🫀⚠️ 𝗙𝗮𝗹𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮́𝗺𝗶𝗰𝗮 𝗲𝗻 𝘀𝗲𝗽𝘀𝗶𝘀: 𝗲𝗹 𝗽𝗿𝗼𝗯𝗹𝗲𝗺𝗮 𝗻𝗼 𝗲𝘀 𝘀𝗼𝗹𝗼 “𝘃𝗮𝘀𝗼𝗱𝗶𝗹𝗮𝘁𝗮𝗰𝗶𝗼́𝗻”, 𝘀𝗶𝗻𝗼 𝘂𝗻𝗮 𝗱𝗶𝘀𝗿𝘂𝗽𝗰𝗶𝗼́𝗻 𝗴𝗹𝗼𝗯𝗮𝗹 𝗱𝗲𝗹 𝗰𝗼𝗻𝘁𝗿𝗼𝗹 𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿, 𝗰𝗮𝗿𝗱𝗶́𝗮𝗰𝗼 𝘆 𝗺𝗶𝗰𝗿𝗼𝗰𝗶𝗿𝗰𝘂𝗹𝗮𝘁𝗼𝗿𝗶𝗼🚨
@ElsevierConnect@sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
En sepsis la inestabilidad hemodinámica surge por la combinación de:
📉 Pérdida del tono vascular
🫀 Alteración de función cardíaca
🧬 Disfunción microcirculatoria y metabólica
👉 Todo esto es un determinante mayor de falla multiorgánica y mortalidad.
🧠 𝙇𝙖 𝙛𝙞𝙨𝙞𝙤𝙥𝙖𝙩𝙤𝙡𝙤𝙜𝙞́𝙖 𝙚𝙨 𝙢𝙪𝙘𝙝𝙤 𝙢𝙖́𝙨 𝙘𝙤𝙢𝙥𝙡𝙚𝙟𝙖 𝙦𝙪𝙚 “𝙛𝙖𝙡𝙩𝙖 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖”
La revisión resume varios mecanismos simultáneos:
✅ Exceso de 𝙤́𝙭𝙞𝙙𝙤 𝙣𝙞́𝙩𝙧𝙞𝙘𝙤 y prostaciclina
✅ Disfunción del 𝙨𝙞𝙨𝙩𝙚𝙢𝙖 𝙣𝙚𝙧𝙫𝙞𝙤𝙨𝙤 𝙖𝙪𝙩𝙤́𝙣𝙤𝙢𝙤
✅ Desensibilización catecolaminérgica
✅ Alteración del 𝙍𝘼𝘼𝙎
✅ 𝘿𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙧𝙚𝙡𝙖𝙩𝙞𝙫𝙖 𝙙𝙚 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖
💧 𝙇𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙩𝙚𝙧𝙖𝙥𝙞𝙖 𝙮𝙖 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙚𝙣𝙩𝙚𝙣𝙙𝙚𝙧𝙨𝙚 𝙘𝙤𝙢𝙤 𝙪𝙣𝙖 𝙢𝙖𝙣𝙞𝙤𝙗𝙧𝙖 𝙖𝙪𝙩𝙤𝙢𝙖́𝙩𝙞𝙘𝙖 𝙣𝙞 𝙪𝙣𝙞𝙛𝙤𝙧𝙢𝙚
Los fluidos siguen siendo fundamentales al inicio, pero su beneficio disminuye rápido fuera de la fase precoz.
Mensajes clave:
📌 La 𝙧𝙚𝙨𝙥𝙪𝙚𝙨𝙩𝙖 𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙨 debe valorarse activamente
📌 No basta con pensar en “respondedor a fluidos”; también importa la 𝙩𝙤𝙡𝙚𝙧𝙖𝙣𝙘𝙞𝙖 𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙨
📌 El exceso de fluidos favorece edema intersticial, disfunción orgánica y peor pronóstico
👉 El enfoque actual es personalizar volumen, velocidad y momento de administración.
💉 𝙀𝙣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨, 𝙡𝙖 𝙩𝙚𝙣𝙙𝙚𝙣𝙘𝙞𝙖 𝙖𝙘𝙩𝙪𝙖𝙡 𝙚𝙨 𝙢𝙚𝙣𝙤𝙨 𝙧𝙚𝙩𝙧𝙖𝙨𝙤 𝙮 𝙢𝙖́𝙨 𝙚𝙨𝙩𝙧𝙖𝙩𝙚𝙜𝙞𝙖 𝙢𝙪𝙡𝙩𝙞𝙢𝙤𝙙𝙖𝙡 𝙥𝙧𝙚𝙘𝙤𝙯
La revisión reafirma a la 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 como vasopresor de primera línea, pero resalta que prolongar o escalar demasiado la monoterapia catecolaminérgica puede asociarse a peor evolución.
Por eso propone pensar antes en:
➕ 𝙑𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖
➕ incluso 𝙖𝙣𝙜𝙞𝙤𝙩𝙚𝙣𝙨𝙞𝙣𝙖 𝙄𝙄 en escenarios seleccionados
Según una lógica de “soporte vasopresor multimodal”.
👉 El objetivo no es solo subir PAM, sino hacerlo con menor toxicidad catecolaminérgica y más racionalidad fisiológica.
📟 𝙀𝙡 𝙢𝙤𝙣𝙞𝙩𝙤𝙧𝙚𝙤 𝙝𝙚𝙢𝙤𝙙𝙞𝙣𝙖́𝙢𝙞𝙘𝙤 𝙪́𝙩𝙞𝙡 𝙣𝙤 𝙚𝙨 𝙚𝙡 𝙦𝙪𝙚 𝙙𝙖 𝙢𝙖́𝙨 𝙣𝙪́𝙢𝙚𝙧𝙤𝙨, 𝙨𝙞𝙣𝙤 𝙚𝙡 𝙦𝙪𝙚 𝙖𝙮𝙪𝙙𝙖 𝙖 𝙙𝙚𝙘𝙞𝙙𝙞𝙧 𝙢𝙚𝙟𝙤𝙧
El review enfatiza que la evaluación debe integrar:
🫀 𝙀𝙘𝙤𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙧𝙖𝙛𝙞́𝙖 𝙘𝙧𝙞́𝙩𝙞𝙘𝙖
📈 Parámetros dinámicos de respuesta a fluidos
🩸 Perfusión periférica, incluyendo 𝙩𝙞𝙚𝙢𝙥𝙤 𝙙𝙚 𝙡𝙡𝙚𝙣𝙖𝙙𝙤 𝙘𝙖𝙥𝙞𝙡𝙖𝙧
🧪 Lactato, pero interpretado con cautela
Además, subraya que no existe un biomarcador único perfecto de perfusión tisular.
👉 La resucitación efectiva sigue siendo multimodal y guiada por fisiología real, no por un solo marcador.
🎯 𝙏𝙖𝙠𝙚-𝙝𝙤𝙢𝙚: 𝙚𝙡 𝙛𝙪𝙩𝙪𝙧𝙤 𝙙𝙚𝙡 𝙨𝙝𝙤𝙘𝙠 𝙨𝙚́𝙥𝙩𝙞𝙘𝙤 𝙚𝙨𝙩𝙖́ 𝙚𝙣 𝙥𝙖𝙨𝙖𝙧 𝙙𝙚 𝙪𝙣𝙖 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙘𝙞𝙤́𝙣 𝙧𝙚𝙖𝙘𝙩𝙞𝙫𝙖 𝙖 𝙪𝙣𝙖 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙘𝙞𝙤́𝙣 𝙥𝙧𝙚𝙙𝙞𝙘𝙩𝙞𝙫𝙖 𝙮 𝙥𝙚𝙧𝙨𝙤𝙣𝙖𝙡𝙞𝙯𝙖𝙙𝙖
El artículo mira hacia adelante con varias líneas potentes:
🤖 Inteligencia artificial para anticipar deterioro hemodinámico
🧬 Biomarcadores más precisos, especialmente del eje 𝙧𝙚𝙣𝙞𝙣𝙖-𝙖𝙣𝙜𝙞𝙤𝙩𝙚𝙣𝙨𝙞𝙣𝙖
⚙️ Estrategias preventivas, no solo reactivas
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/tojooaa9Gy]
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
#Sepsis #SepticShock #Hemodynamics #Vasopressors
#FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada
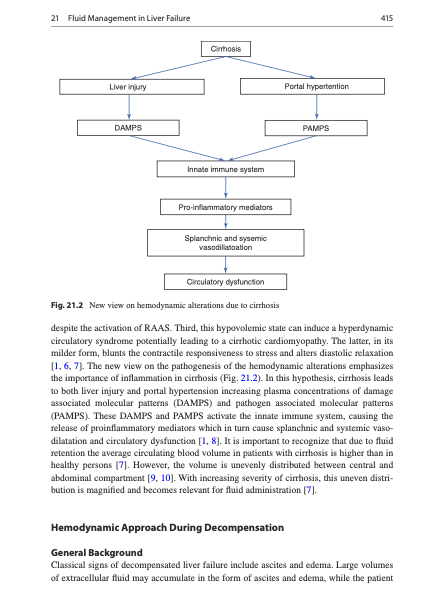
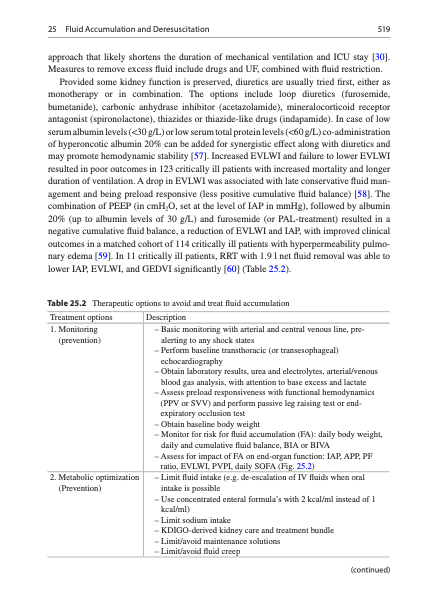
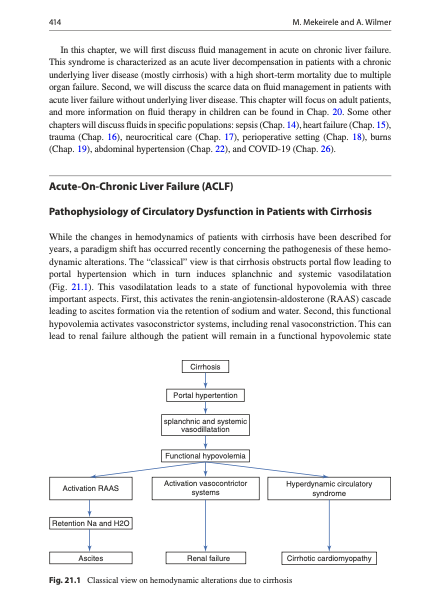
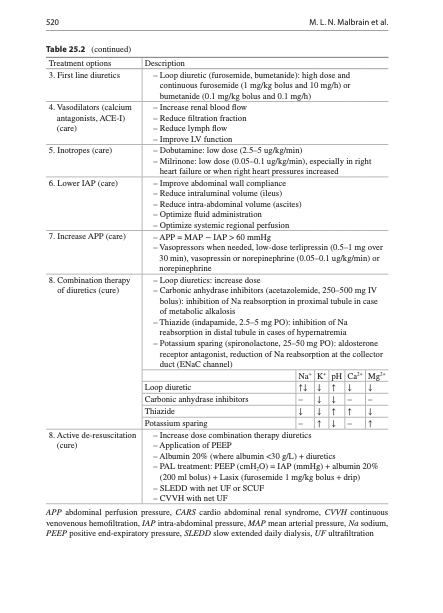
💧 Fluid Management in Liver Failure and Ascites
Circulatory Dysfunction and Effective Hypovolaemia
The liver failure chapter explains that despite edema and ascites, many patients with cirrhosis are effectively underfilled due to splanchnic vasodilation and low effective arterial blood volume. This creates a delicate balance: excessive fluids exacerbate ascites and hyponatraemia, while under‑resuscitation risks renal hypoperfusion and hepatorenal syndrome.
Albumin, Paracentesis and Vasoactive Drugs
The authors review indications and dosing for albumin following large‑volume paracentesis, in spontaneous bacterial peritonitis and in prevention/treatment of hepatorenal syndrome, drawing on key clinical trials. Practical tables link specific clinical situations (e.g. tense ascites, SBP, HRS) to albumin and vasoconstrictor strategies while reinforcing sodium restriction and diuretic stewardship.
📘 Full liver failure chapter in Rational Use of Intravenous Fluids in Critically Ill Patients:
👉 https://t.co/7pvDxZGh4I
🔵 IFAD 2026 will address albumin use and fluid management in decompensated cirrhosis and liver ICU.
👉Registration: https://t.co/wATwBWAIge
#LiverFailure #Ascites #Albumin #HepatorenalSyndrome #ICU
Updated guidelines for managing migraine in the emergency department: Intravenous prochlorperazine and greater occipital nerve blocks emerged as first-line interventions. Read key points: https://t.co/5rur3nCyCO
POCUS in Shock: The Modern ICU Stethoscope 🩺
The evaluation of hypotension in critically ill patients is a race against time.
The "Pump, Tank, Pipes" Approach
The most widely used protocol for undifferentiated shock remains the RUSH examination:
🫀 Pump • Cardiac function • Pericardial effusion/tamponade • Right ventricular strain • Global ventricular performance
🪣 Tank • IVC assessment • Intravascular volume status • Free abdominal fluid • Fluid responsiveness clues
🩸 Pipes • Pneumothorax • Aortic pathology • Deep vein thrombosis • Massive pulmonary embolism indicators
This systematic approach allows clinicians to rapidly classify shock as hypovolemic, cardiogenic, obstructive, or distributive.
Why POCUS Changes Management
Structured ultrasound protocols improve diagnostic accuracy from approximately 60% with clinical examination alone to 85%, while altering management decisions in up to 50% of patients.
In many cases, POCUS provides the decisive clue before laboratory or radiologic confirmation becomes available.
Lung Ultrasound: A Critical Extension
Lung ultrasound has transformed bedside respiratory assessment.
Key findings include:
🌊 Diffuse B-lines • Suggest pulmonary edema • Sensitivity ≈94% • Specificity ≈92%
🏖️ A-lines • Usually indicate normally aerated lung
🚫 Barcode Sign • Supports pneumothorax diagnosis
🏝️ Seashore Sign • Normal lung sliding
In unstable patients, lung ultrasound frequently identifies life-threatening pathology faster than chest radiography.
The New Frontier: Venous Congestion and AI
POCUS is evolving beyond simple volume assessment.
Emerging applications include:
• Venous Excess Ultrasound Score (VExUS)
• Critical care transesophageal echocardiography (TEE)
• Automated AI-assisted image acquisition
• Real-time calculation of ejection fraction
• Automated IVC and stroke volume assessment
• Handheld ultrasound devices integrated into ICU workflows
These innovations may reduce operator dependence while expanding access to advanced hemodynamic assessment.
Important Caveat
One of the most valuable statements from this review is also one of the simplest:
"While POCUS is a powerful tool, it requires humility and awareness of its fallibilities."
Ultrasound should complement clinical reasoning, not replace it. Poor image quality, operator dependency, confirmation bias, and overreliance on isolated findings remain important limitations.
Reference 📚
Rowe M, Ferrada P. Ultrasound to guide critical decisions: What you need to know. Journal of Trauma and Acute Care Surgery. 2026;100(5):692–699. DOI: 10.1097/TA.0000000000004815.
🥤SODa-BIC Trial (NEJM 2026):
En 500 pacientes críticos con acidosis metabólica (pH <7.30) y choque, la infusión de bicarbonato de sodio NO redujo los eventos renales mayores a 30 días (40.2% vs 39.4%), ni la mortalidad hospitalaria (25.4% vs 24.0%).
Lo que sí:
✅ Corrigió más rápido el pH y disminuyó la recurrencia de la acidosis (32% vs 55.7%),
✅La necesidad de terapia de reemplazo renal fue numéricamente menor (16.8% vs 20.9%), pero sin diferencia estadísticamente significativa y sin mejores desenlaces clínicos.
El principal nicho que aún conserva respaldo es el paciente con acidosis metabólica severa + AKI avanzada, que fue donde BICAR-ICU encontró señal de beneficio, aunque ahora esa señal queda opacada por SODa-BIC.
Descarga: https://t.co/FVHTcMZflI
🚨 Cardio/ Toxicology pearls you should never miss 7️⃣
What is the rationale behind giving sodium bicarbonate in wide-complex tachycardia seen in toxicology emergencies such as TCA overdose?
The key issue is not simply the tachycardia it’s myocardial sodium channel blockade.
Tricyclic antidepressants (TCAs) like amitriptyline block fast Na+ channels in the His-Purkinje system and ventricular myocardium, slowing depolarization and producing:
🔸QRS widening
🔸Ventricular arrhythmias
🔶Hypotension
🔶Cariogenic shock
Sodium bicarbonate works through two mechanisms:
✅ Sodium loading:- Increases extracellular Na⁺ concentration, helping overcome drug-induced sodium channel blockade.
✅ Serum alkalinization:- Raising pH (target 7.50–7.55) increases protein binding of the toxin, reducing the free active fraction available to block cardiac sodium channels.
The result?
🔶Narrower QRS
🔶Improved conduction
🔶Reduced ventricular arrhythmias
🔶Improved blood pressure
Think of it as ‘flooding the system with sodium while simultaneously weakening the toxin’s grip on the sodium channel.
🔻TCA toxicity is the classic indication, but sodium bicarbonate is also used in other sodium channel blocker poisonings that present with wide-complex tachycardia.
Examples include:
🔶Diphenhydramine overdose
🔶Cocaine toxicity
🔶Propoxyphene toxicity
🔶Flecainide overdose
🔶Propafenone overdose
🔶Carbamazepine toxicity
🔶Certain class I antiarrhythmic overdoses
Clinical reminder :- Wide QRS + suspected sodium channel blocker toxicity = think sodium bicarbonate.
ECG clues:-
▪️QRS >100 ms → increased seizure risk
▪️QRS >160 ms → increased ventricular arrhythmia risk
🟩Takeaway point : Sodium bicarbonate is not merely correcting acidosis it is a targeted antidotal therapy that reverses cardiac sodium channel blockade, making it one of the most important life-saving interventions in toxicologic wide-complex tachycardia.
#Cardiology #Toxicology
📱🫁Utilidad del PoCUS en el Manejo del Embolismo Pulmonar con Inestabilidad Hemodinámica
🔰📚Critical Care 2026
https://t.co/ZscgQ8HpX6
Enlace a Artículo Completo👇🏻🆓✅
https://t.co/rPEDXf5xvO
❤️ Pressure-Volume Loops at the Bedside: Are We Finally Measuring What Really Matters in Cardiogenic Shock?
For decades, cardiogenic shock management has focused on cardiac output, blood pressure, filling pressures, lactate, and cardiac power.
A fascinating multicenter study published in the ASAIO Journal proposes a practical bedside method to estimate pressure-volume (PV) loop energetics using only pulmonary artery catheter and echocardiographic data, avoiding the need for invasive conductance catheters.
Why does this matter?
Traditional hemodynamic variables tell us about flow and pressure.
PV-loop analysis tells us about:
📌 Ventriculoarterial coupling (VAC)
📌 Ventricular efficiency
📌 Stroke work (SW)
📌 Potential energy (PE)
📌 Pressure-volume area (PVA)
📌 Myocardial energetic demand
These parameters may provide a much deeper understanding of whether a therapy truly unloads the failing ventricle.
Key Findings
🔹 Microaxial flow pump support in AMI-related cardiogenic shock
The most striking observation was a reduction in arterial elastance and improved ventriculoarterial coupling, accompanied by increased stroke work but decreased pressure-volume area.
This translated into an improvement in estimated ventricular efficiency from approximately 32% to 40%, suggesting genuine ventricular unloading and lower energetic expenditure.
🔹 IABP support in AMI-related shock
IABP improved ventriculoarterial coupling and reduced filling pressures but produced a more modest energetic effect compared with microaxial support.
🔹 Heart failure-related cardiogenic shock
The physiological response was far more heterogeneous. Changes in pressure-volume area and ventricular energetics were inconsistent, highlighting that device effects may depend strongly on shock etiology.
Why This Study Is Important
This work reinforces a concept increasingly discussed in advanced heart failure and shock programs:
The goal is not simply increasing cardiac output.
The goal is improving systemic perfusion while simultaneously reducing myocardial oxygen consumption and ventricular workload.
A patient can have a higher cardiac output while still operating at an unfavorable energetic state.
Pressure-volume analysis may reveal this hidden physiology.
Practical ICU Takeaway
When evaluating mechanical circulatory support, we should ask three questions:
1️⃣ Is systemic perfusion improving?
2️⃣ Is ventricular filling pressure decreasing?
3️⃣ Is ventricular energetic demand falling?
Only when all three occur simultaneously can we confidently say that true ventricular unloading has been achieved.
The future of cardiogenic shock management may be less about isolated hemodynamic variables and more about understanding the complete interaction between the ventricle and the arterial system.
Reference 📚
Ortega-Hernández JA. ASAIO Journal. 2026. DOI: 10.1097/MAT.0000000000002737.
🔰Asincronía paciente-ventilador: relevancia clínica, detección y estrategias de resolución🌀
"Mirar ondas en tiempo real salva más pulmones que cualquier número aislado."
▪️Las asincronías paciente–ventilador (APV) ocurre cuando el esfuerzo neural del paciente no coincide en inicio, magnitud o terminación con el ciclo mecánico del ventilador. Es frecuente en UCI (30–80% ) no es un fenómeno benigno.
📖Notas cafeteras ☕️
🫁 ↑ Trabajo respiratorio y fatiga diafragmática
▪️↑ disconfort, ansiedad y necesidad de sedación
▪️. ↑ duración de ventilación mecánica, fallos de destete
▪️ ↑ lesión pulmonar asociada al ventilador (VILI) (p. ej., doble disparo → volutrauma)
⚠️Asociación con mayor mortalidad cuando es persistente y no reconocida.‼️
🫁La asincronía no se corrige con un solo parámetro: es interacción drive–mecánica–modo.
🫁Doble disparo = riesgo de volutrauma aun con VT “protectores”.
🫁Inefectivos son la asincronía más común: piense en PEEPi.
🫁Reverse triggering sospeche con sedación profunda y ritmos “perfectos”.
🔰 Tipos principales de asincronía
a) De disparo (trigger)🔫
🔫Disparo inefectivo: esfuerzo no reconocido (PEEPi, sensibilidad inadecuada).🫁
🌀Auto-disparo: ciclos sin esfuerzo (fugas, agua en circuito, sensibilidad excesiva).
🔎b) De flujo
▪️El flujo entregado < demanda del paciente → disnea, uso muscular accesorio.⚠️
📛c) De ciclado
▪️Ciclado precoz: el ventilador termina antes del fin del esfuerzo neural.
▪️Ciclado tardío: el ventilador continúa tras cesar el esfuerzo.
⚠️d) Complejas
▪️Doble disparo: dos ciclos por un solo esfuerzo (tiempo inspiratorio corto, VT bajo, drive alto).
▪️Reverse triggering: el ciclo mecánico induce el esfuerzo neural (frecuente con sedación profunda).
🫁Detección en la práctica
🫁Clínica🧠🫀
▪️Taquipnea, uso de músculos accesorios, “lucha” con el ventilador, ansiedad.
▪️Monitoreo de ondas
-Presión: deflexiones negativas sin ciclo (inefectivo), picos abruptos (doble disparo).
-Flujo: retorno a cero con esfuerzo persistente (hambre de flujo).
-Volumen: VT duplicado en doble disparo.
🔧Herramientas avanzadas
▪️EAdi (NAVA) para sincronía neural.
▪️Análisis automatizado de asincronías (software/IA).
▪️Ultrasonido diafragmático (apoyo para esfuerzo y fatiga).
💡 Estrategias de resolución (enfoque paso a paso)
🫁A. Ajustes básicos (siempre primero)
1. Sensibilidad de disparo: hacerla más sensible (sin auto-disparo).
2. PEEP: reducir PEEP intrínseca (↑ PEEP externa cuidadosamente, ↓ FR, ↑ tiempo espiratorio).
3. Flujo inspiratorio: aumentar flujo o cambiar a patrón desacelerado.
4. Tiempo inspiratorio / criterios de ciclado: adaptar a la duración del esfuerzo neural.
5. Modo ventilatorio: considerar PSV optimizada, PCV, o modos proporcionales.
🫁B. Modos proporcionales
▪️NAVA / PAV+: mejoran sincronía, reducen sedación y asincronías complejas cuando están disponibles.
🫁C. Sedación y analgesia (uso juicioso)
🫠Tratar dolor y ansiedad antes que “profundizar” sedación.
⚠️Evitar sedación profunda innecesaria (↑ reverse triggering).
💉Bloqueo neuromuscular solo en indicaciones muy específicas y temporales (p. ej, SDRA grave refractario).
🫁D. Destete
✅️Optimizar carga/drive; asincronía no corregida = fracaso de destete.
‼️Asincronías paciente-ventilador en el paciente neurocrítico🧠
✅️Ventilación mecánica y neuroprotección
Por qué son especialmente relevantes en neurocríticos❓️
⏺️En el paciente neurocrítico (TCE, HSA, EVC, estatus epiléptico, encefalopatías), la asincronía no solo genera disconfort: impacta directamente la presión intracraneal (PIC), la perfusión cerebral (PPC) y la oxigenación cerebral.
🧠Cualquier aumento del trabajo respiratorio, tos, lucha o ventilación ineficiente puede elevar la PIC y comprometer el pronóstico neurológico.‼️
📈📉Asincronías más frecuentes y peligrosas en neurocríticos
A. Disparo inefectivo
Muy frecuente por:
💉Sedación profunda
▪️Drive respiratorio deprimido
▪️PEEP intrínseca (especialmente en neurocríticos con EPOC asociado)
👇🏽👇🏽👇🏽
🫀 The Most Dangerous Moment in the ICU May Last Less Than 60 Seconds
We often think of tracheal intubation as an airway procedure. Physiologically, it is a profound cardiovascular intervention.
Why Do ICU Patients Crash During Intubation?
The problem begins before the laryngoscope enters the mouth.
Many critically ill patients survive on a fragile compensatory state characterized by:
🔹 Endogenous catecholamine surge
🔹 Tachycardia
🔹 Vasoconstriction
🔹 Increased myocardial oxygen demand
What appears to be "stable" hemodynamics may actually represent physiological exhaustion.
The moment induction drugs are administered, this compensatory sympathetic drive disappears.
The result? A sudden reduction in:
• Systemic vascular resistance
• Cardiac output
• Coronary perfusion pressure
• Organ blood flow
This phenomenon has been termed adrenergic collapse.
Intubation Is a Hemodynamic Timeline
The authors propose viewing intubation as a sequence of cumulative threats rather than a single procedure:
1️⃣ Pre-induction adrenergic dependence
2️⃣ Sympatholysis after induction
3️⃣ Apnea, hypoxemia, hypercapnia, and acidosis
4️⃣ Transition to positive-pressure ventilation
5️⃣ Post-intubation ventilator and sedation effects
Each phase adds physiological stress.
Together, they can culminate in cardiovascular collapse.
The Propofol Question
One of the most clinically relevant findings is the growing evidence regarding induction agent selection.
In the INTUBE cohort, propofol was associated with a higher risk of cardiovascular collapse and was the only modifiable risk factor consistently identified.
The review therefore suggests:
✅ Ketamine
✅ Etomidate
as preferred induction agents in patients at risk of hemodynamic instability, while propofol should be used cautiously in shock states.
Positive Pressure Ventilation: The Forgotten Hemodynamic Challenge
Once the tube is secured, many clinicians relax.
The physiology is only beginning.
Positive-pressure ventilation:
🔹 Reduces venous return
🔹 Increases intrathoracic pressure
🔹 Raises right ventricular afterload
🔹 May precipitate right ventricular failure
This is particularly relevant in ARDS, pulmonary hypertension, pulmonary embolism, and severe hypoxemic respiratory failure.
Reference 📚
Kotani Y, Koroki T, Hayashi Y, Russotto V. The hemodynamics of tracheal intubation in critically ill patients: a narrative review. Journal of Intensive Care. 2026;14:42. DOI: 10.1186/s40560-026-00877-4.
🫀 Septic Shock Is Not Just About Blood Pressure: It Is About Ventriculo-Arterial Coupling
For years, septic shock resuscitation has focused on restoring MAP, increasing cardiac output, and normalizing lactate.
But what if the real problem is not flow alone?
What if the heart and arterial system are no longer working together?
This is the concept of ventriculo-arterial coupling (VAC): the dynamic interaction between ventricular contractility (Ees) and arterial load (Ea). When coupling is preserved, the cardiovascular system operates efficiently, maximizing stroke work while minimizing myocardial energy expenditure.
Why VAC Matters in Septic Shock
Sepsis causes profound vasoplegia, myocardial depression, and alterations in vascular tone.
As a result, many patients develop ventriculo-arterial uncoupling, where ventricular contractility and arterial load become mismatched. This leads to:
✅ Reduced cardiovascular efficiency
✅ Increased myocardial energetic cost
✅ Impaired tissue perfusion despite apparently adequate cardiac output
✅ Variable responses to fluids, vasopressors, and inotropes
In other words:
Two patients may have the same MAP and cardiac output but completely different cardiovascular efficiency and energetic burden.
The Norepinephrine Paradox
One of the most interesting concepts highlighted by Pinsky and Guarracino is that increasing blood pressure does not always improve cardiovascular performance.
In some septic shock patients with depressed contractility:
🔹 Norepinephrine increases arterial elastance (Ea)
🔹 MAP rises
🔹 Left ventricular afterload increases
🔹 Stroke volume may fall
🔹 VAC worsens
🔹 Cardiac output may remain unchanged or even decrease
The monitor shows a better blood pressure.
The ventricle may actually be working less efficiently.
Why Some Patients Respond and Others Do Not
The review provides a physiological explanation for the heterogeneity we see every day in the ICU.
Patients with preserved contractile reserve may tolerate increased afterload and maintain efficient coupling.
Patients with septic cardiomyopathy may not.
This may explain why identical norepinephrine doses can produce dramatically different hemodynamic responses among seemingly similar septic shock patients.
Beyond Left Ventricular Function
The same principles apply to the right ventricle.
In septic patients with ARDS:
🔹 Pulmonary vascular resistance rises
🔹 RV afterload increases
🔹 RV-pulmonary artery coupling deteriorates
🔹 Venous congestion develops
🔹 Organ perfusion worsens despite acceptable systemic pressures
This reminds us that shock physiology extends far beyond MAP alone.
Clinical Takeaway
Perhaps the next evolution of septic shock management is not simply asking: "Did cardiovascular efficiency improve?"
Reference 📚
Pinsky MR, Guarracino F. Pathophysiological implications of ventriculoarterial coupling in septic shock. Intensive Care Medicine Experimental. 2023;11:87.
https://t.co/3bYkZ1G7wG
💧Monitoring Fluid Balance – Seeing the Full Picture
Why Daily Weights and Balances Matter
This chapter highlights the limitations of “ins and outs” alone and advocates combining meticulous input/output charting with daily weights and bedside assessment of edema, lung water and organ function. Even modest daily positive balances, when unnoticed, can accumulate to significant tissue edema and ventilator dependence.
From Numbers to Decisions
he authors propose thresholds (e.g. >5% weight gain from baseline) and patterns that should trigger a reassessment of fluids, diuretics or ultrafiltration. They also discuss technical tools—bio‑impedance analysis, transpulmonary thermodilution, ultrasound‑based congestion scores—that refine volume assessment beyond physical exam alone.
📘 All measurement methods and cut‑offs: https://t.co/7pvDxZGOUg
🔵 IFAD 2026 will feature practical sessions on integrating congestion scores and advanced monitoring into ICU rounding.
👉Registration: https://t.co/wATwBWBg5M
#FluidBalance #VolumeStatus #Congestion #ICU
In today's @TheLancet there are 3 papers on cardiometabolic disease: biology, epidemiology, prevention/treatment.
The sobering and all to common story from womb to tomb conveyed in this graphic
https://t.co/rVs2Yz97NC
https://t.co/OpuJTia0bC
https://t.co/i714onXoCG
Benign paroxysmal positional vertigo (BPPV) is an inner ear disorder that causes brief episodes of vertigo.
This JAMA Patient Page describes common symptoms and causes of benign paroxysmal positional vertigo, risk factors, and diagnosis and treatment.
https://t.co/jLSA169OcR



![MarlonVFZR's tweet photo. 🫀⚠️ 𝗙𝗮𝗹𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮́𝗺𝗶𝗰𝗮 𝗲𝗻 𝘀𝗲𝗽𝘀𝗶𝘀: 𝗲𝗹 𝗽𝗿𝗼𝗯𝗹𝗲𝗺𝗮 𝗻𝗼 𝗲𝘀 𝘀𝗼𝗹𝗼 “𝘃𝗮𝘀𝗼𝗱𝗶𝗹𝗮𝘁𝗮𝗰𝗶𝗼́𝗻”, 𝘀𝗶𝗻𝗼 𝘂𝗻𝗮 𝗱𝗶𝘀𝗿𝘂𝗽𝗰𝗶𝗼́𝗻 𝗴𝗹𝗼𝗯𝗮𝗹 𝗱𝗲𝗹 𝗰𝗼𝗻𝘁𝗿𝗼𝗹 𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿, 𝗰𝗮𝗿𝗱𝗶́𝗮𝗰𝗼 𝘆 𝗺𝗶𝗰𝗿𝗼𝗰𝗶𝗿𝗰𝘂𝗹𝗮𝘁𝗼𝗿𝗶𝗼🚨
@ElsevierConnect @sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
En sepsis la inestabilidad hemodinámica surge por la combinación de:
📉 Pérdida del tono vascular
🫀 Alteración de función cardíaca
🧬 Disfunción microcirculatoria y metabólica
👉 Todo esto es un determinante mayor de falla multiorgánica y mortalidad.
🧠 𝙇𝙖 𝙛𝙞𝙨𝙞𝙤𝙥𝙖𝙩𝙤𝙡𝙤𝙜𝙞́𝙖 𝙚𝙨 𝙢𝙪𝙘𝙝𝙤 𝙢𝙖́𝙨 𝙘𝙤𝙢𝙥𝙡𝙚𝙟𝙖 𝙦𝙪𝙚 “𝙛𝙖𝙡𝙩𝙖 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖”
La revisión resume varios mecanismos simultáneos:
✅ Exceso de 𝙤́𝙭𝙞𝙙𝙤 𝙣𝙞́𝙩𝙧𝙞𝙘𝙤 y prostaciclina
✅ Disfunción del 𝙨𝙞𝙨𝙩𝙚𝙢𝙖 𝙣𝙚𝙧𝙫𝙞𝙤𝙨𝙤 𝙖𝙪𝙩𝙤́𝙣𝙤𝙢𝙤
✅ Desensibilización catecolaminérgica
✅ Alteración del 𝙍𝘼𝘼𝙎
✅ 𝘿𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙧𝙚𝙡𝙖𝙩𝙞𝙫𝙖 𝙙𝙚 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖
💧 𝙇𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙩𝙚𝙧𝙖𝙥𝙞𝙖 𝙮𝙖 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙚𝙣𝙩𝙚𝙣𝙙𝙚𝙧𝙨𝙚 𝙘𝙤𝙢𝙤 𝙪𝙣𝙖 𝙢𝙖𝙣𝙞𝙤𝙗𝙧𝙖 𝙖𝙪𝙩𝙤𝙢𝙖́𝙩𝙞𝙘𝙖 𝙣𝙞 𝙪𝙣𝙞𝙛𝙤𝙧𝙢𝙚
Los fluidos siguen siendo fundamentales al inicio, pero su beneficio disminuye rápido fuera de la fase precoz.
Mensajes clave:
📌 La 𝙧𝙚𝙨𝙥𝙪𝙚𝙨𝙩𝙖 𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙨 debe valorarse activamente
📌 No basta con pensar en “respondedor a fluidos”; también importa la 𝙩𝙤𝙡𝙚𝙧𝙖𝙣𝙘𝙞𝙖 𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙨
📌 El exceso de fluidos favorece edema intersticial, disfunción orgánica y peor pronóstico
👉 El enfoque actual es personalizar volumen, velocidad y momento de administración.
💉 𝙀𝙣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨, 𝙡𝙖 𝙩𝙚𝙣𝙙𝙚𝙣𝙘𝙞𝙖 𝙖𝙘𝙩𝙪𝙖𝙡 𝙚𝙨 𝙢𝙚𝙣𝙤𝙨 𝙧𝙚𝙩𝙧𝙖𝙨𝙤 𝙮 𝙢𝙖́𝙨 𝙚𝙨𝙩𝙧𝙖𝙩𝙚𝙜𝙞𝙖 𝙢𝙪𝙡𝙩𝙞𝙢𝙤𝙙𝙖𝙡 𝙥𝙧𝙚𝙘𝙤𝙯
La revisión reafirma a la 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 como vasopresor de primera línea, pero resalta que prolongar o escalar demasiado la monoterapia catecolaminérgica puede asociarse a peor evolución.
Por eso propone pensar antes en:
➕ 𝙑𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖
➕ incluso 𝙖𝙣𝙜𝙞𝙤𝙩𝙚𝙣𝙨𝙞𝙣𝙖 𝙄𝙄 en escenarios seleccionados
Según una lógica de “soporte vasopresor multimodal”.
👉 El objetivo no es solo subir PAM, sino hacerlo con menor toxicidad catecolaminérgica y más racionalidad fisiológica.
📟 𝙀𝙡 𝙢𝙤𝙣𝙞𝙩𝙤𝙧𝙚𝙤 𝙝𝙚𝙢𝙤𝙙𝙞𝙣𝙖́𝙢𝙞𝙘𝙤 𝙪́𝙩𝙞𝙡 𝙣𝙤 𝙚𝙨 𝙚𝙡 𝙦𝙪𝙚 𝙙𝙖 𝙢𝙖́𝙨 𝙣𝙪́𝙢𝙚𝙧𝙤𝙨, 𝙨𝙞𝙣𝙤 𝙚𝙡 𝙦𝙪𝙚 𝙖𝙮𝙪𝙙𝙖 𝙖 𝙙𝙚𝙘𝙞𝙙𝙞𝙧 𝙢𝙚𝙟𝙤𝙧
El review enfatiza que la evaluación debe integrar:
🫀 𝙀𝙘𝙤𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙧𝙖𝙛𝙞́𝙖 𝙘𝙧𝙞́𝙩𝙞𝙘𝙖
📈 Parámetros dinámicos de respuesta a fluidos
🩸 Perfusión periférica, incluyendo 𝙩𝙞𝙚𝙢𝙥𝙤 𝙙𝙚 𝙡𝙡𝙚𝙣𝙖𝙙𝙤 𝙘𝙖𝙥𝙞𝙡𝙖𝙧
🧪 Lactato, pero interpretado con cautela
Además, subraya que no existe un biomarcador único perfecto de perfusión tisular.
👉 La resucitación efectiva sigue siendo multimodal y guiada por fisiología real, no por un solo marcador.
🎯 𝙏𝙖𝙠𝙚-𝙝𝙤𝙢𝙚: 𝙚𝙡 𝙛𝙪𝙩𝙪𝙧𝙤 𝙙𝙚𝙡 𝙨𝙝𝙤𝙘𝙠 𝙨𝙚́𝙥𝙩𝙞𝙘𝙤 𝙚𝙨𝙩𝙖́ 𝙚𝙣 𝙥𝙖𝙨𝙖𝙧 𝙙𝙚 𝙪𝙣𝙖 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙘𝙞𝙤́𝙣 𝙧𝙚𝙖𝙘𝙩𝙞𝙫𝙖 𝙖 𝙪𝙣𝙖 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙘𝙞𝙤́𝙣 𝙥𝙧𝙚𝙙𝙞𝙘𝙩𝙞𝙫𝙖 𝙮 𝙥𝙚𝙧𝙨𝙤𝙣𝙖𝙡𝙞𝙯𝙖𝙙𝙖
El artículo mira hacia adelante con varias líneas potentes:
🤖 Inteligencia artificial para anticipar deterioro hemodinámico
🧬 Biomarcadores más precisos, especialmente del eje 𝙧𝙚𝙣𝙞𝙣𝙖-𝙖𝙣𝙜𝙞𝙤𝙩𝙚𝙣𝙨𝙞𝙣𝙖
⚙️ Estrategias preventivas, no solo reactivas
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/tojooaa9Gy]
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
#Sepsis #SepticShock #Hemodynamics #Vasopressors
#FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HLvd5KNXcAAco89.jpg)
![MarlonVFZR's tweet photo. 🫀⚠️ 𝗙𝗮𝗹𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮́𝗺𝗶𝗰𝗮 𝗲𝗻 𝘀𝗲𝗽𝘀𝗶𝘀: 𝗲𝗹 𝗽𝗿𝗼𝗯𝗹𝗲𝗺𝗮 𝗻𝗼 𝗲𝘀 𝘀𝗼𝗹𝗼 “𝘃𝗮𝘀𝗼𝗱𝗶𝗹𝗮𝘁𝗮𝗰𝗶𝗼́𝗻”, 𝘀𝗶𝗻𝗼 𝘂𝗻𝗮 𝗱𝗶𝘀𝗿𝘂𝗽𝗰𝗶𝗼́𝗻 𝗴𝗹𝗼𝗯𝗮𝗹 𝗱𝗲𝗹 𝗰𝗼𝗻𝘁𝗿𝗼𝗹 𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿, 𝗰𝗮𝗿𝗱𝗶́𝗮𝗰𝗼 𝘆 𝗺𝗶𝗰𝗿𝗼𝗰𝗶𝗿𝗰𝘂𝗹𝗮𝘁𝗼𝗿𝗶𝗼🚨
@ElsevierConnect @sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
En sepsis la inestabilidad hemodinámica surge por la combinación de:
📉 Pérdida del tono vascular
🫀 Alteración de función cardíaca
🧬 Disfunción microcirculatoria y metabólica
👉 Todo esto es un determinante mayor de falla multiorgánica y mortalidad.
🧠 𝙇𝙖 𝙛𝙞𝙨𝙞𝙤𝙥𝙖𝙩𝙤𝙡𝙤𝙜𝙞́𝙖 𝙚𝙨 𝙢𝙪𝙘𝙝𝙤 𝙢𝙖́𝙨 𝙘𝙤𝙢𝙥𝙡𝙚𝙟𝙖 𝙦𝙪𝙚 “𝙛𝙖𝙡𝙩𝙖 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖”
La revisión resume varios mecanismos simultáneos:
✅ Exceso de 𝙤́𝙭𝙞𝙙𝙤 𝙣𝙞́𝙩𝙧𝙞𝙘𝙤 y prostaciclina
✅ Disfunción del 𝙨𝙞𝙨𝙩𝙚𝙢𝙖 𝙣𝙚𝙧𝙫𝙞𝙤𝙨𝙤 𝙖𝙪𝙩𝙤́𝙣𝙤𝙢𝙤
✅ Desensibilización catecolaminérgica
✅ Alteración del 𝙍𝘼𝘼𝙎
✅ 𝘿𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙧𝙚𝙡𝙖𝙩𝙞𝙫𝙖 𝙙𝙚 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖
💧 𝙇𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙩𝙚𝙧𝙖𝙥𝙞𝙖 𝙮𝙖 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙚𝙣𝙩𝙚𝙣𝙙𝙚𝙧𝙨𝙚 𝙘𝙤𝙢𝙤 𝙪𝙣𝙖 𝙢𝙖𝙣𝙞𝙤𝙗𝙧𝙖 𝙖𝙪𝙩𝙤𝙢𝙖́𝙩𝙞𝙘𝙖 𝙣𝙞 𝙪𝙣𝙞𝙛𝙤𝙧𝙢𝙚
Los fluidos siguen siendo fundamentales al inicio, pero su beneficio disminuye rápido fuera de la fase precoz.
Mensajes clave:
📌 La 𝙧𝙚𝙨𝙥𝙪𝙚𝙨𝙩𝙖 𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙨 debe valorarse activamente
📌 No basta con pensar en “respondedor a fluidos”; también importa la 𝙩𝙤𝙡𝙚𝙧𝙖𝙣𝙘𝙞𝙖 𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙨
📌 El exceso de fluidos favorece edema intersticial, disfunción orgánica y peor pronóstico
👉 El enfoque actual es personalizar volumen, velocidad y momento de administración.
💉 𝙀𝙣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨, 𝙡𝙖 𝙩𝙚𝙣𝙙𝙚𝙣𝙘𝙞𝙖 𝙖𝙘𝙩𝙪𝙖𝙡 𝙚𝙨 𝙢𝙚𝙣𝙤𝙨 𝙧𝙚𝙩𝙧𝙖𝙨𝙤 𝙮 𝙢𝙖́𝙨 𝙚𝙨𝙩𝙧𝙖𝙩𝙚𝙜𝙞𝙖 𝙢𝙪𝙡𝙩𝙞𝙢𝙤𝙙𝙖𝙡 𝙥𝙧𝙚𝙘𝙤𝙯
La revisión reafirma a la 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 como vasopresor de primera línea, pero resalta que prolongar o escalar demasiado la monoterapia catecolaminérgica puede asociarse a peor evolución.
Por eso propone pensar antes en:
➕ 𝙑𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖
➕ incluso 𝙖𝙣𝙜𝙞𝙤𝙩𝙚𝙣𝙨𝙞𝙣𝙖 𝙄𝙄 en escenarios seleccionados
Según una lógica de “soporte vasopresor multimodal”.
👉 El objetivo no es solo subir PAM, sino hacerlo con menor toxicidad catecolaminérgica y más racionalidad fisiológica.
📟 𝙀𝙡 𝙢𝙤𝙣𝙞𝙩𝙤𝙧𝙚𝙤 𝙝𝙚𝙢𝙤𝙙𝙞𝙣𝙖́𝙢𝙞𝙘𝙤 𝙪́𝙩𝙞𝙡 𝙣𝙤 𝙚𝙨 𝙚𝙡 𝙦𝙪𝙚 𝙙𝙖 𝙢𝙖́𝙨 𝙣𝙪́𝙢𝙚𝙧𝙤𝙨, 𝙨𝙞𝙣𝙤 𝙚𝙡 𝙦𝙪𝙚 𝙖𝙮𝙪𝙙𝙖 𝙖 𝙙𝙚𝙘𝙞𝙙𝙞𝙧 𝙢𝙚𝙟𝙤𝙧
El review enfatiza que la evaluación debe integrar:
🫀 𝙀𝙘𝙤𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙧𝙖𝙛𝙞́𝙖 𝙘𝙧𝙞́𝙩𝙞𝙘𝙖
📈 Parámetros dinámicos de respuesta a fluidos
🩸 Perfusión periférica, incluyendo 𝙩𝙞𝙚𝙢𝙥𝙤 𝙙𝙚 𝙡𝙡𝙚𝙣𝙖𝙙𝙤 𝙘𝙖𝙥𝙞𝙡𝙖𝙧
🧪 Lactato, pero interpretado con cautela
Además, subraya que no existe un biomarcador único perfecto de perfusión tisular.
👉 La resucitación efectiva sigue siendo multimodal y guiada por fisiología real, no por un solo marcador.
🎯 𝙏𝙖𝙠𝙚-𝙝𝙤𝙢𝙚: 𝙚𝙡 𝙛𝙪𝙩𝙪𝙧𝙤 𝙙𝙚𝙡 𝙨𝙝𝙤𝙘𝙠 𝙨𝙚́𝙥𝙩𝙞𝙘𝙤 𝙚𝙨𝙩𝙖́ 𝙚𝙣 𝙥𝙖𝙨𝙖𝙧 𝙙𝙚 𝙪𝙣𝙖 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙘𝙞𝙤́𝙣 𝙧𝙚𝙖𝙘𝙩𝙞𝙫𝙖 𝙖 𝙪𝙣𝙖 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙘𝙞𝙤́𝙣 𝙥𝙧𝙚𝙙𝙞𝙘𝙩𝙞𝙫𝙖 𝙮 𝙥𝙚𝙧𝙨𝙤𝙣𝙖𝙡𝙞𝙯𝙖𝙙𝙖
El artículo mira hacia adelante con varias líneas potentes:
🤖 Inteligencia artificial para anticipar deterioro hemodinámico
🧬 Biomarcadores más precisos, especialmente del eje 𝙧𝙚𝙣𝙞𝙣𝙖-𝙖𝙣𝙜𝙞𝙤𝙩𝙚𝙣𝙨𝙞𝙣𝙖
⚙️ Estrategias preventivas, no solo reactivas
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/tojooaa9Gy]
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
#Sepsis #SepticShock #Hemodynamics #Vasopressors
#FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HLvd5ItWUAAP0T_.jpg)




























![MarlonVFZR's tweet photo. 🫀⚠️ 𝗙𝗮𝗹𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮́𝗺𝗶𝗰𝗮 𝗲𝗻 𝘀𝗲𝗽𝘀𝗶𝘀: 𝗲𝗹 𝗽𝗿𝗼𝗯𝗹𝗲𝗺𝗮 𝗻𝗼 𝗲𝘀 𝘀𝗼𝗹𝗼 “𝘃𝗮𝘀𝗼𝗱𝗶𝗹𝗮𝘁𝗮𝗰𝗶𝗼́𝗻”, 𝘀𝗶𝗻𝗼 𝘂𝗻𝗮 𝗱𝗶𝘀𝗿𝘂𝗽𝗰𝗶𝗼́𝗻 𝗴𝗹𝗼𝗯𝗮𝗹 𝗱𝗲𝗹 𝗰𝗼𝗻𝘁𝗿𝗼𝗹 𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿, 𝗰𝗮𝗿𝗱𝗶́𝗮𝗰𝗼 𝘆 𝗺𝗶𝗰𝗿𝗼𝗰𝗶𝗿𝗰𝘂𝗹𝗮𝘁𝗼𝗿𝗶𝗼🚨
@ElsevierConnect @sciencedirect
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
En sepsis la inestabilidad hemodinámica surge por la combinación de:
📉 Pérdida del tono vascular
🫀 Alteración de función cardíaca
🧬 Disfunción microcirculatoria y metabólica
👉 Todo esto es un determinante mayor de falla multiorgánica y mortalidad.
🧠 𝙇𝙖 𝙛𝙞𝙨𝙞𝙤𝙥𝙖𝙩𝙤𝙡𝙤𝙜𝙞́𝙖 𝙚𝙨 𝙢𝙪𝙘𝙝𝙤 𝙢𝙖́𝙨 𝙘𝙤𝙢𝙥𝙡𝙚𝙟𝙖 𝙦𝙪𝙚 “𝙛𝙖𝙡𝙩𝙖 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖”
La revisión resume varios mecanismos simultáneos:
✅ Exceso de 𝙤́𝙭𝙞𝙙𝙤 𝙣𝙞́𝙩𝙧𝙞𝙘𝙤 y prostaciclina
✅ Disfunción del 𝙨𝙞𝙨𝙩𝙚𝙢𝙖 𝙣𝙚𝙧𝙫𝙞𝙤𝙨𝙤 𝙖𝙪𝙩𝙤́𝙣𝙤𝙢𝙤
✅ Desensibilización catecolaminérgica
✅ Alteración del 𝙍𝘼𝘼𝙎
✅ 𝘿𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙧𝙚𝙡𝙖𝙩𝙞𝙫𝙖 𝙙𝙚 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖
💧 𝙇𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙩𝙚𝙧𝙖𝙥𝙞𝙖 𝙮𝙖 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙚𝙣𝙩𝙚𝙣𝙙𝙚𝙧𝙨𝙚 𝙘𝙤𝙢𝙤 𝙪𝙣𝙖 𝙢𝙖𝙣𝙞𝙤𝙗𝙧𝙖 𝙖𝙪𝙩𝙤𝙢𝙖́𝙩𝙞𝙘𝙖 𝙣𝙞 𝙪𝙣𝙞𝙛𝙤𝙧𝙢𝙚
Los fluidos siguen siendo fundamentales al inicio, pero su beneficio disminuye rápido fuera de la fase precoz.
Mensajes clave:
📌 La 𝙧𝙚𝙨𝙥𝙪𝙚𝙨𝙩𝙖 𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙨 debe valorarse activamente
📌 No basta con pensar en “respondedor a fluidos”; también importa la 𝙩𝙤𝙡𝙚𝙧𝙖𝙣𝙘𝙞𝙖 𝙖 𝙛𝙡𝙪𝙞𝙙𝙤𝙨
📌 El exceso de fluidos favorece edema intersticial, disfunción orgánica y peor pronóstico
👉 El enfoque actual es personalizar volumen, velocidad y momento de administración.
💉 𝙀𝙣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨, 𝙡𝙖 𝙩𝙚𝙣𝙙𝙚𝙣𝙘𝙞𝙖 𝙖𝙘𝙩𝙪𝙖𝙡 𝙚𝙨 𝙢𝙚𝙣𝙤𝙨 𝙧𝙚𝙩𝙧𝙖𝙨𝙤 𝙮 𝙢𝙖́𝙨 𝙚𝙨𝙩𝙧𝙖𝙩𝙚𝙜𝙞𝙖 𝙢𝙪𝙡𝙩𝙞𝙢𝙤𝙙𝙖𝙡 𝙥𝙧𝙚𝙘𝙤𝙯
La revisión reafirma a la 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 como vasopresor de primera línea, pero resalta que prolongar o escalar demasiado la monoterapia catecolaminérgica puede asociarse a peor evolución.
Por eso propone pensar antes en:
➕ 𝙑𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖
➕ incluso 𝙖𝙣𝙜𝙞𝙤𝙩𝙚𝙣𝙨𝙞𝙣𝙖 𝙄𝙄 en escenarios seleccionados
Según una lógica de “soporte vasopresor multimodal”.
👉 El objetivo no es solo subir PAM, sino hacerlo con menor toxicidad catecolaminérgica y más racionalidad fisiológica.
📟 𝙀𝙡 𝙢𝙤𝙣𝙞𝙩𝙤𝙧𝙚𝙤 𝙝𝙚𝙢𝙤𝙙𝙞𝙣𝙖́𝙢𝙞𝙘𝙤 𝙪́𝙩𝙞𝙡 𝙣𝙤 𝙚𝙨 𝙚𝙡 𝙦𝙪𝙚 𝙙𝙖 𝙢𝙖́𝙨 𝙣𝙪́𝙢𝙚𝙧𝙤𝙨, 𝙨𝙞𝙣𝙤 𝙚𝙡 𝙦𝙪𝙚 𝙖𝙮𝙪𝙙𝙖 𝙖 𝙙𝙚𝙘𝙞𝙙𝙞𝙧 𝙢𝙚𝙟𝙤𝙧
El review enfatiza que la evaluación debe integrar:
🫀 𝙀𝙘𝙤𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙧𝙖𝙛𝙞́𝙖 𝙘𝙧𝙞́𝙩𝙞𝙘𝙖
📈 Parámetros dinámicos de respuesta a fluidos
🩸 Perfusión periférica, incluyendo 𝙩𝙞𝙚𝙢𝙥𝙤 𝙙𝙚 𝙡𝙡𝙚𝙣𝙖𝙙𝙤 𝙘𝙖𝙥𝙞𝙡𝙖𝙧
🧪 Lactato, pero interpretado con cautela
Además, subraya que no existe un biomarcador único perfecto de perfusión tisular.
👉 La resucitación efectiva sigue siendo multimodal y guiada por fisiología real, no por un solo marcador.
🎯 𝙏𝙖𝙠𝙚-𝙝𝙤𝙢𝙚: 𝙚𝙡 𝙛𝙪𝙩𝙪𝙧𝙤 𝙙𝙚𝙡 𝙨𝙝𝙤𝙘𝙠 𝙨𝙚́𝙥𝙩𝙞𝙘𝙤 𝙚𝙨𝙩𝙖́ 𝙚𝙣 𝙥𝙖𝙨𝙖𝙧 𝙙𝙚 𝙪𝙣𝙖 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙘𝙞𝙤́𝙣 𝙧𝙚𝙖𝙘𝙩𝙞𝙫𝙖 𝙖 𝙪𝙣𝙖 𝙧𝙚𝙖𝙣𝙞𝙢𝙖𝙘𝙞𝙤́𝙣 𝙥𝙧𝙚𝙙𝙞𝙘𝙩𝙞𝙫𝙖 𝙮 𝙥𝙚𝙧𝙨𝙤𝙣𝙖𝙡𝙞𝙯𝙖𝙙𝙖
El artículo mira hacia adelante con varias líneas potentes:
🤖 Inteligencia artificial para anticipar deterioro hemodinámico
🧬 Biomarcadores más precisos, especialmente del eje 𝙧𝙚𝙣𝙞𝙣𝙖-𝙖𝙣𝙜𝙞𝙤𝙩𝙚𝙣𝙨𝙞𝙣𝙖
⚙️ Estrategias preventivas, no solo reactivas
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/tojooaa9Gy]
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
#Sepsis #SepticShock #Hemodynamics #Vasopressors
#FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HLvd5KiXUAAVfe6.jpg)