🚨 NEW #PlatinumOpinion in European Urology by M. J. Roberts, @GGandaglia et al :
💡 Is extended pelvic lymph node dissection (ePLND) still justified in prostate cancer?
📉 No oncologic benefit in RCTs
⚠️ Up to 20% complication rate
🧬 PSMA PET reshapes staging
🔄 2024 EAU Guidelines update: reconsider routine ePLND.
🔗 https://t.co/XFczocASmF
#EAUGuidelines #ProstateCancer #UroOncology #ePLND #PSMAPET #urotwitter
📢Publication alert!
Highlights:
1⃣Across 11 trials, TMT was associated with lower OS and CSS than RC
2⃣RC should remain the standard of care for nonmetastatic MIBC
3⃣TMT remains a valid alternative for carefully selected and informed patients
🔗https://t.co/EERejp5J6l
Real-world outcomes for high-risk non-muscle-invasive #BladderCancer: screened patients for the BRAVO trial
@S_Conroy91@JimCatto
https://t.co/iGlTvitSyk
Influence of a surgeon’s exposure to operating room turnover delays on patient outcomes
➡️https://t.co/Y0WLcHT3SZ
In this prospective study, a 3.3% (95% c.i. 0.6% to 5.6%) increase in the rate of major adverse events was observed when a surgeon experienced a delay in operating room scheduling or waiting time between two procedures exceeding 1 h. Optimizing operating room turnover to prevent delayed operations and waiting time is critical for patient safety.
👏👏👏Arnaud Pasquer, Quentin Cordier, Jean-Christophe Lifante, Gilles Poncet, Stéphanie Polazzi, Antoine Duclos
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @me4_so@BJSAcademy@BJSurgery@young_bjs@juliomayol@JJEarnshaw @OUPMedicine
Digital Rectal Examination Is Not a Useful Screening Test for Prostate Cancer - finally out. Early results from the PROBASE screening trial in younger men. Great team effort! https://t.co/xwLQu5eWui
@Issarami Totally agree, but all the headaches saved in the immediate post-operative recovery are often paid back on the mid-/long-term with multiple readmissions for dislodged stents, recurrent UTIs, stoma stenosis. Not to forget the need of keeping these patients on regular stent change.
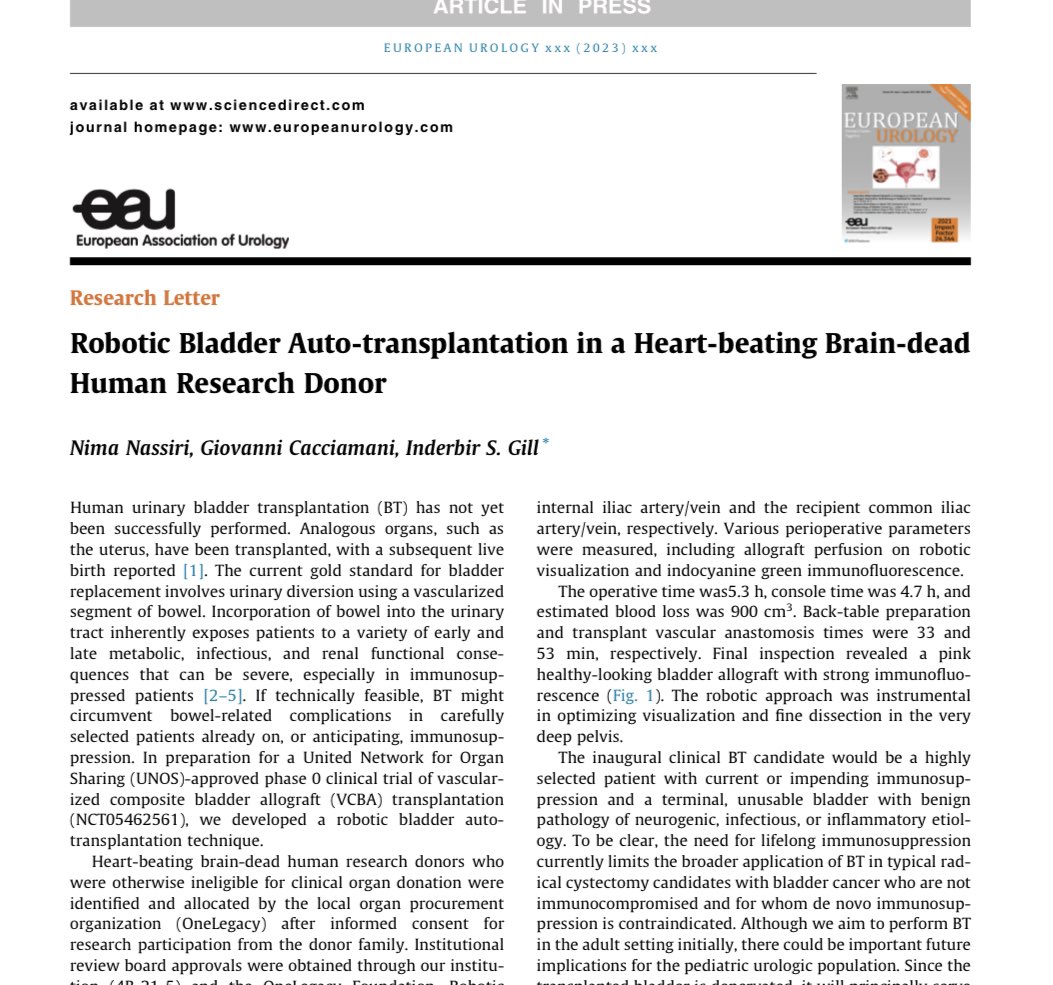
💡This is the first report of vascularized #BladderTransplantation in a heart-beating, brain-dead human donor, with excellent vascular viability after reperfusion, and is a necessary #preclinical step before a first-in-human BT.
✅If clinically successful, BT could offer a bowel-free, more normal bladder substitute in selected patients with bladder failure.
https://t.co/ZZXfmoblRX
@uro_nima@USC_Urology@EUplatinum@Uroweb@AmerUrological
If you are looking to train in robotic prostate surgery and bladder cancer surgery in a high volume pelvic cancer unit with a strong focus on education @SNathanUK@Jkurol@greglshaw@4urology @ZaferTandogdu @lambwben@KelkarUro @UroSplice @veerukasi https://t.co/onYr6CKD5N
Proud that the service we offer at @MSEHospitals has been publicised in the local newspaper. Gaining local awareness is important, so patients know that top class treatments can be delivered at their doorstep.
Thanks to my hardworking #team for the support.
#urology#essex
4⃣ A surgeon based at Southend Hospital has become the first in the East of England to carry out a rare operation using a pioneering robotic device - By @Sophie_England_
https://t.co/ezemMIqbam
@Issarami@doculla@Uroweb@nairajesh@acesridhar Also, operating times in experienced surgeon are comparable in both approaches. So, yes, when the patient can go for either RARC or ORC, I do counsel about advantages of RARC 😂
@Issarami@doculla@Uroweb@nairajesh@acesridhar Unless patient/cancer characteristics do not allow a safe🤖 approach, RARC is first option IMHO. RAZOR, iROC don’t show any disadvantage for robotic vs open and rather quicker recovery and less DVT/PE or wound complications. Even cost has been shown to be not an issue anymore.
It is this time of the year again: TOP 10 GU Oncology clinical papers/trials in 2022:
Some negative, some positive, but we learned from all!
Feel free to add more & retweet & tag anyone involved
This is not an exhaustive list!
@OncoAlert@danafarber#OnwardFor2023