EPSの引き出し、知識を広げたいポンコツCE 。「EP大学」の動画などで大好きなEPSを勉強中です。 日々感謝!あと、バイクはcb223sに乗ってます。 I'm clinical engineer working at japan OSAKA and very interesting in EPS for PSVT.
ECG Breakdown
Clinical scenario:
An 81-year-old woman presents with palpitations.
Step 1: Rhythm
🔺Regular narrow-complex tachycardia.
🔺Ventricular rate approx 160–180 bpm.
🔺QRS complexes are narrow (<120 ms).
This confirms a supraventricular tachycardia (SVT).
Step 2: Look for P waves
🔹No obvious sinus P waves preceding the QRS complexes.
🔹In lead V1, there is a small positive deflection at the terminal portion of the QRS complex (pseudo R′ wave).
This represents retrograde atrial activation.
Step 3: Key diagnostic clue
⚪The arrows in the image below highlight the pseudo R′ waves in V1.
During the tachycardia:
- Pseudo R′ is present.
After spontaneous conversion to sinus rhythm:
- The pseudo R′ disappears.
Normal sinus P waves become visible.
This strongly indicates that the atria are being activated retrogradely from the AV node rather than from the sinus node.
Step 4: Mechanism
Typical AV nodal re-entrant tachycardia (AVNRT):
Atrial impulse travels:
- Antegrade down the slow pathway
- Retrograde up the fast pathway
This creates a re-entry circuit within or near the AV node.
As a result:
◻️ Atria and ventricles are activated almost simultaneously.
◻️Retrograde P waves become buried within the QRS complex.
◻️In V1 they appear as a pseudo R′ wave.
Final Diagnosis:
Typical AV Nodal Re-entrant Tachycardia (AVNRT)
(A form of Paroxysmal Supraventricular Tachycardia, PSVT)
@Paul_Wischmeyer VA ECMO🤔
To prevent ischemia in the leg, a bypass is performed from the ECMO blood supply side to the femoral artery (7fr sheath).
I can see the rSO2 probe on the lower leg.
Induction indices during ventricular pacing as an alternative diagnostic tool in supraventricular tachycardias, by @OsakanogishiM, @MasatoOkada1105, and colleagues
#EPeeps
https://t.co/vJcuhtLzU8
@syamkumarmd Thank you so much. I was wrong🙇🏻
The insertion should be almost simultaneous with the QRS timing.
I understand the timing of the refractory period of HIS to be "late," is that correct?
@syamkumarmd The early PAC insertion immediate hisresets,extending the VA. There is no conventional VA linking. Furthermore, the AA for the two beats surrounding the PAC is not reset, supporting AT. However, there is a possibility of cancellation due to VA decri, so I'll to try other methods.
@Teebi_MD@Amhar_47 VES during tachy(reset+、sequence same)
VAV responce(AT r/o)
PPI-TCL=Approximately 60ms
SA-VA →short
I suspect this is ORT with left bundle branch block (aberrancy), but I'd like to see an evaluation of the HV interval and the response to atrial pacing🤔
@Teebi_MD@Amhar_47 VES during tachy(reset+、sequence same)
VAV responce(AT r/o)
PPI-TCL=Approximately 60ms
SA-VA →short
I suspect this is ORT with left bundle branch block (aberrancy), but I'd like to see an evaluation of the HV interval and the response to atrial pacing🤔
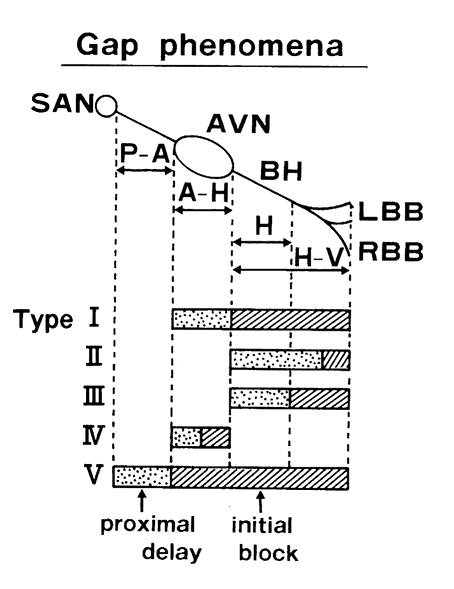
It is indeed the Retrograde Type 2 Gap Phenomenon. His bundle potential seen after the V suggests retrograde RBBB, allowing AV nodal conduction to recover.
@syamkumarmd 270→retro slow(or retro2)+ante fast ventricular responce
260→retro fast return
I suspect that the prolongation of the 「stim-local V 」interval did not shorten the VV interval, and it reverted to going through fast again (GAP phenomenon)🤔