!A physician with Passion for Cardiology #CVimaging#yesCCT#whyCMR#echofirst
“I know that thou canst do all things, and nothing is impossible with thee”
#CTO#PCI skills can help you in a multitude of situations as well!
An older patient (80s) presented with NSTEMI and cardiogenic shock, surgical turndown with trifurcation LM disease and ostial LAD CTO.
Impella support; LAD identified with #HDR and crossed; followed by DK crush into LAD/LCX and sequential kissing for the trifurcation.
I believe that without CTO skills, this patient would likely not make it.
#CardioX #ACCFIT
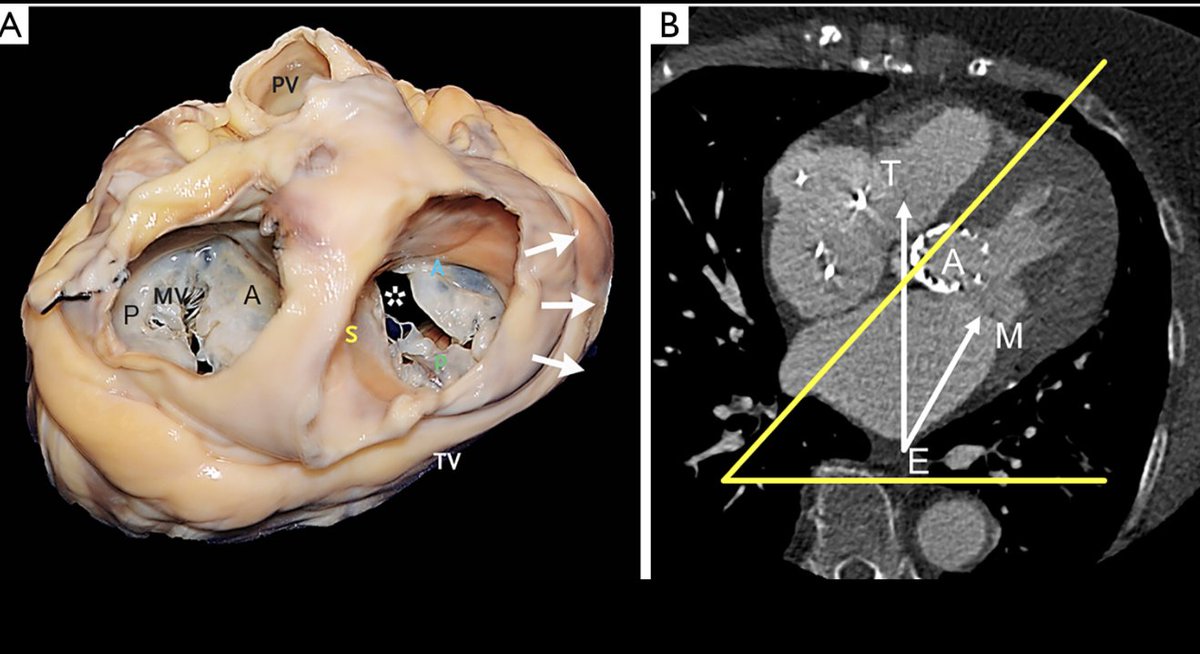
Excited to share our latest work on T-TEER! We break down how to mirror M-TEER workflows for the TV—highlighting key anatomic parallels, imaging strategies, procedural steps to simplify a complex intervention. A practical step-by-step guide
Link -> https://t.co/xcDFbRZzSW
@Hragy Maybe not just post prolapse and there is systolic bowing of anterior leaflet / traction by chordae . Any concern for rheumatic fever ? TEE to check the subvalvular apparatus, papillary muscle displacement etc
Landmark #whyCMR paper on HCM
From @JAMA_current
Among patients with #hypertrophic#cardiomyopathy followed for nearly 7 years, key predictors of adverse outcomes included
1. late gadolinium enhancement (LGE) percentage on #whyCMR,
2. left ventricular (LV) mass index,
3. LV end-systolic volume index,
4. history of heart failure, and
5. log(N-terminal pro–B-type natriuretic peptide [NT-proBNP]).
LGE ≥9% of LV mass was associated with substantially increased risk for the composite of hypertrophic cardiomyopathy–related deaths, ventricular arrhythmias, and transplant or LV assist device implant.
These findings provide prospective evidence for integrating #whyCMR and blood biomarkers in risk assessment for hypertrophic cardiomyopathy. #HCM
https://t.co/idxjF1VGV7
Congratulations Dr. @ChrisKramerMD and others from HCM registry on this terrific paper.
I haven't posted in a while... but here a technique to repair an anterior MV prolapse with transfer of P2 segment, and patch repair of P2. A technique I have learned from Prof. El Khoury. This is open for discussion. More to come;) @GebrineK
@SVRaoMD@benhibbertMDPhD@TCTMD Great points 👍🏼 With very low event rates on DOACs, even a slightly worse therapy can pass) Margin selection can artificially favor LAAO.
Should we accept clinically meaningful excess stroke risk to gain less bleeding?
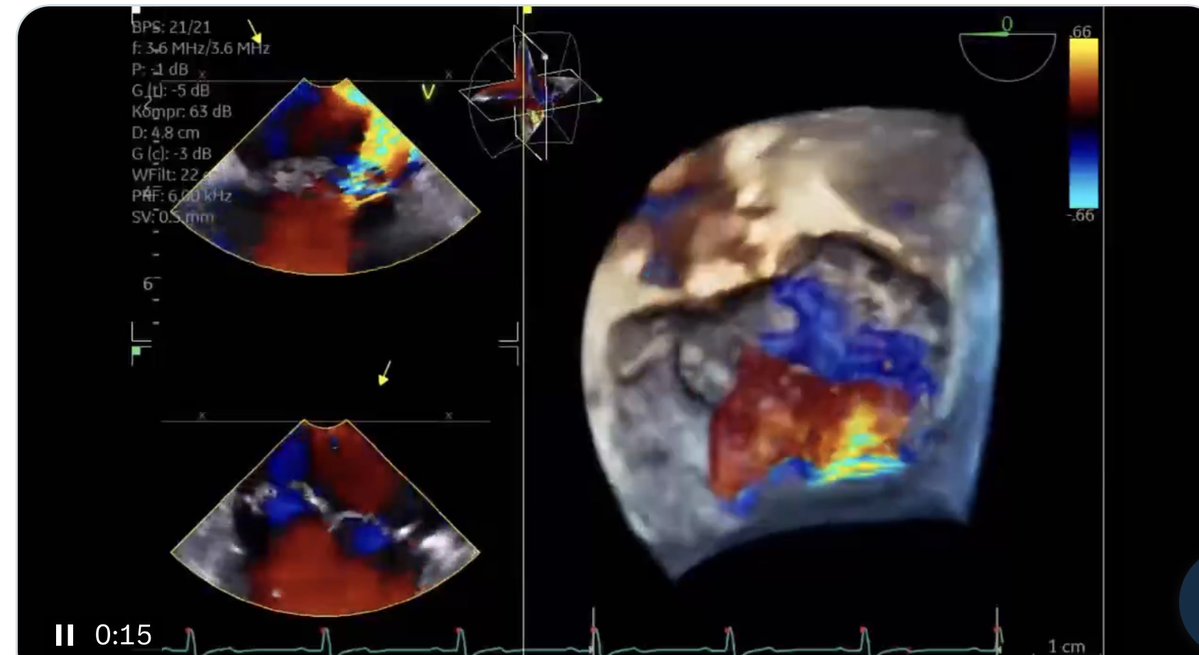
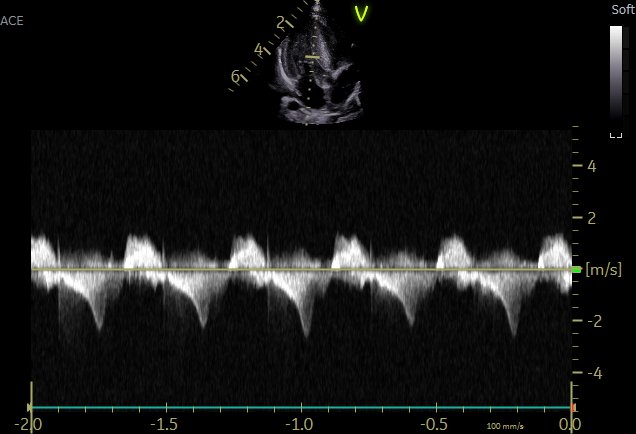
Teaching case/decision making
👉 M. 69 yo with severe AS scheduled for SAVR
📍preop TTE
📍intraop TEE (pre-CPB)
📍no pt’s informed consent about MV surgery
Intraop TEE done by a fellow
How would you proceed #echofirst@iamritu@NMerke@CASivaram1@DrRajeshG1@OungSavly

























![purviparwani's tweet photo. Landmark #whyCMR paper on HCM
From @JAMA_current
Among patients with #hypertrophic #cardiomyopathy followed for nearly 7 years, key predictors of adverse outcomes included
1. late gadolinium enhancement (LGE) percentage on #whyCMR,
2. left ventricular (LV) mass index,
3. LV end-systolic volume index,
4. history of heart failure, and
5. log(N-terminal pro–B-type natriuretic peptide [NT-proBNP]).
LGE ≥9% of LV mass was associated with substantially increased risk for the composite of hypertrophic cardiomyopathy–related deaths, ventricular arrhythmias, and transplant or LV assist device implant.
These findings provide prospective evidence for integrating #whyCMR and blood biomarkers in risk assessment for hypertrophic cardiomyopathy. #HCM
https://t.co/idxjF1VGV7
Congratulations Dr. @ChrisKramerMD and others from HCM registry on this terrific paper.](https://pbs.twimg.com/media/HILQWWibMAAxPh7.jpg)