se publicó el libro de “ Electrocardiograma” de @CONAREC_ORG 👏🏻🫶🏼
En 2021 cuando éramos residentes de @ArgerichCardio con mis colegas/amigos @JulianColla_ y @luciahelguera participamos de este proyecto de escribir el capítulo 10.
Hoy está al alcance de todos 🫶🏼
Terapia antitrombótica después de la cirugía de revascularización coronaria (CABG). 💊💥🫀
💊Aspirina: la piedra angular. La aspirina reduce la oclusión de injertos y los eventos CV sin incrementar significativamente el sangrado postoperatorio.
✅Mantener aspirina perioperatorio.
✅Reiniciarla dentro de las primeras 24 horas tras cirugía (idealmente antes de las 6 horas).
✅Continuar de forma indefinida a dosis bajas (75-100 mg/día).
💊💊¿TAP Dual? En pacientes con alto riesgo isquémico y bajo riesgo hemorrágico, puede considerarse aspirina + ticagrelor o clopidogrel durante 12 meses (indicación mas fuerte en SICA que en SCC) para mejorar la permeabilidad de los puentes venosos (reducen MACE pero aumentan 🩸).
✅Reiniciar TAPD tan pronto como el riesgo de sangrado esté controlado.
✅Mantenerla durante 12 meses.
✅Ticagrelor o prasugrel son preferibles a clopidogrel por su mayor reducción de eventos isquémicos y mortalidad.
📄🆓️⤵️ @ESC_Journals 💯
https://t.co/IcdxvQsTD9
https://t.co/SeTF6YUsXm
🫀⚠️ SCOT-HEART changed cardiology with one simple idea:
👉 First scan. Then treat.
This is going to generate some hitching to some colleagues within the community 😁. Sorry about that.
And 10 years later…
the message is even more disruptive.
For decades, we built cardiology around:
👉 ischemia
👉 stress tests
👉 flow limitation
Find ischemia.
Open arteries.
Simple.
Except… it didn’t reduce hard events consistently.
SCOT-HEART helped expose the problem:
👉 Atherosclerosis—not ischemia—is the real disease.
At 10 years:
👉 coronary CT guidance reduced:
- coronary death
- non-fatal MI
despite:
❌ NO increase in revascularization
Let that sink in.
Patients did better NOT because we opened more arteries.
They did better because:
👉 we identified plaque
👉 intensified prevention
👉 treated biology earlier
The most important number may not be stenosis anymore.
It may be:
👉 total plaque burden
👉 plaque phenotype
👉 lipid-rich disease
👉 adverse plaque features
The paper says it clearly:
Patients with:
⚠️ low-attenuation plaque
⚠️ positive remodeling
had dramatically higher event rates.
This is the paradigm shift
From: ❌ ischemia-centered cardiology
To: 👉 plaque-centered prevention
And the implications are enormous.
Because suddenly:
👉 non-obstructive CAD matters
👉 “normal” stress tests become insufficient
👉 anatomy alone becomes incomplete
Even more interesting
The next frontier is already here:
⚡ Photon Counting CT
⚡ AI-driven plaque analysis
⚡ Radiomics
⚡ Quantitative phenotyping
My take
SCOT-HEART did not simply validate coronary CT.
It challenged the entire logic of modern cardiology.
We used to ask: 👉 “Is this lesion ischemic?”
Now the real question is: 👉 “How biologically dangerous is this patient?”
Bottom line
The future is not:
👉 detect stenosis
👉 react late
It is:
👉 detect atherosclerosis early
👉 personalize prevention aggressively
⚡ Because myocardial infarction often starts long before ischemia appears.
#SCOTHEART #CCTA #Cardiology #Atherosclerosis #PlaqueImaging #Prevention #PhotonCounting #AI #PrecisionMedicine
Un gran honor haber escrito Junto a @JulianColla_@cardiologiamn y @CardioBornan un capítulo para este gran libro que no tengo dudas será un texto de referencia en #ECG de habla hispana
Muchas gracias @adribaran y @distribuna por la invitación 🙌🏼
https://t.co/JWYSXikNNe
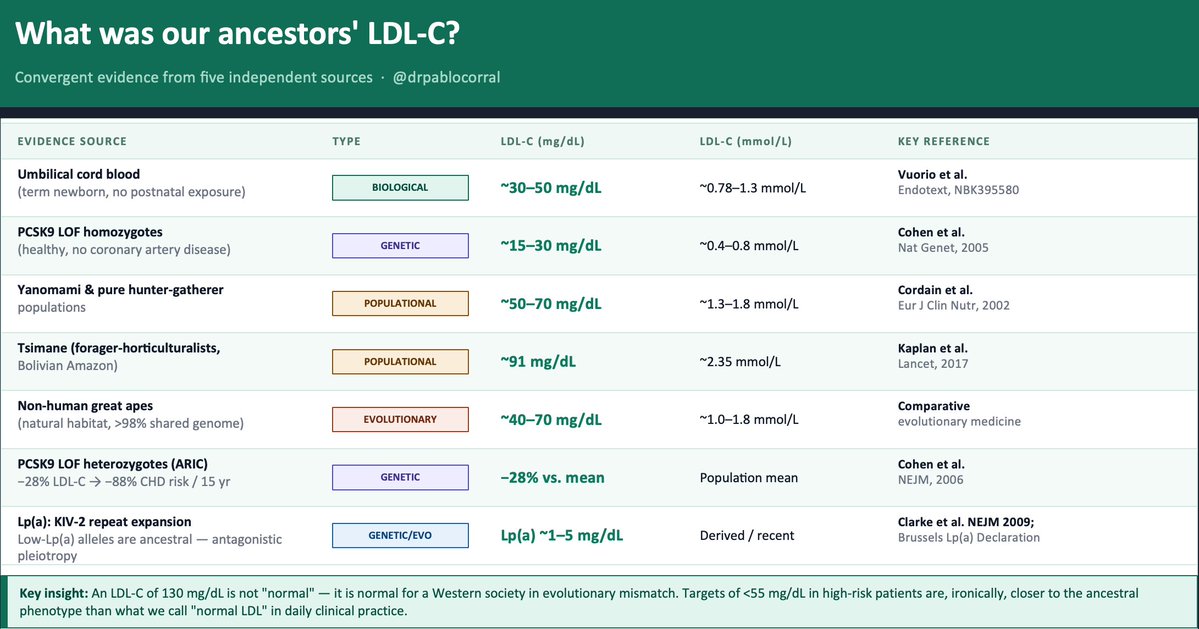
👉 We spend decades arguing about how low to push LDL-C
👆 Almost no one asks the obvious question:
🤔 How much LDL-C did our ancestors actually have?
The evidence exists — five independent lines, all converging on the same uncomfortable answer.
1️⃣ The term newborn. Before any dietary or metabolic influence, a healthy neonate arrives with LDL-C of ~30–50 mg/dL. That is the LDLR operating without environmental interference. Everything that rises after birth is acquired.
2️⃣ The Tsimane (Kaplan et al., Lancet 2017) — forager-horticulturalists of the Bolivian Amazon — have a LDL-C between 70 to 90 mg/dL and the lowest prevalence of coronary atherosclerosis ever recorded in any human population. Five times less than the U.S. in adults over 75. And their LDL is rising as roads and processed food arrive.
3️⃣ PCSK9 loss-of-function variants. African American carriers of nonsense mutations (Y142X/C679X, ~2% frequency): −28% LDL-C and −88% CHD risk over 15 years (Cohen et al., NEJM 2006). Homozygous LOF carriers live with LDL-C of ~15–30 mg/dL. Perfectly healthy. Nature already ran the trial.
4️⃣ Evolutionary genetics. Recent positive selection signals exist on gain-of-function PCSK9 variants that raise LDL-C — likely adaptive in food-scarce ancestral environments. Modern hypercholesterolemia is not "normal." It is an ancestral survival advantage turned pathological by evolutionary mismatch.
5️⃣ Great apes in natural habitat: ~40–70 mg/dL LDL-C. Same genome. Different environment.
👆 Bonus — Lp(a). The KIV-2 repeat expansion that raises Lp(a) is a derived, recent variant. Low-Lp(a) alleles are ancestral. Elevated Lp(a) is a textbook antagonistic pleiotropy signal — possibly protective against bleeding early in life, atherogenic over decades
📍The convergent estimate: ancestral LDL-C was ~30–70 mg/dL.
📍An LDL-C of 130 mg/dL is not "normal." It is normal for a Western society in evolutionary mismatch. Targets of <55 mg/dL in high-risk patients — which still feel aggressive to many clinicians — are, ironically, closer to the ancestral phenotype than what we call "normal LDL" in daily practice.
🤔 The question is not "is it safe to lower LDL this much?"
The question is: why did we let it rise this high?
@society_eas@nationallipid
DOCUMENTO AHA 2026 SOBRE DIETA PARA MEJORAR LA SALUD CARDIOVASCULAR
Minimizar
🔴Bebidas y alimentos azucaradas🥤🍬
🔴Alimentos con alto contenido de sodio 🧂
🔴Alimentos ultraprocesados
🔴Alcohol 🍷
Vía @CircAHA
https://t.co/ccowWcTiJn
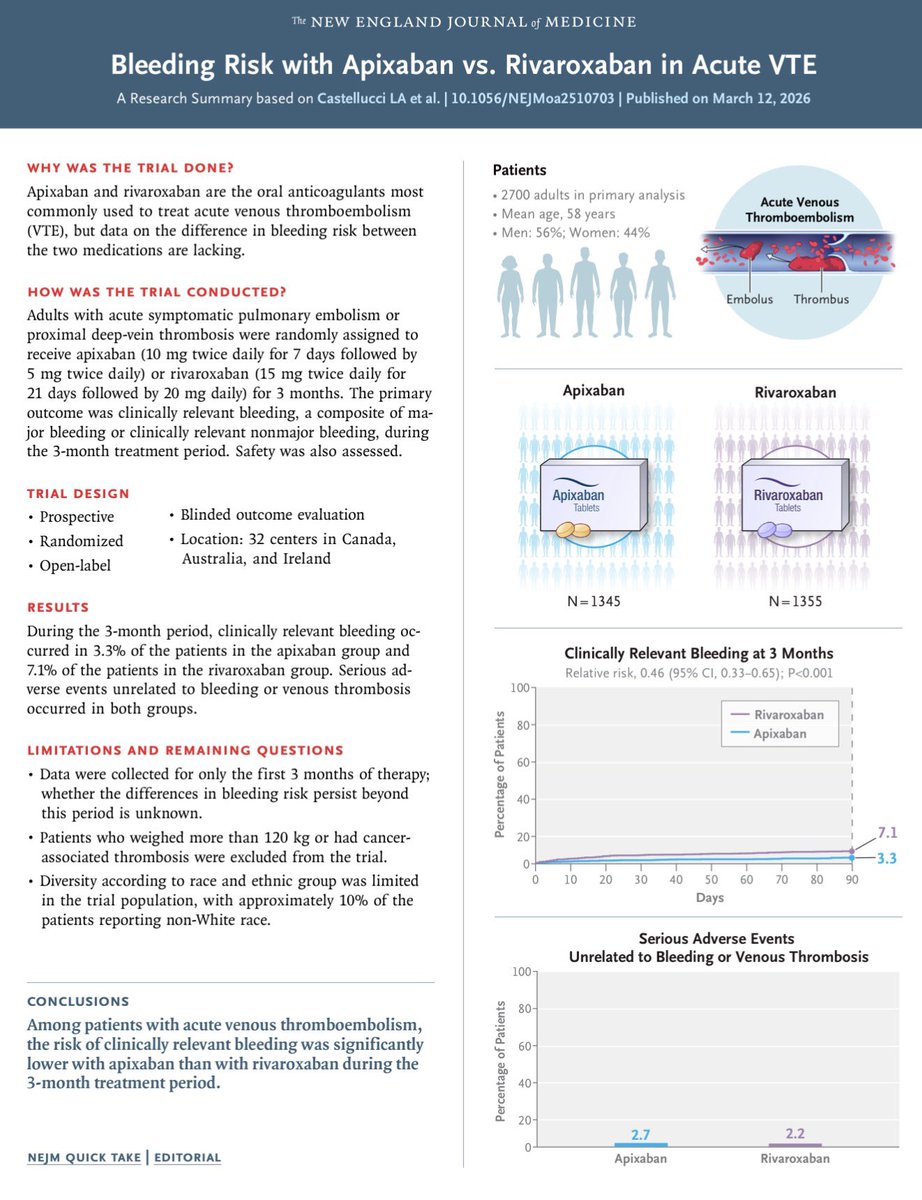
🚨 New head-to-head RCT in @NEJM: apixaban vs rivaroxaban 🥊
🏆 Apixaban emerges as the safe winner, with half the risk of bleeding complications
💡 For patients at high risk of GI bleeding, apixaban may be preferrable to rivaroxaban
https://t.co/Drqxr1kDu4
Clopidogrel outperformed aspirin in preventing cardiovascular events in patients with coronary artery disease (CAD), showing superior efficacy across both genders, in PANTHER-2 trial. https://t.co/XqH9rADKHp
📊 Los 5 artículos más leídos de 2025
Los contenidos que marcaron agenda, generaron debate y aportaron evidencia clave para la cardiología de nuestra región.
Descubre cuáles fueron los más leídos este año en este hilo 🫀📚
#SIAC#Cardiología#ArtículosCientíficos#Evidencia #SaludCardiovascular
🔬 La inflamación ya es un factor de riesgo CV tratable
⚠️ hsCRP >2 mg/L predice eventos CV incluso con LDL <70
💊 Colesterol bajo ≠ riesgo bajo si la inflamación persiste
🫀 Medir y tratar la inflamación es prevención cardiovascular moderna
⛓️💥https://t.co/ArkGIdEDeq
1/10 🚨2040: De “Just stent it!” a la era METAL-LESS.
🛑 Serruys et al (EHJ 2025) pronostican el fin de la revascularización mecánica universal.
🚀Nace la “imagenomics” (imaging + omics + IA) p/ decidir entre revascularización farmacológica🆚 mecánica.
🔜El futuro ya empezó
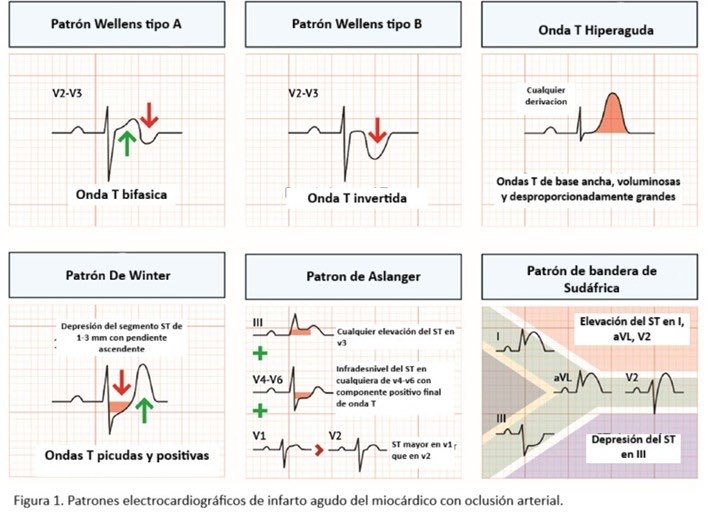
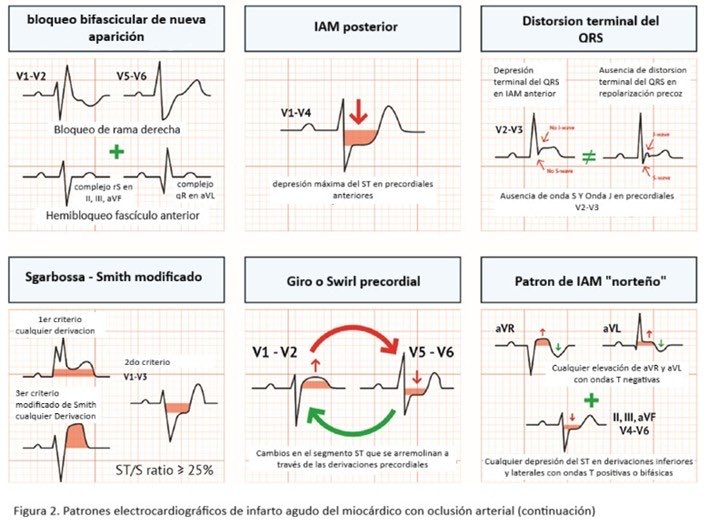
🩺 Nuevo artículo en #SIAC: “Patrones electrocardiográficos de oclusión coronaria en infarto agudo de miocardio” por el Dr. Julián Colla
🔍 Explora cómo los criterios STEMI/NSTEMI pueden subestimarse, identifica los 11 patrones de “STEMI-equivalentes” y adopta un enfoque más preciso con el modelo OMI/NOMI.
➡️Lee el artículo completo en https://t.co/6mpfae6bOU
Revascularization in Ischemic Left Ventricular Dysfunction: a pathophysiology-guided, evidence-based approach
Trials of routine coronary revascularization for iLVD have shown neutral results except for a benefit of CABG emerging beyond 5 years from surgery, supporting a selective pproach that is pathophysiology guided and tailored to the individual patient’s needs.
@JACCJournals@ACCinTouch@CMichaelGibson@DrMarthaGulati@iamritu@biljana_parapid@AnastasiaSMihai@Hragy
#Cardiology #MedTwitter #CardioTwitter #HeartHealth #Healthcare
https://t.co/EjFeYGuHNO
Les recomiendo leer esta revisión sobre PATRONES ELECTROCARDIOGRÁFICOS EN OCLUSIÓN CORONARIA E INFARTO AGUDO DE MIOCARDIO
#STEMI#NSTEMI
Por @JulianColla_ 🇦🇷 para @SIAC_cardio
https://t.co/rM6hldGjxR
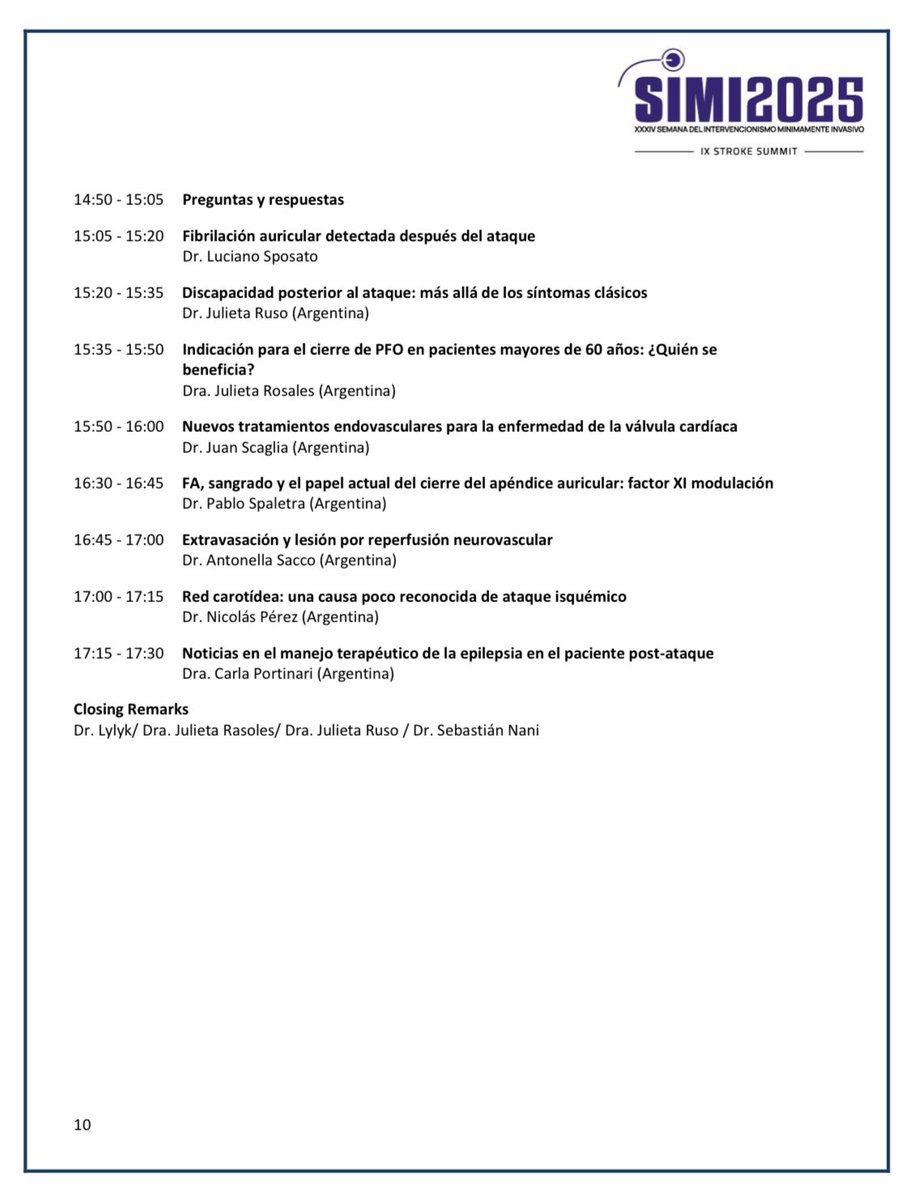
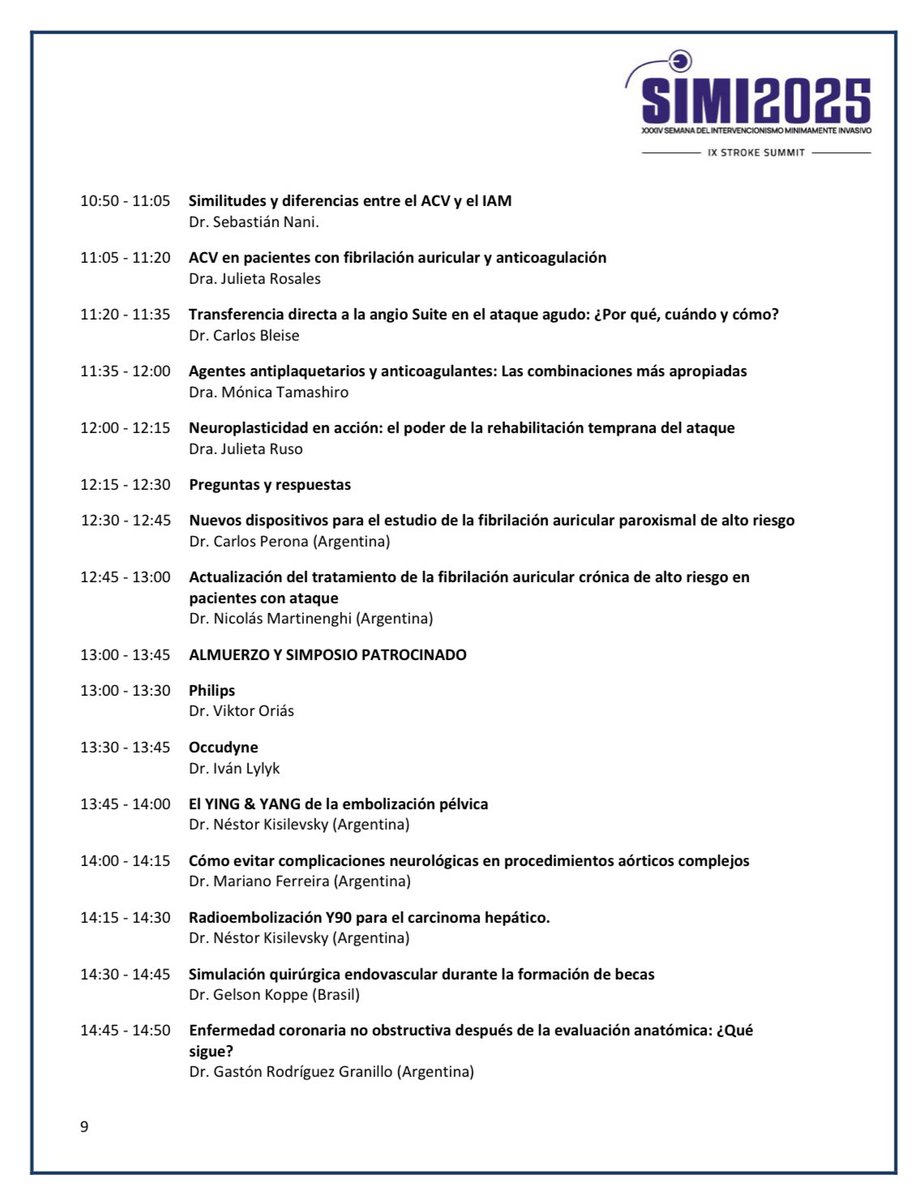
El próximo Jueves 25/9, junto a grandes colegas, participaré en la sesión de neurocardiologia del Congreso #SIMI2025
“CARDIOMETABOLISMO Y STROKE”
📍Alvear Icon Hotel, Puerto Madero, BsAs 🇦🇷
Inscripción 🆓
LOS ESPERAMOS!!!
Más info https://t.co/fZ1EftWNIQ
@eneri_neuro
Clopidogrel versus aspirin for secondary prevention of coronary artery disease: a systematic review and individual patient data meta-analysis: @TheLancet
🥸Plavix for secondary prevention may be superior to aspirin
😱 Summary
👇👇👇
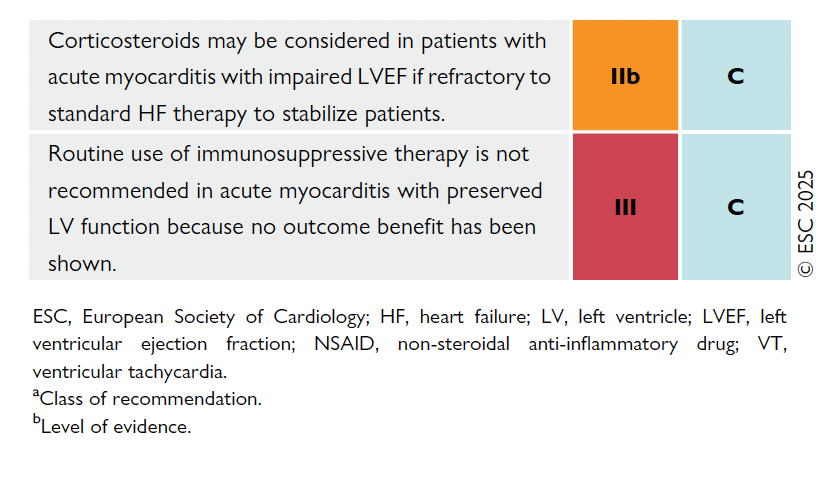
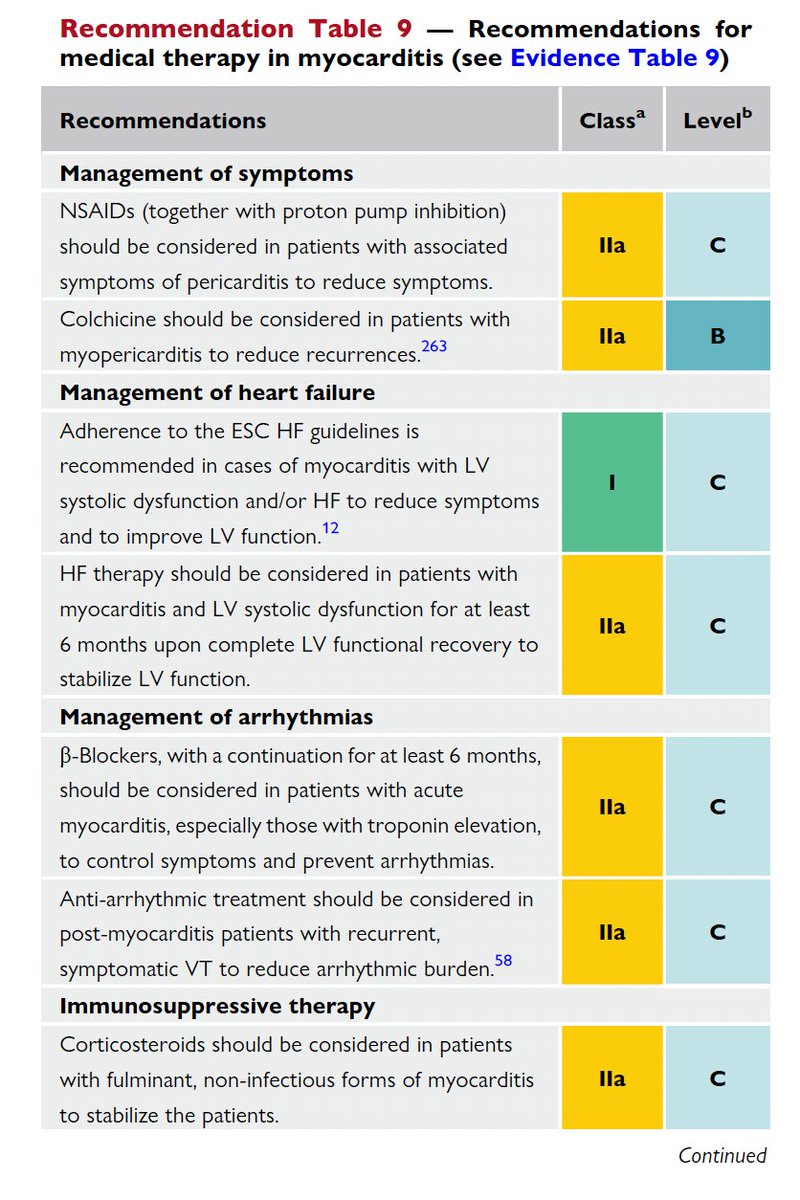
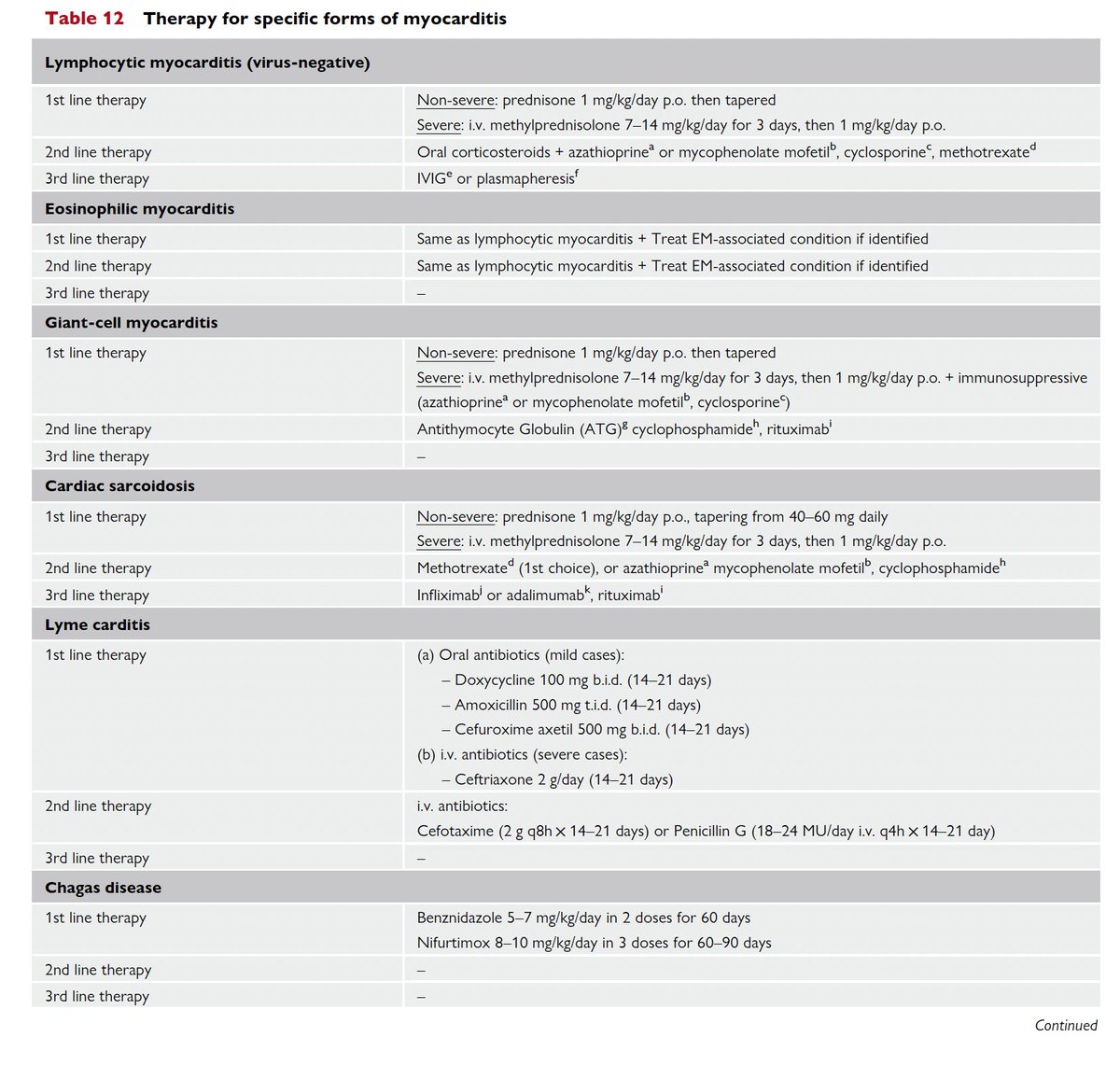
GUÍAS ESC 2025 MIOCARDITIS Y PERICARDITIS
#ESCCongress 6/10
Miocarditis
🔴Aspirina o AINES en 👥 con pericarditis asociada IIB LOE C
🔴Colchicina para evitar recurrencias IIB LOE B
🔴Considerar Betabloqueantes por 6 meses en pac con troponina + IIA LOE C