The 2 Longevity Fields...
New post on a topic of great importance.
Long, but something I feel strongly about.
Broadly Slowing Aging
vs.
Divide-and-Conquer Rejuvenation:
How to tell the difference and why acknowledging both matters
(link in next post)
Social algorithms are weird. I made the same exact post on LinkedIn 1 min before I did here & the post here has 750+ impressions but the LI algorithm decided to bury it so it has 14 impressions there after same amount of time.
https://t.co/1UzZxIMzVk
Sometimes it's the reverse.
Medipost gets US FDA okay to do only 1 phase 3 trial of Cartistem
https://t.co/RXRciNZEct
Huh? One wonders why US needs its own ph3 at all after 30,000 people dosed in Korea w/ 5-7 year follow-up structural benefit published papers
& then a successful ph3 in Japan where it met all primary & secondary endpoints.
Medipost gets US FDA okay to do only 1 phase 3 trial of Cartistem
https://t.co/RXRciNZEct
Huh? One wonders why US needs its own ph3 at all after 30,000 people dosed in Korea w/ 5-7 year follow-up structural benefit published papers
& then a successful ph3 in Japan where it met all primary & secondary endpoints.
I prev noted Mesoblast's Ryoncil/remestemcel-L as 1st allogeneic MSC therapy to get to approval (2024). That's true for FDA approval, but for regulatory approval by any national regulator it was beaten by Medipost's Cartistem allogeneic MSCs for OA in South Korea in 2012!
2/7
How is this not over-conservatism? Is someone seriously weighing the harms of delay vs. potential harm of approval & coming up w/ more net negative from approving? Is someone checking their math? This looks like a classic example of "do no harm" gone too far.
@julianweisser@celinehalioua Does 'cancer drugs' sound like the opposite of what people with cancer want?
Allergy drugs for those with allergies?
Diabetes drugs?
Etc.
Isn't "<name of bad medical issue> drugs" the common phrasing?
@MotionlessStall@celinehalioua Agree: 'aging' not 'longevity'
~90sec slide presentation on the slide version of that thread of mine here, from my Vitalist Bay 2026 talk:
https://t.co/F1V3rMTMsE
@mattwridley Trends in max height f/ Earth of a crewed vehicle was a terrible predictor of future level:
https://t.co/uI250lor9D
Lack of big max lifespan change isn't a good counterargument to belief it will rise decades from now. A lot can change in 1 decade (Apollo). 50yrs is a long time.
Using lifespan achieved to measure aging/longevity field progress is like measuring progress to the moon in the Apollo era in height achieved. It hides huge amounts of progress.
The ultimate goal is not necessarily the right metric for measuring incremental progress on the way.
@KrisMBarnes Good historical milestone to map. All the fields pursuing aging mitigation should try to develop narratives that map past & future milestones to better estimate confidence intervals on rates of future progress.
Most of NIA is Alzheimer's disease specific research. The Division of Aging Biology within NIA is where aging research lives, and it's funding is a what is a joke. It gets 2 orders of magnitude less than cancer per death caused. See the report that started this thread. How can you seriously say this in a thread where that report was the top post?
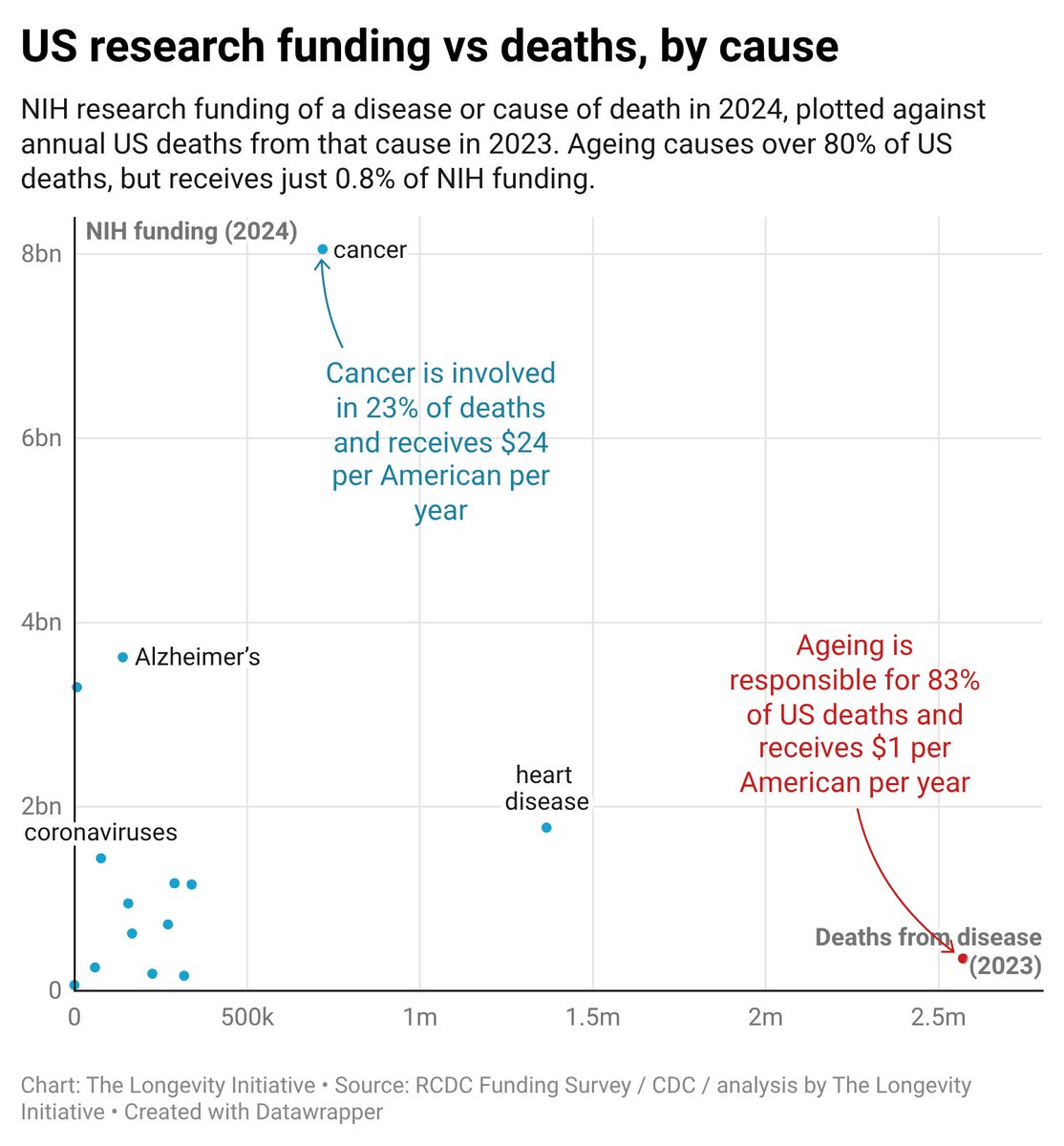
Does NIH research funding track what actually kills Americans?
Building on @theA4LI’s new report, we ran the numbers: and ageing fares worst.
Ageing causes 83% of deaths, yet receives just 1.2% of the research funding per death that cancer does—around $1 per American per year.
Aging is the pathology. It IS all about aging as the thing that needs fixing since it kill 70%+ of all humans (100k+ deaths/day). Replacement, rejuvenation, & slowing aging are different approaches to the problem.
I don't think anyone thinks the replacement approach is a joke. It's getting serious attention: Jean Hebert has a well funded ARPA-H program. There's a serious journal article w/ top people in the field on it: https://t.co/L4wsYJBT0p
There was a workshop at ARDD about it, also with top people in the field. Here's the report about it, also published: https://t.co/PcBGL6i8py
For 10-15 years now it's the divide-&-conquer rejuvenation (aka damage-repair) that has been the unloved sibling to the slow-aging approaches. See https://t.co/0dLLl3I0Q0
And now even Aubrey who was the only one really publicly advocating that strategy is not a loud voice doing so anymore & no one else really is. See:
https://t.co/KaakKUUq6D
Remember that rejuvenation & replacement are basically overlapping at all levels of granularity except for whole-body replacement. See:
https://t.co/vEhz4STgEb
I don't think whole-body replacement is a joke. It would be great. But I think there are a lot of technical challenges to solve & think they are more difficult than prominent advocates think they are. Plus, there are serious societal acceptance challenges that are hard to estimate the difficulty of. Appreciating the magnitude of that challenge is not the same as treating the idea as a joke.
I don't know why public perception & media slants (your # 1 & 2) should be taken into account when deciding science budgets. Sounds weird.
As for difficulty, I don't think it's as clear as you think it is. There are many signs that aging is not "far more difficult" as you suggest:
The Dublin Longevity Declaration expressly claims moderate longevity improvements are clearly achievable and radical longevity is feasible enough to justify significant resources to pursue it. 2708 people signed this declaration as of the end of 2025, including roughly ¼ of the most cited experts in aging and longevity (per Expertscape as of 2024).
Clearly Alzheimer's has not be easy to solve. Hundreds of times as much funding as the aging field has seen has gotten us not very far. Cancer explicitly evolves its way around treatments. The problems in biological aging don't do that. Eg once we figure out how to kill senescent cells, those solutions will keep working.
The targets the aging field goes after are upstream in causal chains of the disease-specific targets that the disease-specific treatments go after. It's often better to go after the steps earlier in the causal chain.
We have no idea what the success rate will be for trials & clinical programs going after aging targets because we are just now starting to get them through trials, so there aren't enough datapoints, but it's hard to imagine that the field in aggregate will end up with a worse track record over the next 1-2 decades than Alzheimer's had over the past 1-2 decades.
@ReddDrift I agree that difficulty should be factored in. My statement was that it makes no sense that disease burden is NOT factored in. There's no process for seriously assessing either disease burden or tractability. Budgets are primarily based on inertia (prior budgets) & lobbying.
@canonicalmodel Your comment is completely off topic here. Aging is clearly not the result of government policy. All humans who live long enough experience adult biological aging. It is degenerative & pathological universally across cultures & time. No conspiracy theory is needed or helpful.
@cremieuxrecueil Also, we've had Leqvio (2x/yr injection) approved for ~5 yrs already & siRNA is widely considered safer than gene therapy at the moment.
@cremieuxrecueil It's early days for PCSK9 drugs. Better in my mind to lower by the same amount via daily pill for the next couple decades then if all seems good one can get the gene therapy at any point. Not much hassle for the pill to those taking a handful of supplements or more a day anyway.
Enhanced games seems disappointing. I didn't pay attention or realize it was just steroids, HGH, etc. I was expecting exoskeletons, implants, new shoes, etc. & crushed records like 5hr English channel swims, 1h30min marathons, long jumps far enough to cross 50m rivers, etc.