We thank @ACPIMPhysicians for standing up and advocating for the thousands of physicians affected by the USCIS pause.
Since December, US-trained doctors born in 39 designated countries have effectively been blocked from every legal pathway to remain lawfully in the US and continue caring for patients: no visa extensions, no work permits, no green cards, and no path to citizenship, despite doing everything right and giving years of service to the US healthcare system.
These are not new applicants trying to enter the system. They are doctors already here who completed residency and fellowship in the US, are board-certified in their primary specialty, and are already caring for American patients. Many serve in rural and underserved communities, where losing even one physician can be devastating.
After years of training and service, their careers are being brought to a halt for one reason alone: their country of birth. Yet almost no one knows this is happening. Media coverage has been minimal, and organizational advocacy has been scarce.
ACP was among the first to recognize the gravity of this issue. This is not just an immigration matter. It is a patient care crisis unfolding in plain sight.
@ACPIMPhysicians@AmerMedicalAssn@Cardiology@Cardiology@AANmember@AAMCtoday@ProjectImg@ReichlinMelnick
https://t.co/pv3axFpeSy
Encouraging comments from Secretary Mullin. His remarks about the difficulty rural and underserved communities face in recruiting specialists showed a strong understanding of the issue.
This problem extends far beyond one H-1B story. Thousands of physicians from 39 affected countries are already inside the United States and remain subject to USCIS holds that are preventing hospitals from completing hiring, onboarding, or continuation of service. These are physicians whom hospitals recruited, vetted, and signed months, often a year, in advance.
Although a medical physician exemption has been announced, implementation has been slow and inconsistent. With July 1 approaching, many hospitals may face serious staffing disruptions if these cases are not addressed promptly. This is an urgent healthcare access issue, especially for rural and underserved communities that already struggle to recruit specialists. It needs immediate attention.
Secretary Mullin claims that over 200,000 H-1B workers have paid the illegal $100,000 tax on H-1B petitions. That'd be a staggering $20 BILLION in revenue in 6 months! But there's no way it's true. DOJ has said in court filings that H-1B fee revenue is way, way down!
This is only 19. Forget about the 39-country pause. Forget about H1B 100,000, forget about travel bans limiting new hires or incoming physicians from outside the country. We are talking about the ones who were already US-trained and practicing for many years inside the US. US physician unemployment is almost zero. So no one is waiting to take those jobs. It will simply result in disrupted care for millions of Americans. This is an impending workforce crisis hiding in plan sight. We are few weeks away from its full force impact.
Because of delays in waiver processing and the many pause policies affecting thousands of physicians from banned countries, including routine renewals and work permits, many may be forced to leave the U.S. by July.
Once their J-1 status ends on June 30, 2026, those without an approved waiver or H-1B will need to depart the U.S. and pursue H-1B approval through consular processing, adding another barrier to an already prolonged process.
Many hospitals signed thousands of graduating physicians between March and October 2025. After more than a year of planning, this pipeline is now being disrupted at the last minute.
The announced medical physician exemption has moved slowly, leaving the majority of affected physicians stuck in limbo.
To understand the scale, a recent JAMA study found that 24,000 physicians from the initial 19 banned countries alone were active in the U.S. in 2023. That figure does not even account for the expanded list of 39 countries, which includes major feeder countries for U.S.-trained physicians, such as Nigeria, Syria, and Venezuela. Since physicians take an average of 11–15 years to obtain citizenship, anyone along that lengthy pipeline is affected.
When the largest turnover period in medicine and the main hiring cycle begin in July 2026, the impact could be disastrous. Many of these restrictive policies will likely have to be revised to limit disruption to hospital operations and prevent harm to patient care, including delayed clinics and surgeries.
#PhysicianImmigration #IMGPhysicians #J1Waiver #H1BVisa #EADDelays #GreenCardBacklog #DoctorsInLimbo #HealthcareWorkforce #PatientCare #HospitalStaffing #VisaDelays #Residency2026 #UscisPause #MedTwitter #LiftTheHold #LiftThePause
Because of delays in waiver processing and the many pause policies affecting thousands of physicians from banned countries, including routine renewals and work permits, many may be forced to leave the U.S. by July.
Once their J-1 status ends on June 30, 2026, those without an approved waiver or H-1B will need to depart the U.S. and pursue H-1B approval through consular processing, adding another barrier to an already prolonged process.
Many hospitals signed thousands of graduating physicians between March and October 2025. After more than a year of planning, this pipeline is now being disrupted at the last minute.
The announced medical physician exemption has moved slowly, leaving the majority of affected physicians stuck in limbo.
To understand the scale, a recent JAMA study found that 24,000 physicians from the initial 19 banned countries alone were active in the U.S. in 2023. That figure does not even account for the expanded list of 39 countries, which includes major feeder countries for U.S.-trained physicians, such as Nigeria, Syria, and Venezuela. Since physicians take an average of 11–15 years to obtain citizenship, anyone along that lengthy pipeline is affected.
When the largest turnover period in medicine and the main hiring cycle begin in July 2026, the impact could be disastrous. Many of these restrictive policies will likely have to be revised to limit disruption to hospital operations and prevent harm to patient care, including delayed clinics and surgeries.
#PhysicianImmigration #IMGPhysicians #J1Waiver #H1BVisa #EADDelays #GreenCardBacklog #DoctorsInLimbo #HealthcareWorkforce #PatientCare #HospitalStaffing #VisaDelays #Residency2026 #UscisPause #MedTwitter #LiftTheHold #LiftThePause
𝗜𝗺𝗽𝗮𝗰𝘁 𝗼𝗳 𝘃𝗶𝘀𝗮 𝗿𝗲𝘀𝘁𝗿𝗶𝗰𝘁𝗶𝗼𝗻𝘀 𝗮𝗻𝗱 𝘁𝗿𝗮𝘃𝗲𝗹 𝗯𝗮𝗻𝘀 𝗼𝗻 𝗨𝗦 𝗛𝗲𝗮𝗹𝘁𝗵𝗰𝗮𝗿𝗲:
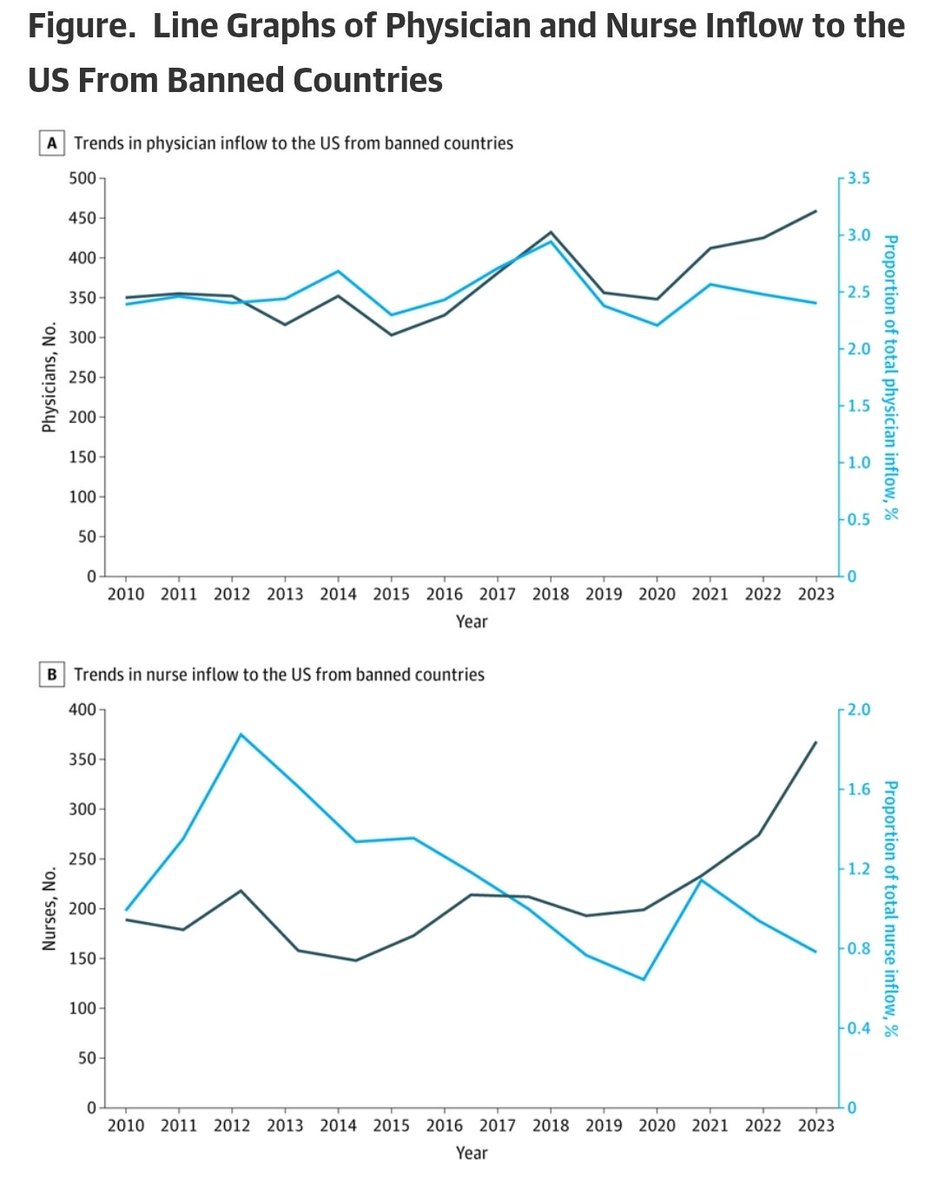
A new study published in JAMA Network Open should serve as a wake up call to policymakers and anyone who believes immigration restrictions have no impact on healthcare.
Researchers found that physicians and nurses from the 19 countries affected by the recent immigration ban make up a significant part of the US healthcare workforce, including nearly 24,000 physicians and more than 56,000 nurses currently practicing across America.
But the most important finding was not just the numbers.
The study showed that these healthcare professionals are disproportionately serving communities that already struggle with physician shortages. Counties with doctors from the affected countries were more than twice as likely to be designated Health Professional Shortage Areas. These communities also tended to have higher proportions of Hispanic and Black residents and lower educational attainment, populations that already face significant healthcare disparities.
For years, International Medical Graduates and immigrant healthcare workers have stepped into areas where physician shortages are most severe. They have staffed rural hospitals, underserved urban neighborhoods, community clinics, nursing homes, emergency departments, addiction treatment centers, and mental health facilities. In many parts of the country, healthcare access would simply not exist at its current level without them.
The debate over immigration often focuses on politics. This study reminds us that there are real world consequences for patients. When barriers are placed in front of qualified physicians and nurses, the people most affected are not politicians or policymakers. They are patients waiting months for appointments, communities struggling to recruit clinicians, and hospitals already operating with critical workforce shortages.
As someone who has worked closely with IMGs and immigrant physicians throughout my career, these findings are not surprising. They simply provide data to support what many of us witness every day: immigrant healthcare professionals are not replacing American healthcare workers, they are filling gaps that would otherwise leave millions of patients without adequate access to care.
Healthcare workforce policy is healthcare policy.
If we are serious about improving access to care, especially in underserved communities, we must recognize the invaluable contributions of immigrant physicians and nurses and ensure that policies do not further weaken an already strained healthcare system.
https://t.co/Uou9a0KeOJ
The latest JAMA study estimates that the original 19 affected countries contributed nearly 24,000 physicians and 56,000 nurses to the U.S. healthcare workforce in 2023, many serving shortage areas.
And that analysis does not even include major physician-source countries such as Nigeria, Venezuela, and Syria that were later swept into related restrictions.
If the physician exemption remains only on paper and is not operationalized before July 1, the consequences will not be abstract. Hospitals, training programs, and patients may feel the impact directly.
#PhysicianWorkforce #HealthcareWorkforce #PatientCare #IMGs #GME #MedTwitter
Immigrants from banned countries contributed nearly 24 000 physicians and 56 000 nurses to the US workforce in 2023, with higher presence in counties with workforce shortages and vulnerable populations.
#ARM26@AcademyHealth
https://t.co/l93CoUXlkX
Immigrants from banned countries contributed nearly 24 000 physicians and 56 000 nurses to the US workforce in 2023, with higher presence in counties with workforce shortages and vulnerable populations.
#ARM26@AcademyHealth
https://t.co/l93CoUXlkX
Important Clarification for the Medical Community:
Some Reported Physician Approvals May Not Reflect Implementation of the Physician Exemption.
The current understanding: Not every physician from a country affected by a travel ban, entry restriction, or visa issuance restriction was subject to the domestic USCIS adjudicative hold. Physicians from countries such as Egypt, Pakistan, India, Brazil, Ethiopia, and others may face entry level (travel or visa-related) restrictions at the border, but their domestic USCIS applications inside the United States generally continued to be processed normally and was never paused.
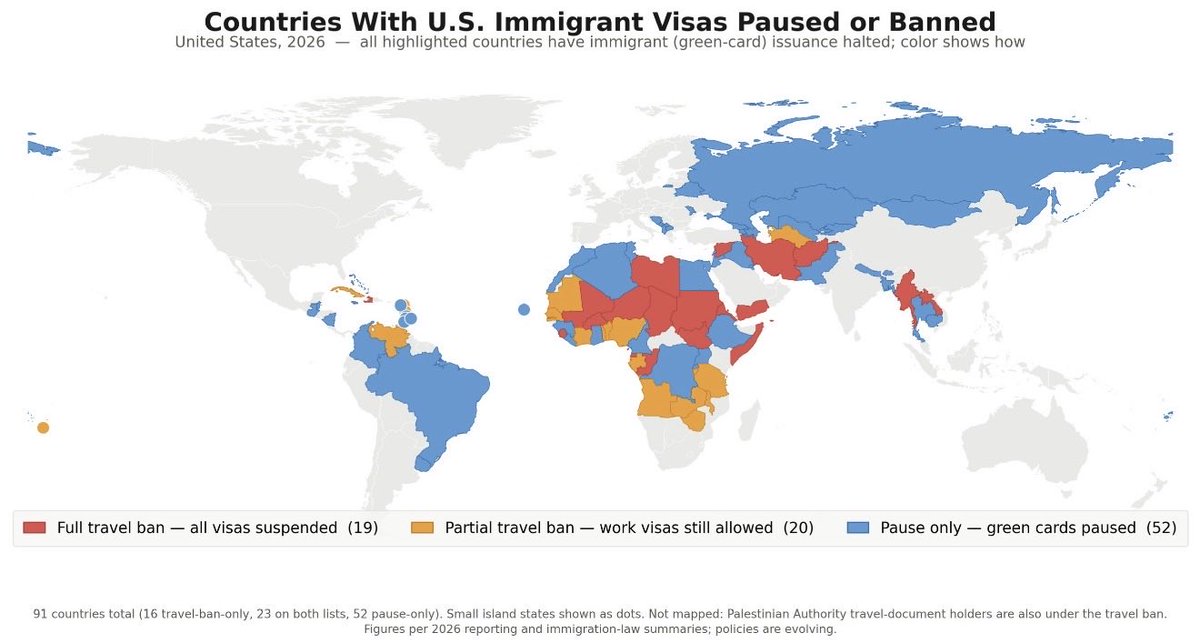
The key question is whether the reported physician approvals after the April 30th physician exemption involve individuals affected by USCIS PM-602-0192 and PM-602-0194, which paused domestic USCIS adjudications for any physician born in or national of the following 39 countries:
Afghanistan, Angola, Antigua and Barbuda, Benin, Burkina Faso, Burma/Myanmar, Burundi, Chad, Côte d’Ivoire, Cuba, Dominica, Equatorial Guinea, Eritrea, Gabon, The Gambia, Haiti, Iran, Laos, Libya, Malawi, Mali, Mauritania, Niger, Nigeria, Republic of the Congo, Senegal, Sierra Leone, Somalia, South Sudan, Sudan, Syria, Tanzania, Togo, Tonga, Turkmenistan, Venezuela, Yemen, Zambia, and Zimbabwe, as well as certain Palestinian Authority travel document holders.
Therefore, when organizations report physician approvals following the announced physician exemption, it is essential to clarify whether those approvals involve physicians from this specific PM-602-0192/PM-602-0194 affected group, or physicians whose domestic USCIS applications were never paused in the first place. Without that distinction, such reports cannot be used as evidence that the physician exemption is being implemented for the physicians it was intended to help.
This distinction is particularly important because a false sense of resolution may obscure the fact that the underlying problem remains unresolved. As July 1 approaches, many incoming and practicing physicians remain at risk of being sidelined if their renewals, extensions, work authorization applications, or employment-related petitions are not adjudicated in time. The resulting disruptions could affect physician staffing, fellowship and residency transitions, hospital recruitment efforts, and ultimately the delivery of patient care.
https://t.co/QjNK87tzeI
https://t.co/ZreItrOBUp
https://t.co/yYRDsrtuWt
#UscisPause #LiftTheHold #PhysicianExemption #IMGs #InternationalMedicalGraduates #PhysicianWorkforce #HealthcareWorkforce #USCIS #ImmigrationPolicy #GraduateMedicalEducation #GME #MedicalResidency #MedicalFellowship #AcademicMedicine #PhysicianAdvocacy
He said all immigration benefits. That is the key point. This is not limited to people outside the United States seeking entry. It also reaches people who were already lawfully admitted, legally living inside the country, and protected by basic constitutional and administrative-law principles.
Section 212(f) is an entry-restriction authority. It is not a blank check to freeze every immigration benefit for people already inside the United States.
Under the policies being applied today, a physician or scientist born in Venezuela or Nigeria, married to a U.S. citizen, legally living and working in the United States for a decade, with an approved extraordinary-ability or national-interest green-card petition, can still be blocked from working, extending legal status, renewing a work permit, receiving a green card, or becoming a citizen, based solely on nationality or place of birth.
No regard for lawful conduct. No regard for years of service, family ties, reliance, taxes paid, contracts signed, or lives built under existing law.
Do you honestly think that makes legal or moral sense?
Congress has not changed the law yet. That is the first problem with your argument.
This is not about whether Congress can regulate future immigration, or whether the President can restrict entry from certain countries under Section 212(f). The people we are discussing were already lawfully admitted, already living legally inside the United States, and had already filed applications under the laws and regulations in effect at the time.
Let’s forget about the INA debate. Even if Congress passed a total immigration restriction today and the President signed it, that law would normally apply prospectively. It would not automatically erase pending applications filed in reliance on existing law, especially where people paid fees, signed contracts, enrolled children in school, accepted jobs, arranged health insurance and made major life decisions based on the legal framework the government itself had in place.
The constitutional issue is not “must all countries be treated equally?” That is a strawman. The issue is whether the government can accept applications and money under one set of rules, then change the rules midstream without meaningful consideration of reliance interests, financial harm, disruption of employment, or humanitarian consequences.
That is not simply an immigration-policy dispute. It is a basic rule-of-law principle and a textbook APA arbitrary-and-capricious problem: the government cannot invite lawful reliance under existing rules, accept applications and fees, then change course midstream and punish people for relying on its own legal framework.
And that is before we even get into other serious issues, such as INA § 202(a)(1)(A), which prohibits discrimination in the issuance of immigrant visas based on race, sex, nationality, place of birth, or place of residence, or the Equal Protection principle that the Supreme Court has repeatedly recognized applies to noncitizens, including lawful permanent residents. But I am not even going there. The narrower point is enough
The majority of impacted physicians are U.S.-trained and board-certified. That means they completed U.S. residency and have often been practicing in the United States for 5–10 years before this pathway ever became an issue.
They are required to complete all USMLE exams, pass in-training exams alongside their U.S. peers, meet the same standards for evaluation and clinical performance, and then pass board exams and, in many cases, multiple subspecialty boards.
If they are “fraud,” then the entire U.S. medical education and training system is a fraud and a diploma mill. That is obviously a ridiculous position.
.