Anesthesiologist, OB, ICU. Best parallel parker ever and here for a fun time. Former @MayoClinic @CedarsSinai @WayneMedicine @MichiganStateU Tweets 🚫advice
How do we prevent drug errors? @AmyPearsonMD discusses the tragic examples of intrathecal administration of tranexamic acid
Potential solutions have to consider human factors and system factors and barriers to Implementation #CSAFallConf25
◾️In Memoriam of Robert H. Bartlett, MD 1939-2025
Without Dr. Bartlett, there is no ECMO: he saved more than 100,000 patients through his life’s work. He changed the world.
He will forever be the Father of ECMO.
Vale, Dr B
🔗 https://t.co/RyDvDyXIsw
🎥 https://t.co/Vd4zvjI319
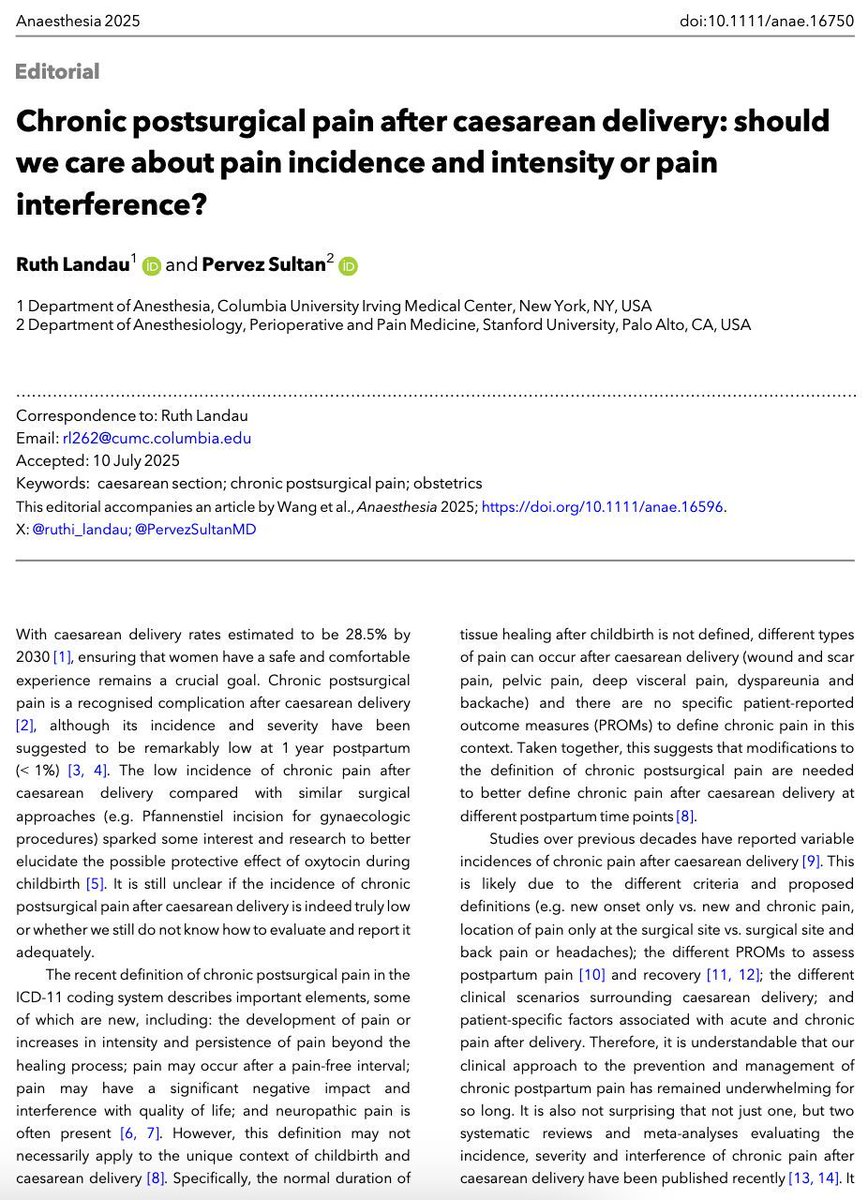
I think how we ask pts about pain during cesarean matters. I’m skeptical of methodology that directly asks about “pain” or “sharp pain.” In Litman et al (https://t.co/rQShzNjoAM) @emilysharpe and I used a VAS scale and didn’t tell pts that 30 mm =pain. #OBAnes
“You should be grateful you had a healthy baby. You should be grateful you survived.”
Tracey Vogel, MD, explains that #trauma can happen despite good medical outcomes, and the reverse is true, too.
#traumahealing#anesthesia#OBAnes#obgyn
Watch now:
https://t.co/aU09ws1nqr
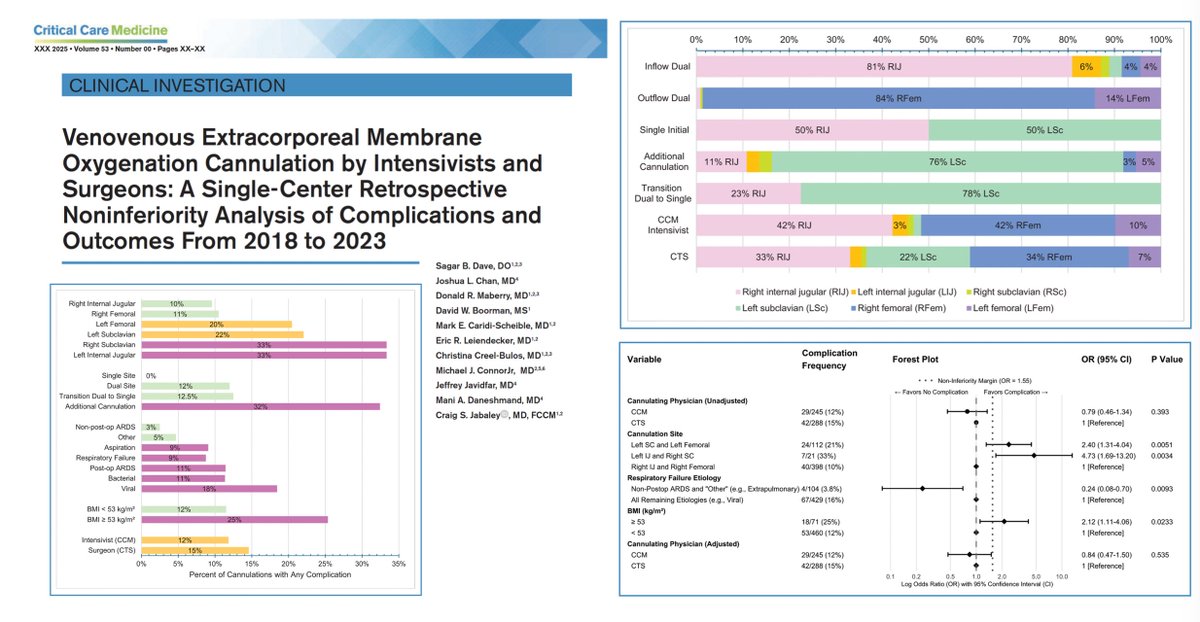
VV #ECMO cannulation by intensivists?
🔍 533 cannulation events (in-center + remote) in established 🇺🇸 #ECLS program
⚖️ cannulation by nonsurgeon noninferior to that by cardiothoracic surgeons with respect to complications
🪦 in-hospital mortality 29%, no significant difference between groups
🚧 complications more common if viral respiratory failure, higher BMI, if cannulation sites other vs RIJV or RFV (2 most commonly used/preferred sites)
Flexible/multidisciplinary model for ECMO delivery are safe! Results reinforce @SCCM & @ELSOOrg guidance + support feasibility of expanding intensivist roles in appropriately structured programs.
@CritCareMed
🖇️ https://t.co/ylLf2Yi5cN
🗓️ Sept 3–4
📍💻 Chicago & Online
The #APSF2025 Stoelting Conference:
“Transforming Maternal Care”
Join us to explore innovations in reducing maternal morbidity & disparities.
Register now: https://t.co/eI2LaXzJig
#Anesthesiology#MaternalHealth#PatientSafety#OBAnes
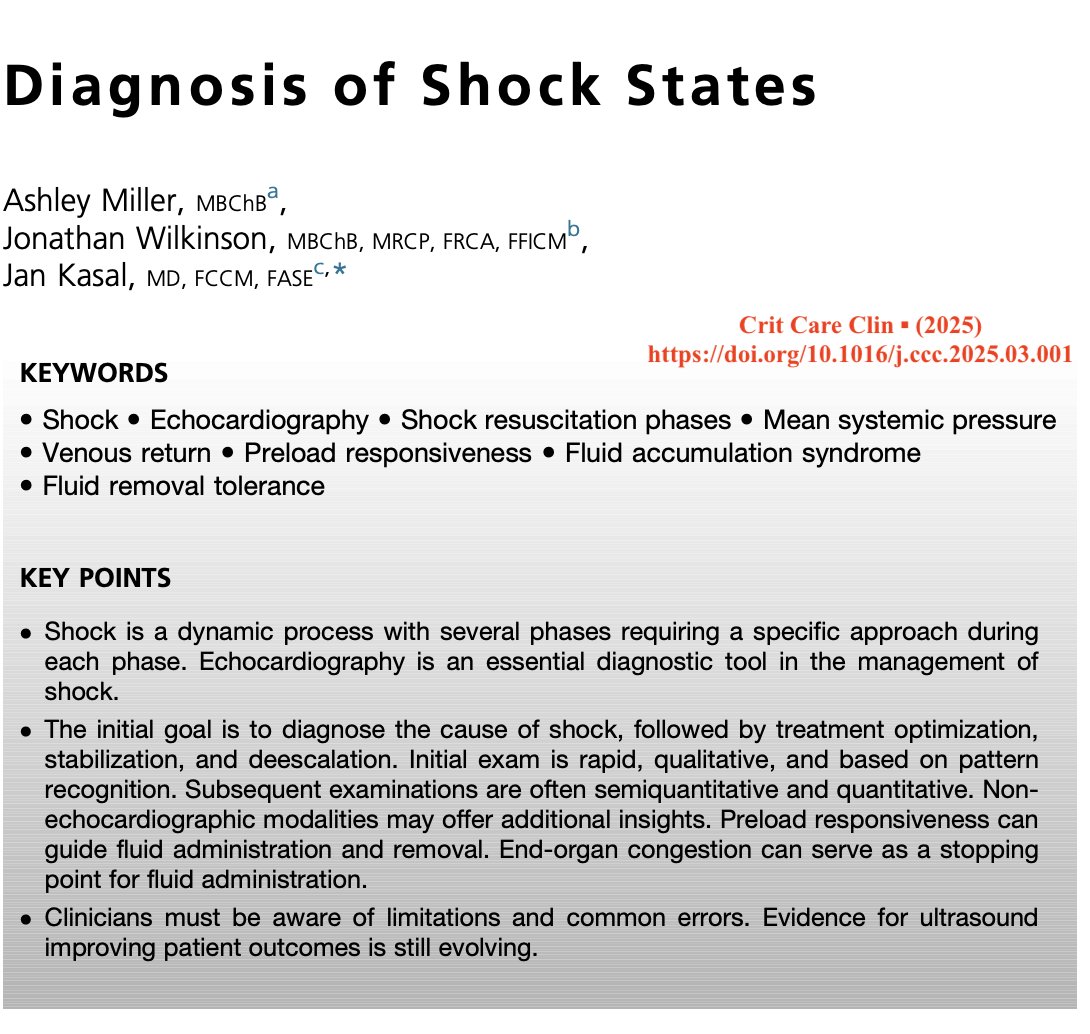
Given that cardiogenic shock tends to carry a higher mortality rate than septic shock, finding strategies to help improve outcomes is worth the effort. A shock team could be helpful to guide the management of these patients. 🎩 tip to the authors.
https://t.co/Sfr6vCn6le
A great review by @icmteaching, @Wilkinsonjonny and Dr Kasal discussing the use of #POCUS in the four phases of shock
BTW, nice blend of (patho-)physiology references & bedside applications!
How common is pain during cesarean under neuraxial? Our review, published in @_Anesthesiology showed it to be v common, overall 17% (95%CI: 13% – 22%. Spinal anesthesia had the lowest pooled incidence of 14% (95%CI: 10% – 20% Epidural top-up highest of 33% (95%CI: 17% - 54%
New research from Stanford’s Dr. Pervez Sultan compares IV treatments for shivering after C-section with neuraxial anesthesia—an issue affecting over half of patients. A systematic review of 20 trials (1,983 patients) ranks the most effective options.
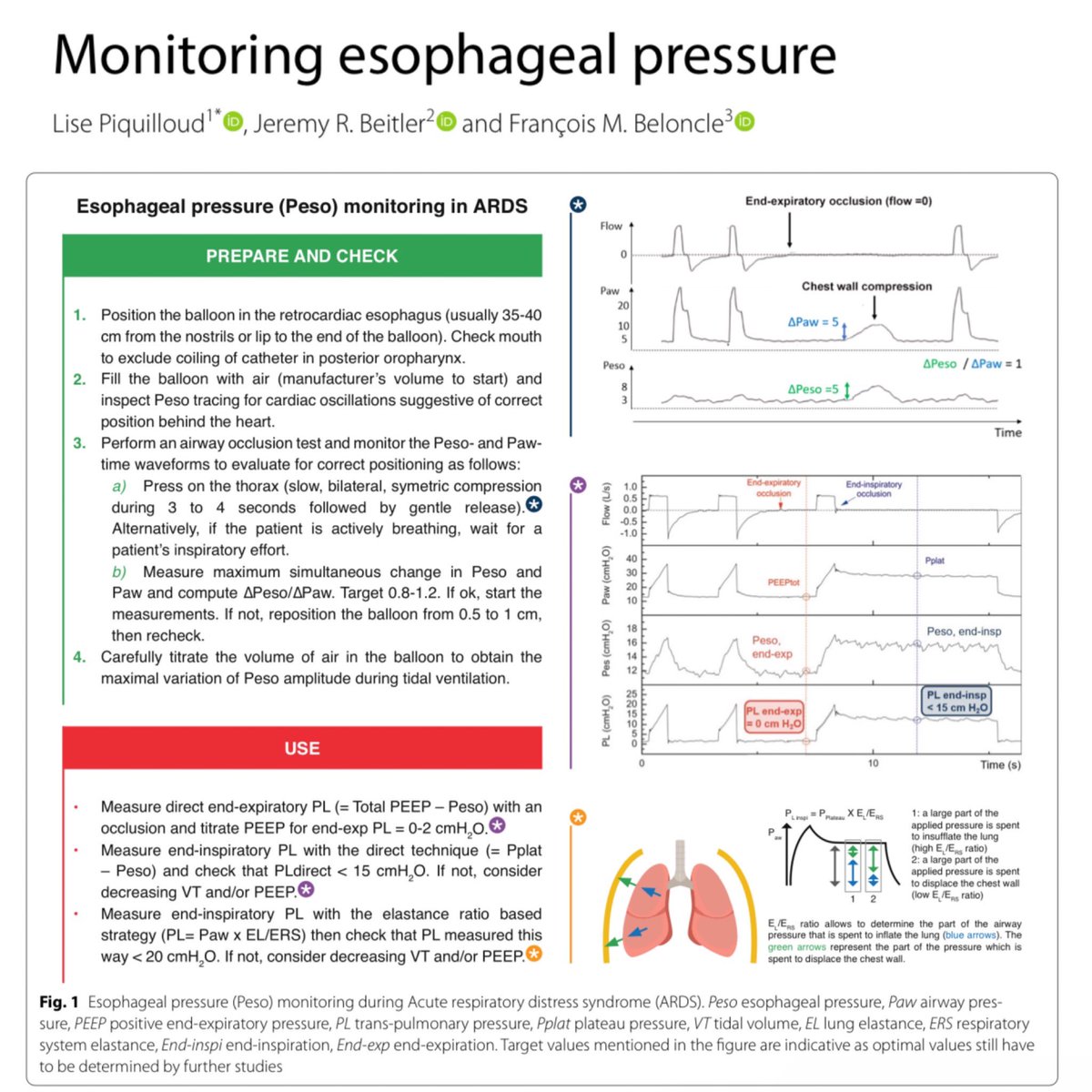
Esophageal manometry is a tool I’ve learned about but have never seen in practice. I welcome thoughts and opinions from those with more experience as to whether this should be routinely used. 🎩 tip to the authors.
https://t.co/4Ise541cSv