"It will conduct clinical trials for local, national and international research initiatives https://t.co/vdynwZqvIl," @AcrpChapterKY. Story via @BusinessCourier.
The p-tau217 Alzheimer’s clock can now estimate when symptoms are likely to begin (new paper)
In a new study in Nature Medicine, a team at Washington University in St. Louis built a model that estimates, from one blood draw, the age at which someone is likely to start showing Alzheimer's symptoms. A marker clinicians already use for diagnosis is starting to look like a timeline.
The bottom line is that a single measurement of p-tau217 can now estimate when symptoms might begin within about three to four years.
🩸 p-tau217 is a tau molecule, but what drives its rise is amyloid, so it climbs early, around the time amyloid becomes detectable and well before tau tangles show up on a scan.
⏱️ In the study of 603 older adults, the model estimated the age of symptom onset within about three to four years, a bit like reading tree rings to tell how far along the process is.
📜 In 2025 the FDA cleared the first p-tau217 blood test to aid diagnosis, and in 2026 this work pushed the question from whether the disease is present toward roughly when symptoms may begin.
📉 The number is not fixed. Amyloid-clearing antibodies lower it by 35 to 39 percent, and even oral semaglutide moved tau-related markers, an early hint that the pathway can be reached.
🧬 No single marker carries the whole picture. p-tau217 is strongest read as part of a panel that also captures neurodegeneration and overall brain aging.
The timing idea fits how I have long thought about brain aging, placing a person on a trajectory rather than sorting them into positive or negative.
One finding I am still a little skeptical of is the claim that becoming positive later in life leaves less time before symptoms, because the age at positivity here was modeled rather than measured directly. I would want longer studies that follow the same people serially with p-tau217 before I take that one as settled. What does hold up is that the marker moves early and reads out from a simple blood draw, which is what prevention has needed.
The real gains will come from layering markers rather than relying on one. Combining p-tau217 with neurofilament light and multi-omic signals, including the RNA-based brain aging clock we use at NeuroAge, should sharpen the estimate of where someone sits and where they are heading beyond what any single number can do. That layered, multi-omics direction is where I expect prevention to go.
Full post: https://t.co/KCtEWS9vAb
#BrainHealth #Alzheimers #Longevity
@LaneLiverpool@euclid_vc “'Voice activation is available in many EHR platforms today, but availability alone hasn’t translated into meaningful adoption,' said @GeorgetownBrett, chief medical information officer at Louisville, Ky.-based @BaptistHealth. https://t.co/qB5qlo4NMM" via @BeckersHR.
📱 Digital phenotyping is transforming aging research by measuring cognition, behavior, symptoms & context in real life—not just in the clinic.
Join #MassAITC on Jun 23 at 4p ET with Raeanne Moore, PhD (@getNeuroUX@UCSanDiego)
🔗 https://t.co/Jq4Z7UiIwS
🧵 (1/3) #DigitalHealth
"But in a time when a single venture-backed AI company can snag $122 billion in a single round, biotech round sizes can’t compete for scale. https://t.co/WfV31kkgV5" by @jglasner.
I’ll never forget how 13 years ago, leaving Medicine for Entrepreneurship was viewed as heresy among some of my peers.
I still remember that physician who told me “oh, so you’re planning to make money off healthcare? That’s unethical”. Which I always found strange since her entire income came from healthcare.
Or another physician who said to me “you’re just doing this to become rich, right?”. It was doubly embarrassing because unexpectedly a friend of mine was sitting in on this meeting because she was a resident rotating with this preceptor.
The funny thing is I guarantee you both these physicians are far wealthier than I am (and probably always will be!).
Fast forward 13 years, and now we are seeing more physicians than ever before leave medicine for tech and entrepreneurship. The increase in burnout since 2020 certainly accelerated that, but this shift was already happening before then. For what it’s worth, if someone asks me if they should leave medicine to start a health tech company, I usually tell them it’s a bad idea - and if they do it anyways, then they were meant to do it, and I couldn’t have stopped them anyways.
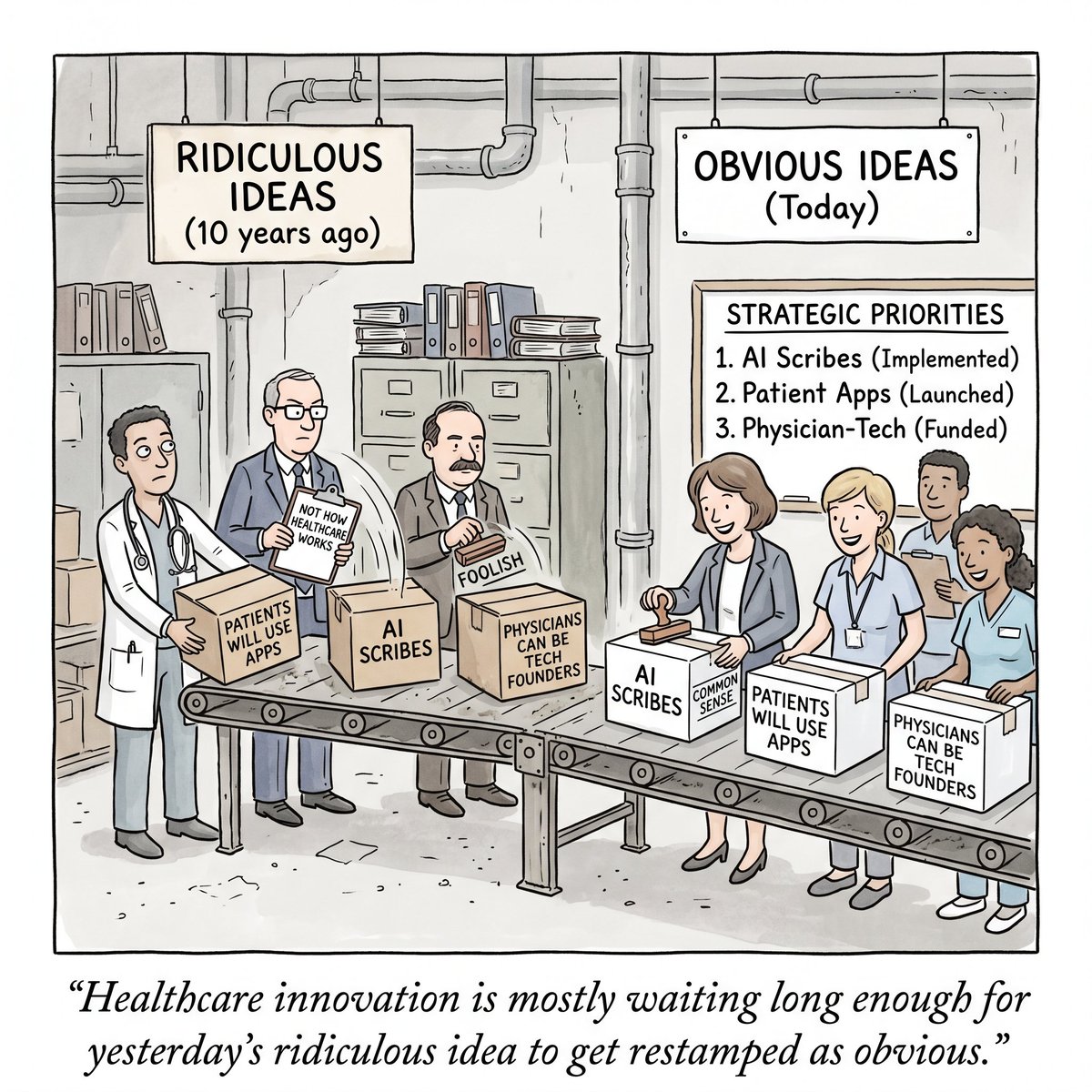
Similarly, starting @SeamlessMD to engage patients with digital health tech was perceived as a foolish idea by most. “Patients won’t use this!” Of course, it wasn’t until the pandemic in 2020 and the explosion of telemedicine / virtual care that healthcare woke up and realized “oh, actually patients CAN use technology".
Similarly, it took the emergence of ChatGPT to get health systems open-minded to AI scribes - despite a number of ambient companies starting before November 2022 (and just getting dismissed by health systems).
But this shift in sentiment over time does make me wonder: what is something today that the healthcare establishment is dismissing that will be “common sense” 13 years from now?
One of the biggest realizations is that these ideas don’t just become “common sense” magically. It takes a movement of people to lay the foundation for these “radical ideas” so that when a Black Swan event (e.g. a pandemic, the ChatGPT moment, etc.) happens, there is enough “kindling” already in place for the idea to spread like wildfire.
Transitioning from clinical to entrepreneurship, engaging patients with tech, using AI scribes - all of these could only be acceptable at scale because of folks who decided to just go ahead and try making it happen before it was commonplace.
Which means if you’re doing something kind of radical and no one gets it just yet - but you genuinely believe it’s making healthcare better… maybe don’t give up just yet. Maybe you’re onto something.
That’s how most innovations and movements start.
Because the best way to predict the future of healthcare is to go ahead and build it.
A look back at Abraham Flexner’s legacy highlights how one reform effort reshaped medical education across the country, raising standards, strengthening scientific training and redefining how physicians are prepared for practice. https://t.co/ToZ7JkMFdf
Food is—or as—Medicine.
Centenarians.
@halletecco's students wrote an awesome piece on AI startups' fundraising experiences.
#HealthDistilled by @LaneLiverpool. It's neat.
https://t.co/pIniYvRIor
@StinesAllison@BFLouisville “'But my career has been in biotech and there’s a pretty big biotech and technology hub in general in Boston. I’m really obsessed with the biotech industry and I know Louisville doesn’t have one. https://t.co/l5ke6XpIX6" via @BFLouisville.
@BFLouAllison @BFLouisville "OPINION: Greater Louisville is positioned to be the next global leader in biotechnology https://t.co/dQ6CrLRc3D" via @BFLouisville.
CenterWell Pharmacy has opened an $83 million Orlando-area central fill facility, joining a wave of pharmaceutical distribution expansion in Central Florida. https://t.co/ATcrbAZ5DX
At this year’s Senior Living Executive Conference in Nashville, Argentum President & CEO James Balda opened the State of the Industry with a clear message: senior living is not simply an industry, senior living is human. Read more at https://t.co/SruFcbgKH5
A complex cancer patient's record can run 300+ pages, and roughly 80% of it is unstructured: clinical notes, radiology, scanned PDFs, faxes from outside providers. Reading and reasoning over those records has required human judgment at every step, creating a bottleneck in nearly every workflow in cancer care.
@Triomicsinc has built the oncology-specific AI infrastructure to change that. We’re excited to lead the company’s $22M round, with @BrandonGleklen joining the Board of Directors.
Founders Sarim Khan (@k__sarim) and Raj Singh (@hrituraj1997) built Triomics with a clear philosophy: you need to deeply understand both oncology and AI workflows to know what “correct” means in the context of hundreds of pages of unstructured data. Their OncoLLM architecture reads the full patient record and produces a structured longitudinal profile that incorporates every clinical note, lab result and imaging readout.
Sitting on top of that foundation is a growing set of products that help oncology teams prepare for patient visits, identify eligible clinical trial candidates, populate disease registries and curate real-world data for research. Leading cancer centers and some of the nation's largest community oncology practices already trust Triomics to power their clinical and research workflows.
Congratulations to Sarim, Raj and the Triomics team. More on why we invested at https://t.co/ZEiWfG3rXf
I didn't know that a simple tool that I built would have an impact like this!
Last week, I built an AI tumor board, something to help me in my clinic to pull the most recent literature and approach a patient from multiple views, similar to what we do in a real-life tumor board, given the current clinical decision support tools lack that
To my surprise, this tool is being used in second- and third-world countries and places where they don't have access to Doximity and OpenEvidence
It's so satisfying to see that I'm able to help oncologists in other parts of the world!
I am not sure how long I can sustain this, but feel free to share this, and I will keep paying the tokens' price for now.
By the way, you don't need an account, and we don't save any data. This is a very simple user interface with a smart and simple backend
if you are a developer would love your thoughts on the GitHub.
https://t.co/O3j0Orp2Ts
Norton Cancer Institute is among the first in Kentucky to offer ExacTrac Dynamic, an advanced radiation therapy technology that improves precision, safety and patient comfort.
Learn more about this technology: https://t.co/0PJumD2pQm