📄 Ischaemia–reperfusion injury: new insights from quantitative CMR
🔗 DOI: https://t.co/2cdu1IuWUa
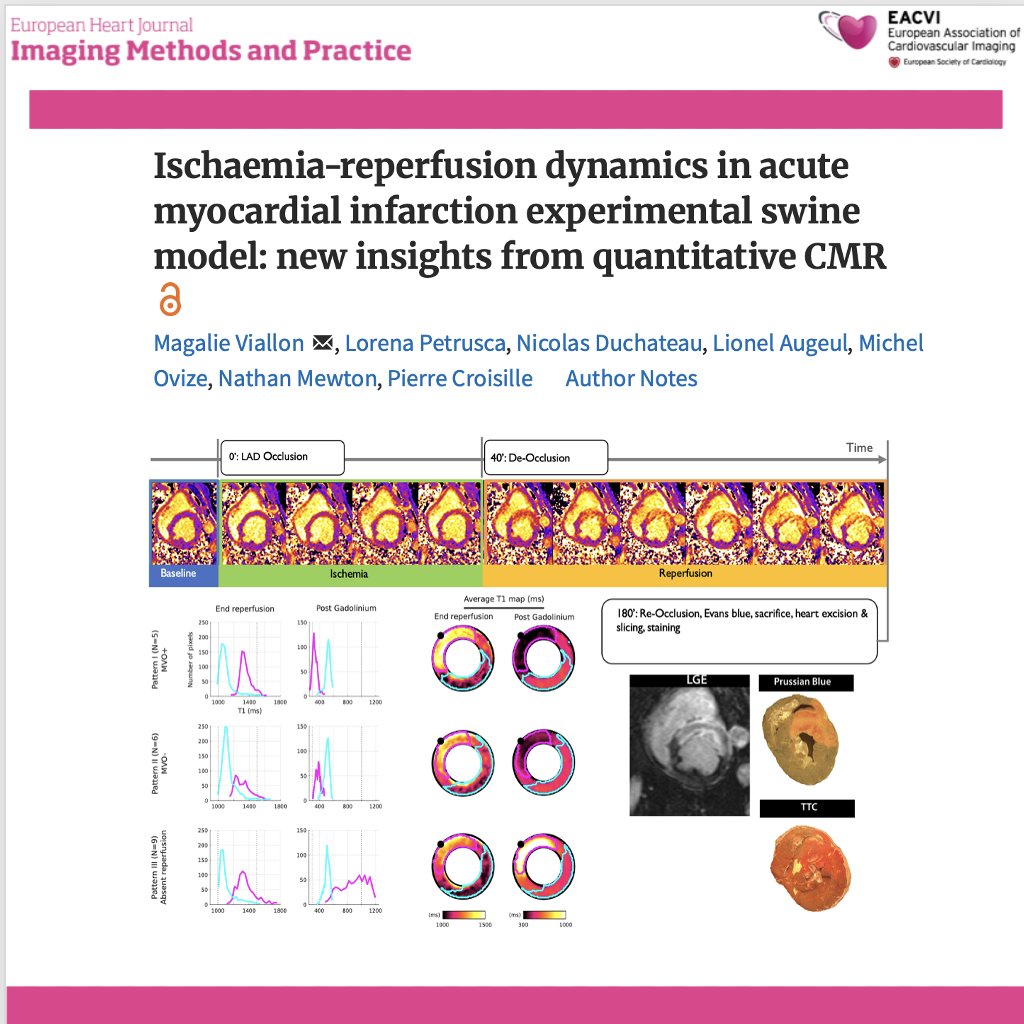
🫀 Reperfusion saves myocardium—but it can also cause additional injury.
This experimental CMR study provides high-resolution, time-resolved insights into what really happens in the myocardium during ischaemia and early reperfusion.
✨ Study design:
🔹 Swine model of acute MI (LAD occlusion → reperfusion)
🔹 Continuous CMR acquisition at:
baseline
during ischaemia
immediately after reperfusion
up to 2–3 hours
🔹 Quantitative T1 & T2 mapping + pixel-wise analysis
✨ Key findings:
📈 During ischaemia:
➡️ Moderate increase in T1 and T2 (+~11%)
👉 reflecting early oedema
📈 After reperfusion:
➡️ Marked increase in T1 and T2 (+~23%)
👉 indicating rapid and significant tissue water accumulation
📊 Critical insight:
👉 The biggest myocardial change happens AFTER reperfusion
➡️ Not during ischaemia
➡️ But immediately after restoring flow
🧠 Three distinct reperfusion patterns identified:
1️⃣ Reperfusion + MVO (microvascular obstruction)
👉 severe injury, largest signal increase
2️⃣ Reperfusion without MVO
👉 less severe but still significant oedema
3️⃣ No effective reperfusion
👉 blunted signal changes
📌 As shown in Figures 2–4 (page 5), each pattern has distinct T1/T2 evolution profiles
⚠️ Key paradigm shift:
👉 Post-reperfusion oedema:
❗ does NOT reflect pre-ischaemic tissue status
❗ does NOT predict final tissue outcome
➡️ Early imaging interpretation may be misleading
🤖 Methodological innovation:
✔ Pixel-wise standardised analysis
✔ Eliminates ROI bias
✔ Enables true spatial and temporal mapping of injury
💡 Clinical implications:
👉 Reperfusion injury is:
dynamic, heterogeneous, and not fully captured by traditional imaging timing
👉 Timing of CMR matters:
➡️ early post-reperfusion scans may reflect transient inflammation, not final infarct size
🚨 Bottom line:
In acute MI, the most dramatic myocardial changes occur after reperfusion—not during ischaemia—and early oedema does not define final injury.
#Cardiology #CMR #MyocardialInfarction #ReperfusionInjury #T1Mapping #T2Mapping #CardiacImaging #PrecisionMedicine #TranslationalResearch 🫀📊
Photon Counting 🔹disminuye la dosis de rayos X🔹duplica /triplica la resolución espacial 🔹menor ruido eléctrico y artefactos 🔹menor dosis de contraste 🔹caracterización de tejido miocárdico & placas arterioscleróticas. Único centro en Madrid @QS_Madrid@CardioQuironMad .
Una experiencia inolvidable . No te la pierdas y veni junto con tu familia & amigos. In programa científico con referentes nacionales e internacionales.
Inscripciones abiertas para el Máster Imagen Cardiaca Avanzada 2026-2027! Consulta toda la información en: https://t.co/k06OZFfoGr
Y reserva ya tu plaza en:
https://t.co/39rTcKdOgU
Repaso del #miniCASO Cardio RM #81 de López Opitz
Transposición de grandes vasos operada con "Switch" arterial y reimplante de coronarias
🔎 https://t.co/v8OBNB26J4 ◀️
Caso completo ⤴️
#aprendeconcasos
🫀👵👴 Septal reduction therapy in elderly patients with obstructive HCM: ASA or myectomy?
A new study from a high-volume HCM center compared alcohol septal ablation (ASA) and transaortic septal myectomy in patients ≥75 years with obstructive hypertrophic cardiomyopathy. Using propensity-matched cohorts (95 vs 95 patients), the authors looked at survival, LVOT gradients, and need for reintervention.
🔍 Key findings:
👉 Procedural risk was low for both strategies (operative mortality 0% with ASA vs 1% with myectomy)
👉 Complete heart block requiring pacemaker was significantly more frequent after ASA (23% vs 10%)
👉 Survival was similar between groups and comparable to an age- and sex-matched general population
👉 LVOT gradient reduction was more complete with myectomy, both early and at late follow-up
👉 Reintervention was more common after ASA (trend toward higher rates)
💡 Take-home message: In elderly patients with obstructive HCM, both ASA and surgical myectomy are safe and effective when performed in experienced centers. Myectomy provides more complete relief of obstruction, while overall early and long-term outcomes remain largely similar, highlighting the importance of individualized, multidisciplinary decision-making.
#HypertrophicCardiomyopathy #HCM #ObstructiveHCM #SeptalMyectomy #AlcoholSeptalAblation #StructuralHeartDisease #ElderlyPatients #CardiacSurgery #InterventionalCardiology #PrecisionMedicine #HeartTeam 🫀🩺📊✨
https://t.co/YTzuNQxZ2J
NUEVO en "García Fernández te pone al día"
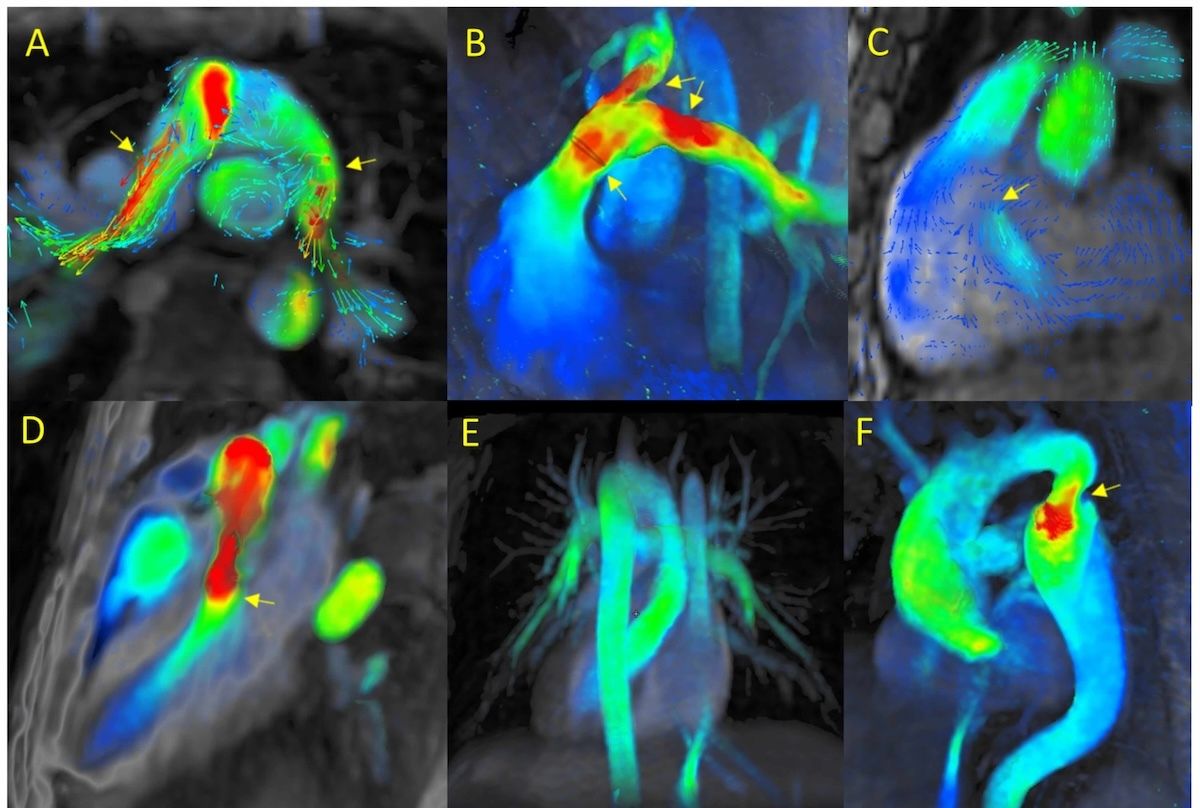
4D-Flow CRM: revisión de la experiencia de 8 años
👓 https://t.co/qH3pD8iGmy ◀️
Los autores superexpertos en el tema nos hacen una detallada revisión de la técnica que merece ser leída por todos los que amamos la imagen
#EHJIMP
🫀 Mitochondrial cardiomyopathy is a cause of #LVH to keep in mind‼️
🫀Cardiac involvement in mitochondrial diseases is common (⅓), including #HCM, conduction disease, #WPW and #DCM. #whyCMR aids in the differential diagnosis!
⏩Read more https://t.co/MA5Wpz1tJj
Shone complex is a rare congenital heart defect characterized by the coexistence of four specific left-sided obstructive lesions of the heart.
● Supra-valvular Ring: A fibrous ring located above the mitral valve.
● Parachute Mitral Valve (MV): A mitral valve with chordae tendineae attaching to a single papillary muscle, resembling a parachute.
● Sub-aortic Stenosis: A narrowing of the left ventricular outflow tract below the aortic valve.
● Coarctation of Aorta: A narrowing of the aorta, the main artery carrying blood from the heart to the body.
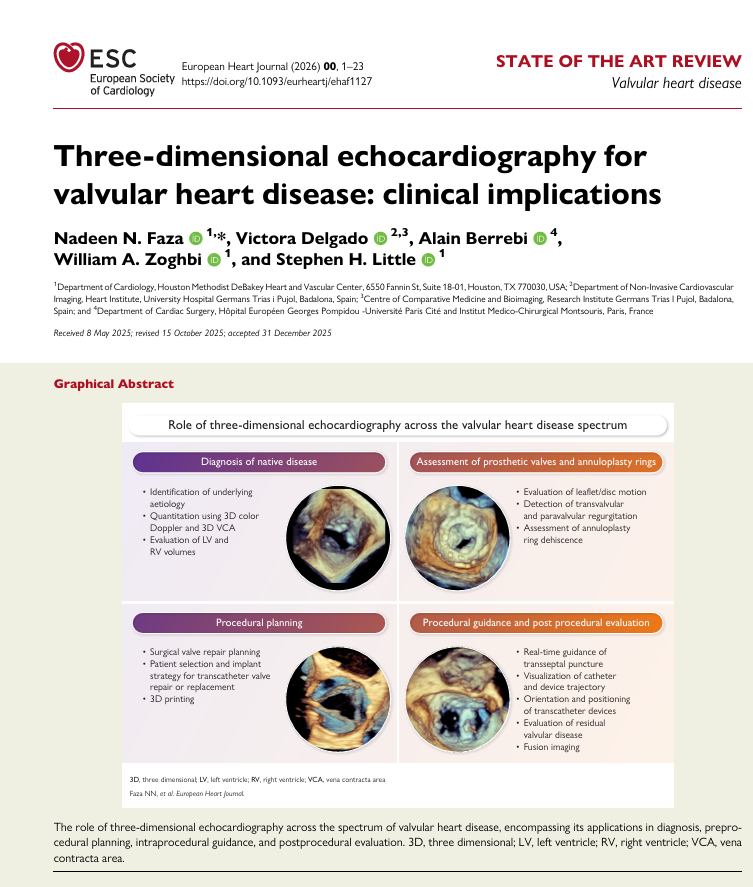
Our #EHJ review highlighting the expanding role of 3D echo in valvular heart disease — from native & prosthetic valve assessment to surgical planning & transcatheter guidance. An honor working with my co-authors on this collaboration.
➡️https://t.co/GwMBVP20bB
#CardioX #Cardiotwitter #Echofirst #3Decho #iecho
Repaso del #miniCASO Eco #201
🔎 https://t.co/Cb1cldij1o ◀️
Paciente de 70 años cursa con ACV isquémico asociado a disnea de 1 mes de evolución
¿Qué vemos en el estudio transesofágico?