@Toad1212@RitikaTuliMD Or you have not captured the highest velocity in whatever view you have obtained like apical 5 chamber or 3 chamber view. Pedoff probe with parasternal view could be helpful
#CardioNuggets
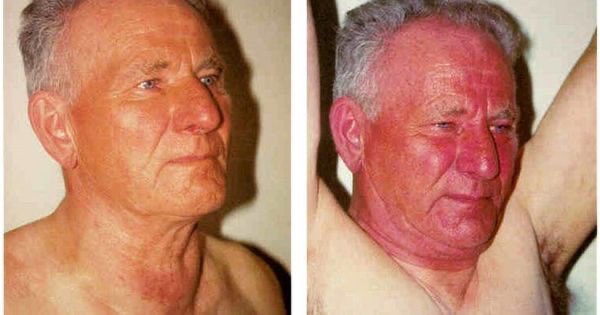
“Teardrop Heart” in Congenital Absence of Pericardium
🫀 Why the “teardrop” shape?
• No pericardial restraint → heart is unusually mobile in the chest
• Leftward displacement → heart shifts toward the left hemithorax
• RV can appear abnormally prominent and findings may mimic those of ASD
✨ Result:
• The LV elongates and stretches downward
• Cardiac silhouette appears narrow superiorly + bulbous inferiorly
#CardioNuggets #MedEd #CardioMed
#acc26 Six reasons why CHAMPION AF should not change oral anticoagulation for AF
I will have a formal post up on @theheartorg but here is a short summary
1) Stroke and Ischemic Stroke went the wrong way.
All S -> 33 vs 50 [HR 1.46 95% CI, 0.94-2.27)]
IS -> 27 vs 45; [HR = 1.61; 95% CI, 1.00-2.59)]
Look at those upper-bounds.
2) NI would not have been met for efficacy had they used a margin with both rate ratio and risk difference, which is standard practice.
The margin of 4.8% is based on event rates at 12%, which is 1.4 in relative terms (40% higher). But when event rates come in lower, as they did: 4.8% vs 5.7%, the 4.8% margin is too lenient.
The 0.9% higher rate of the primary endpoint has a 95% CI of (-0.8-2.6%), so 2.6% is less than the margin of 4.8%. Now do it with relative risk.
It's in table 2. The relative risk is 1.20. The 95% confidence intervals were 0.87-1.66. Note that 1.66> 1.40 so LAAC is not noninferior based on rate ratio margins
3) The primary safety endpoint is flawed because it excludes periprocedural bleeding and uses nonmajor bleeds, such as gum bleeds and bruising. It's open label trial so who which group will complain of more nonmajor bleeding?
4) When counting all events, Watchman barely reduced major bleeds. Also in the main results table is that major bleeds were 83 vs 87 (5.5% vs 5.8%; HR 0.92 95% CI 0.68-1.24)
5) Net Clinical Benefit was also flawed because they used nonprocedural bleeding and nonmajor bleeds.
A normal patient would simply say, there were 17 more strokes and only 4 less bleeds. Hardly a good trade.
6) Bayes: trials don't give answers, they update priors. For Watchman, you have PREVAIL failing against warfarin, CLOSURE AF clearly failing against best med Rx (mostly DOACs) so priors are pessimistic. To go from pessimistic priors to enthusiastic posteriors you'd need hugely positive data. CHAMPION is not that.
Don't believe the stories that CLOSURE failed due to them using other LAAC devices. In the AMULET IDE trial, Watchman and Amulet were similar. Also, if you believe that German operators are worse than US authors, you need to travel more.
Conclusion: Oral anticoagulation for AF is one of the most evidence-based practices in all of medicine. To upend that would take much stronger data.
Don't be bamboozled by this trial, which was designed to be positive before the first patient was enrolled.
#ACC2026
🧵 THREAD: Heart failure kills 50% of patients within 5 years of diagnosis.
But modern GDMT can add 6+ years of life.
Here's the complete evidence hierarchy — ARR, RR, NNT, years gained, combination rankings & ICER ranked best to worst.
#2026 Ideal LDL cholesterol targets in patients with known CVD? National guidelines have increasingly targeted lower LDL cholesterol targets over the years. This trial directly supports this practice, with strong evidence in favor of “Lower is Better”. Ez-PAVE Trial, NEJM 2026 ♥️
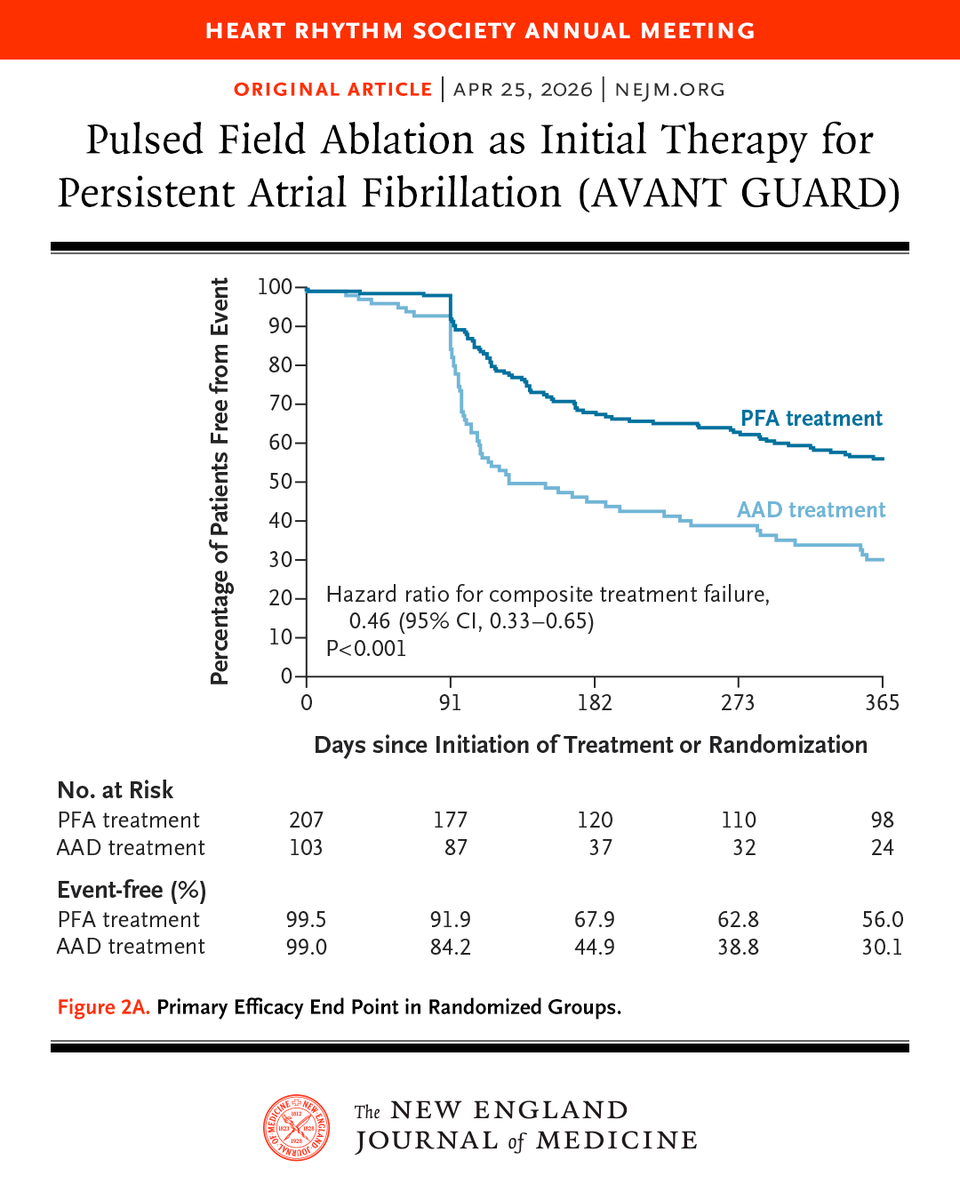
Great thread on the recent NEJM study comparing catheter ablation (PFA) versus antiarrhythmic drugs (AAD) for atrial fibrillation. Never just accept the topline results for big trials. Always drill down on the data like this. The devil is in the details.
Presented at #HRS2026:
In patients with persistent atrial fibrillation, first-line treatment with pulsed field ablation reduced the recurrence of atrial arrhythmias at 12 months as compared with antiarrhythmic drugs. Full AVANT GUARD trial results: https://t.co/milHy26ojJ
@HRSonline
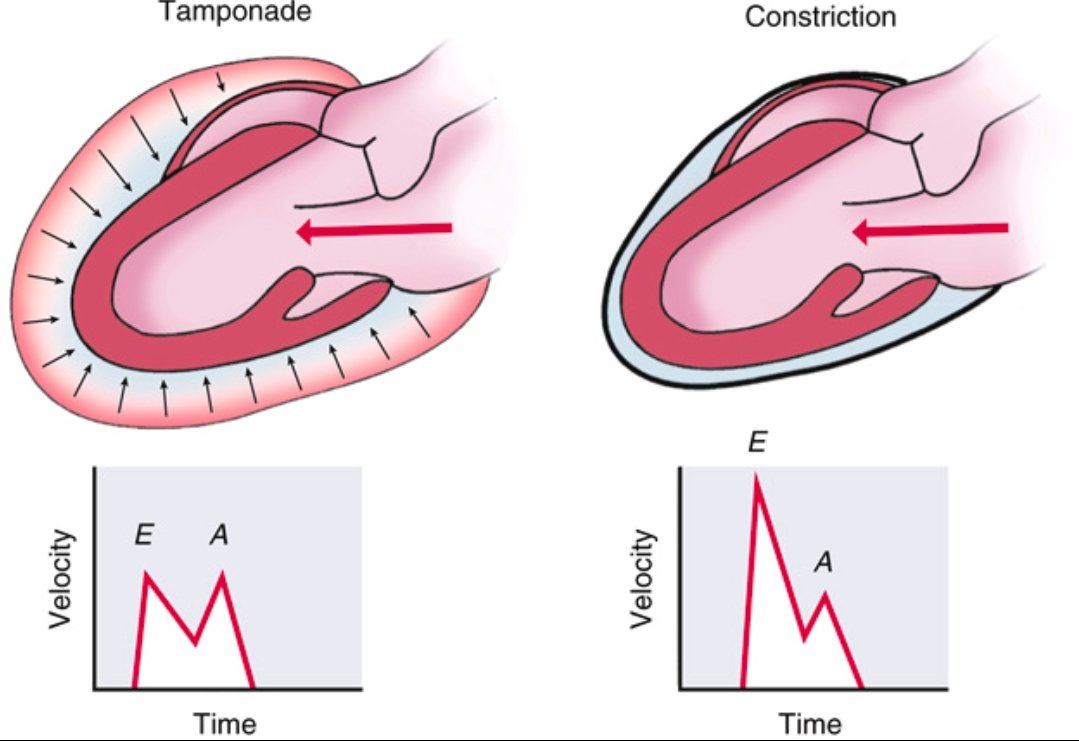
Pericardial Tamponade vs Constrictive Pericarditis ➡️Spot the Difference
Tamponade
⬇️
Accumulation of fluid in the pericardial space
⬇️
↑ intrapericardial pressure
⬇️
impairs diastolic filling throughout the cardiac cycle (early and late diastole).
Doppler shows blunted E and A waves due to restricted filling.
Constrictive Pericarditis
⬇️
Thickened, non-compliant pericardium
⬇️
rapid early diastolic filling that abruptly halts once volume limit is hit.
Doppler shows prominent E wave, reduced A wave, classic for constriction.
Recognizing the echocardiographic filling patterns is essential for diagnosis.
Ref: Catherine M. Otto, Textbook of Clinical Echocardiography
Had an amazing time in NOLA a couple weekends ago for ACC.26! I enjoyed representing @UABCardiology and AL in medical jeopardy, attended some great talks, and best of all, got to spend time with my godson!! 🫀🎉🐣
@ACCinTouch@AlabamaACC@UABCVI