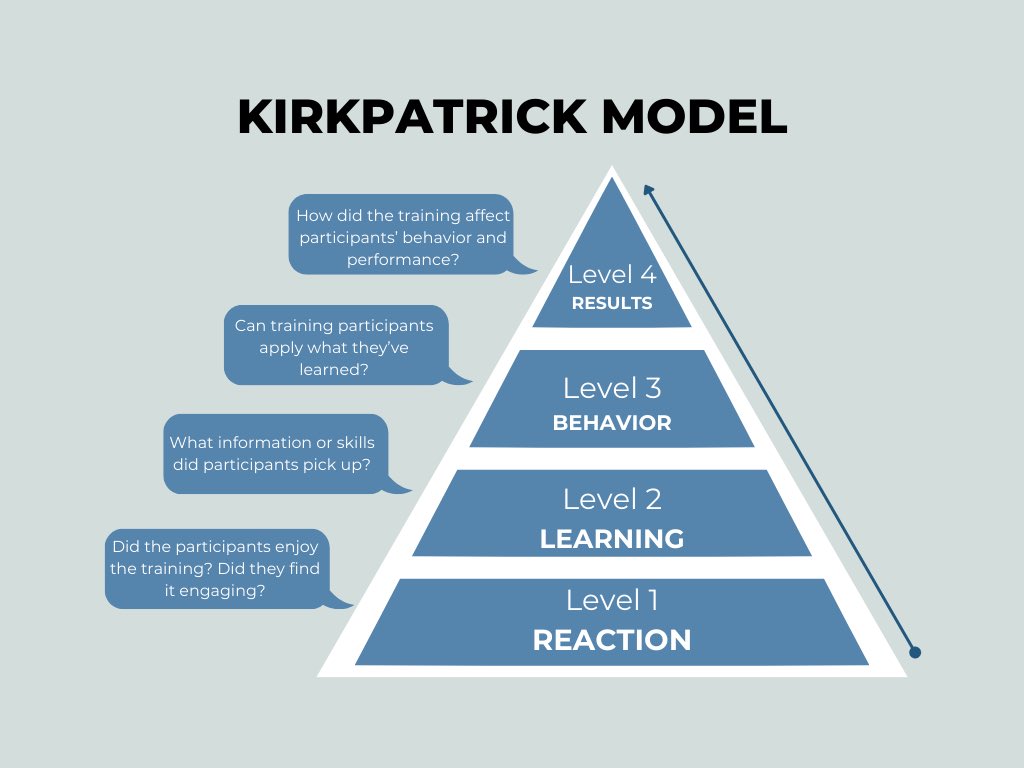
I’m reading the abstract of a #MedEd paper aloud, and my teenage son says, “So what if the students liked the curriculum? Did they actually learn anything or remember any of it six months later?”
I was >20 years older than him when I got that concept.
Newsflash: A randomized controlled trial supports a treatment that millions of patients been using over the last 70+ years!
This could have gone two ways, and speaking on behalf of everyone who cares about MG care, all I can say is... Phew!
https://t.co/VVa3wQcFyy
As Assyrian King Tull-apil-esharra III (745-727 B.C.E) obviously knew, a posterior interosseous neuropathy causes finger drop without wrist drop.
#detroitinstituteofart
SPOILER ALERT!
Join @zach_london, Jim Dolbow and me for the Neurogon Trail game show on Monday at the #AANAM@AANmember on Monday, 11:30 a.m. at the Head Talks stage!
Dear neurology trainees, throughout your career, you will encounter hundreds of patients with presentations you've never seen before. That is when applying the basics becomes most crucial. Define the tempo, localization, and syndrome, then proceed to differential and work up.
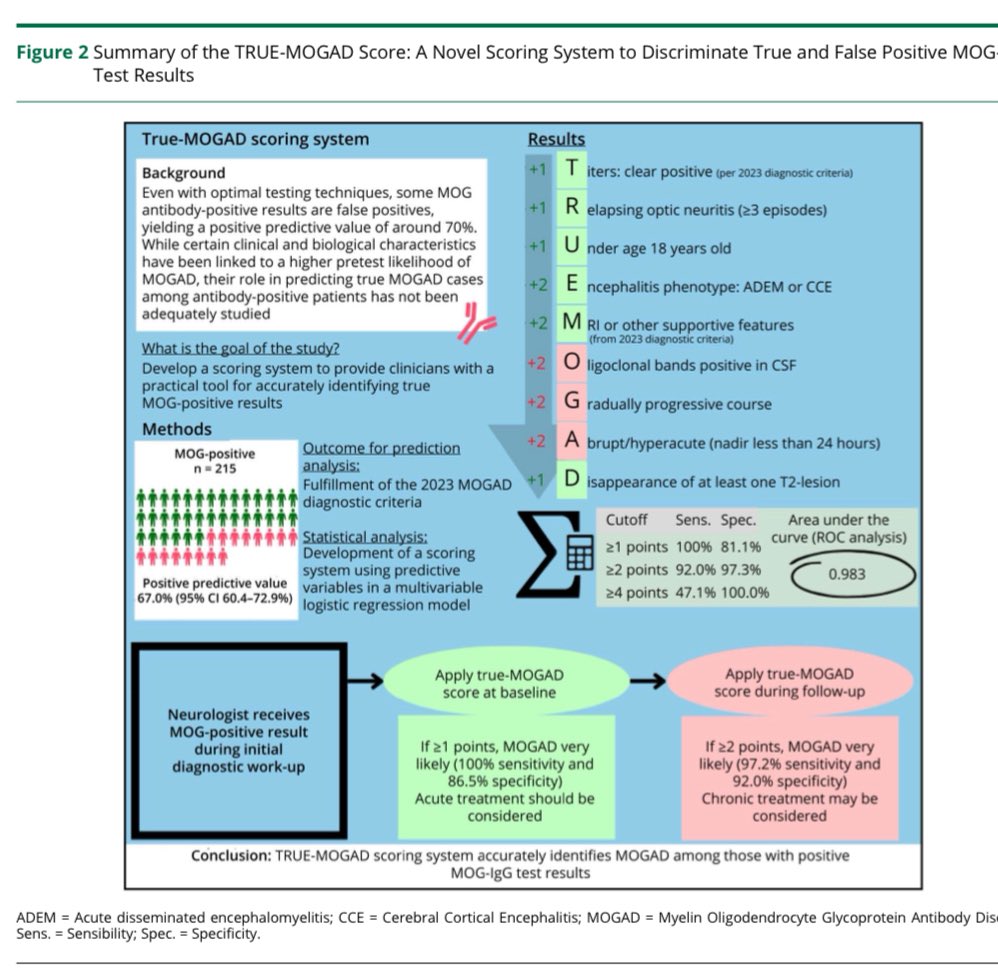
A positive MOG antibody result does not always mean MOGAD‼️
TRUE MOGAD Score helps neurologists worldwide estimate whether a positive MOG result is truly clinically meaningful.
Proud collaboration between @MayoClinic and @JohnsHopkins
Scan the QR code below to access the tool 👇🏽
Key Point 1 from the article Neurologic Complications of Critical Illness by Dr. Shivani Ghoshal from the February #Neurology of Systemic Disease issue, which is available to subscribers at https://t.co/xwNcCC7N9M. #NeuroTwitter#MedEd
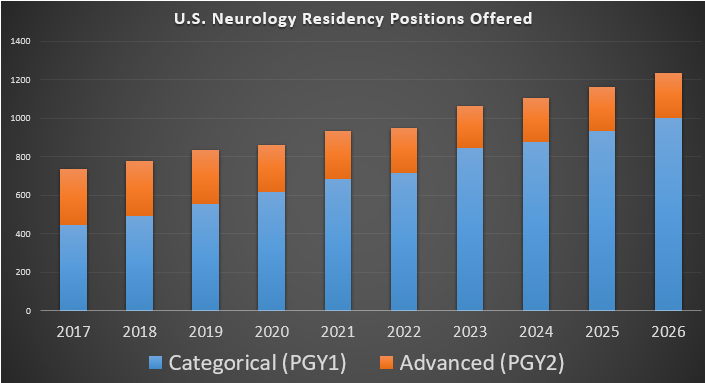
The Match is over. How did #neurology do as a whole?
First of all, the number of neurology residency slots is now at 1236. It keeps increasing, mostly driven by categorical programs.
Not shown in this graph, but this number has more than doubled since 2011.