🌞 Malar Rash: Beyond Lupus
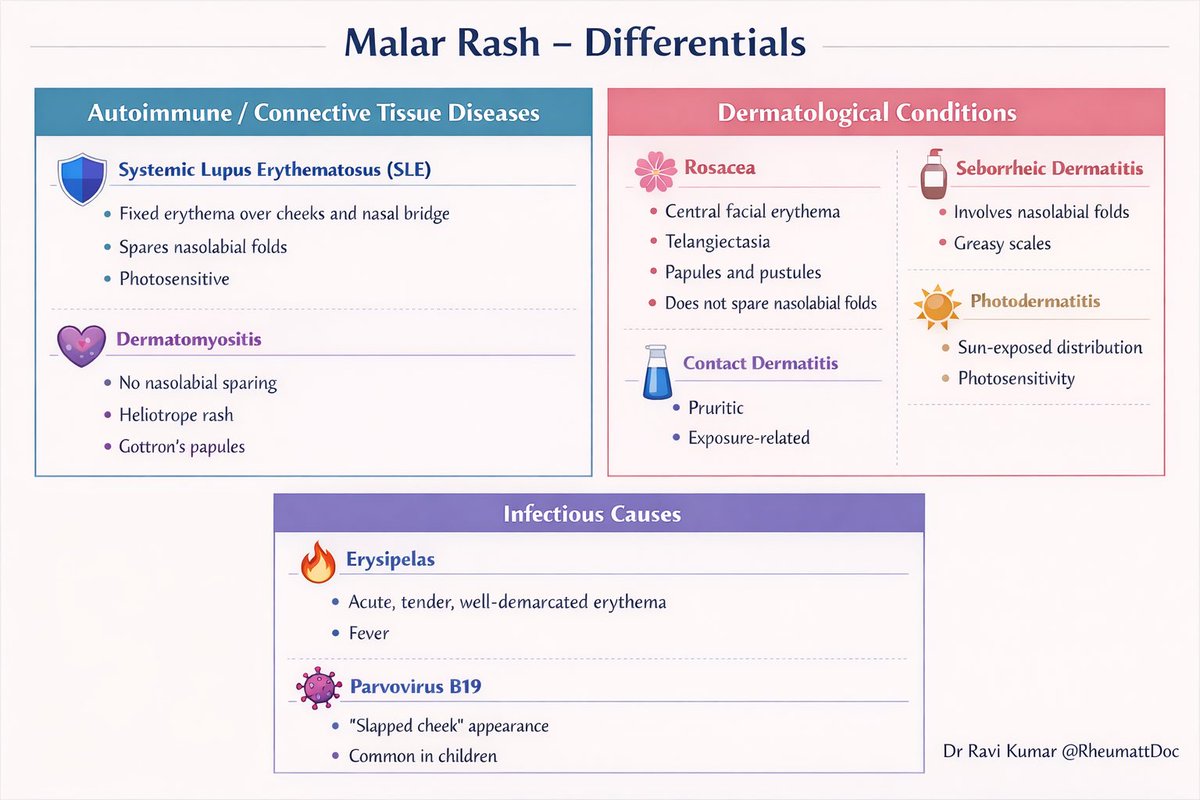
A malar rash is an erythematous rash over the cheeks and bridge of the nose, classically resembling a butterfly.
Not every malar rash is lupus
Here are a few differentials of malar rash👇👇
🧠 Rheumatological Conditions
🛡️ Systemic Lupus Erythematosus (SLE)
•Fixed erythema over cheeks and nasal bridge
•Spares nasolabial folds
•Photosensitive
💜 Dermatomyositis
•Does NOT spare nasolabial folds
•Heliotrope rash
•Gottron’s papules
•Proximal muscle weakness
🌿 Dermatological Conditions
🌸 Rosacea
•Central facial erythema
•Telangiectasia
•Papules and pustules
•Does not spare nasolabial folds
🧴 Seborrheic Dermatitis
•Prominent involvement of nasolabial folds
•Greasy yellow scales
☀️ Photodermatitis
•Sun-exposed distribution
•Clear photosensitivity history
🧪 Contact Dermatitis
•Pruritic eruption
•Exposure related
🦠 Infectious Causes
🔥 Erysipelas
•Acute onset
•Tender, well-demarcated erythema
•Fever and systemic symptoms
🧫 Parvovirus B19
•“Slapped cheek” appearance
•More common in children
•Often associated with viral prodrome
#RheumattDoc #MedTwitter #RheumTwitter #Medicine #rheumatology @DrAkhilX @IhabFathiSulima@CelestinoGutirr@DurgaPrasannaM1
Treat to target in Osteoporosis:
- Pts with T score < -2.5, target to > -2.5 or higher if fracture.
-Pts with T score > -2.5 increase total hip score by (0.2) 3% and LS 0.5 (6%)
#RWCS2026@RheumNow
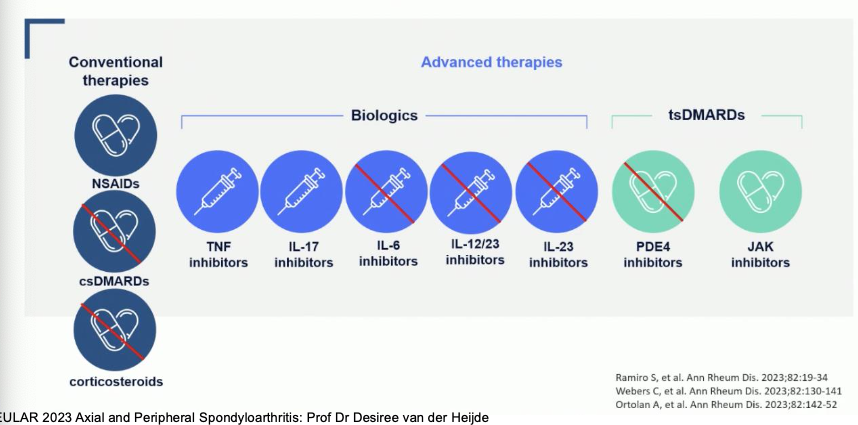
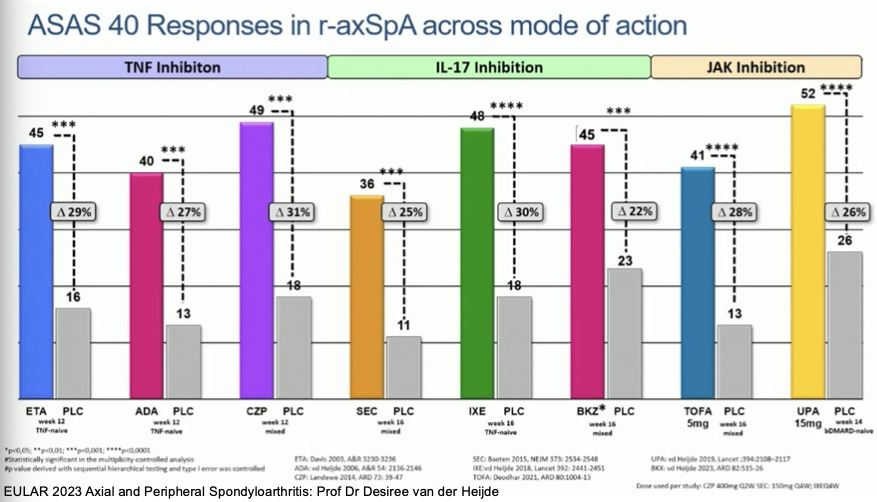
Blakewell: There is not one agent that is superior between TNF, IL-17, JAKi
Patient characteristics and manifestations can help make decision
Some meds clearly shown to be not helpful
@RheumNow#RNL26
🩺 Kikuchi Disease
A rare, benign, self-limiting inflammatory disease causing tender cervical lymphadenopathy, most often in young women. Frequently mistaken for tuberculosis, lymphoma, or SLE.
🧬 Pathogenesis
•Likely immune-mediated, often post-viral
•Prominent CD8⁺ T-cell–mediated apoptosis
•Necrosis without neutrophils
🩺 Clinical Features
•🌡️ Low- to high-grade fever
•🦠 Painful cervical lymph nodes (posterior > anterior)
•😴 Fatigue, malaise
•🧴 Rash (occasionally)
•🤕 Arthralgia (less common)
Usually no weight loss or night sweats (helps distinguish from lymphoma/TB)
🧪 Laboratory Findings
•🔻 Leukopenia (common)
•📈 ESR / CRP mildly elevated
•🧬 ANA: usually negative, but may be transiently positive
•⚠️ Important: monitor for future SLE
🔬 Lymph Node Biopsy (Diagnostic)
Hallmark features
•Patchy necrosis
•Abundant karyorrhectic debris
•Histiocytes & plasmacytoid dendritic cells
•❌ No neutrophils or plasma cells
➡️ This differentiates it from SLE lymphadenitis and infections.
🧠 Differential Diagnosis
•Tuberculous lymphadenitis
•Lymphoma
•SLE lymphadenitis
•Viral infections (EBV, CMV)
💊 Treatment
🟢 Supportive care only in most cases
•NSAIDs, antipyretics
🔵 Short course corticosteroids
•Severe pain, persistent fever, or extranodal disease
•❌ No antibiotics or ATT unless another diagnosis confirmed
⏳ Prognosis
•Excellent 🌟
•Resolves in 1–4 months
•🔁 Recurrence: ~3–5%
•🔍 Small but real association with future SLE → follow-up advised
#RheumattDoc #MedTwitter #RheumTwitter #Medicine #rheumatology @DrAkhilX @IhabFathiSulima@CelestinoGutirr@DurgaPrasannaM1
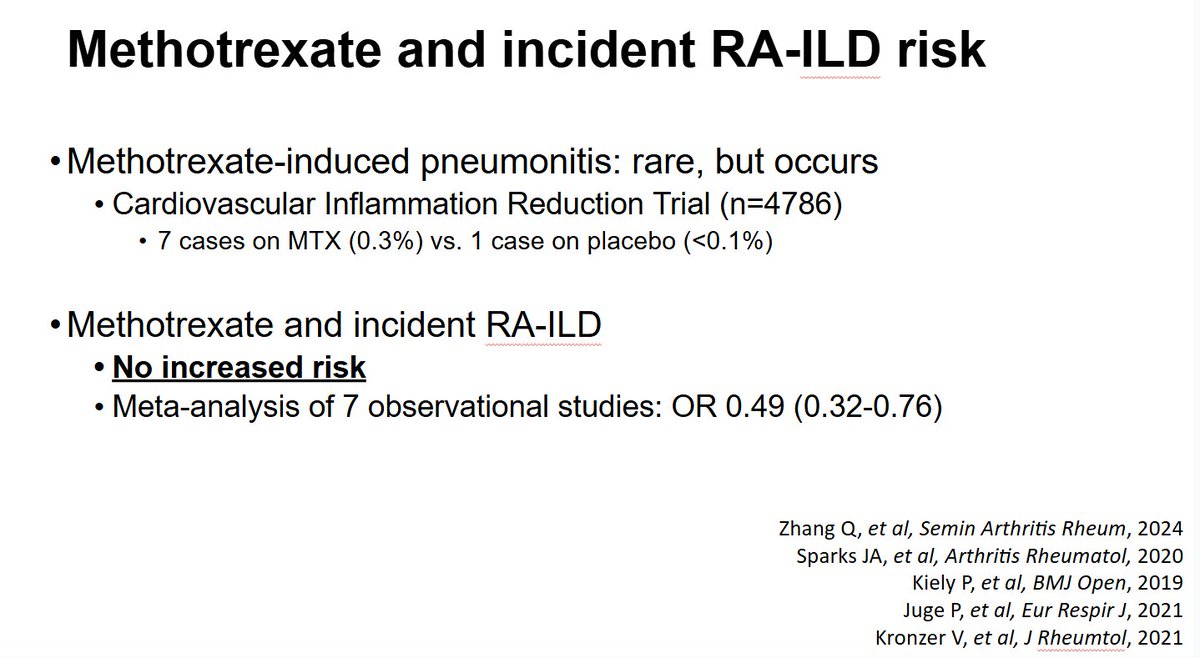
I long for the day when we no longer have to say that MTX does not cause RA-ILD. Another meta-analysis showing no increased risk, in fact a 51% decreased risk with MTX! #RNL26@RheumNow
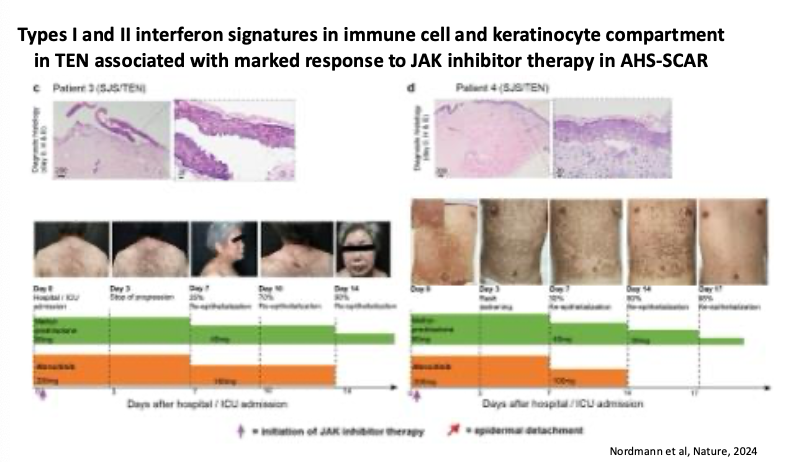
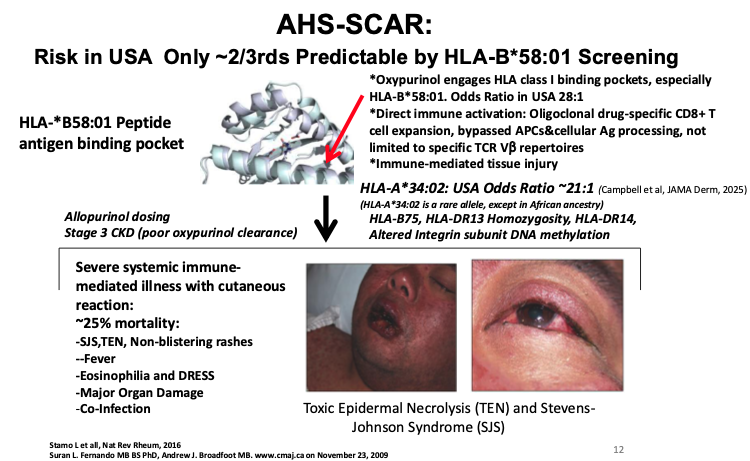
Can you predict Allopurinol Hypersensitivity (AHS-SCAR) with HLA screening?
#RNL26@RheumNow
Not completely - only 2/3 predictable by HLA-B*58:01 screening
Others like HLA-A*34:02 also associated, but unable to commercially test for
Treatment: Marked response to JAK inhibitor Rx
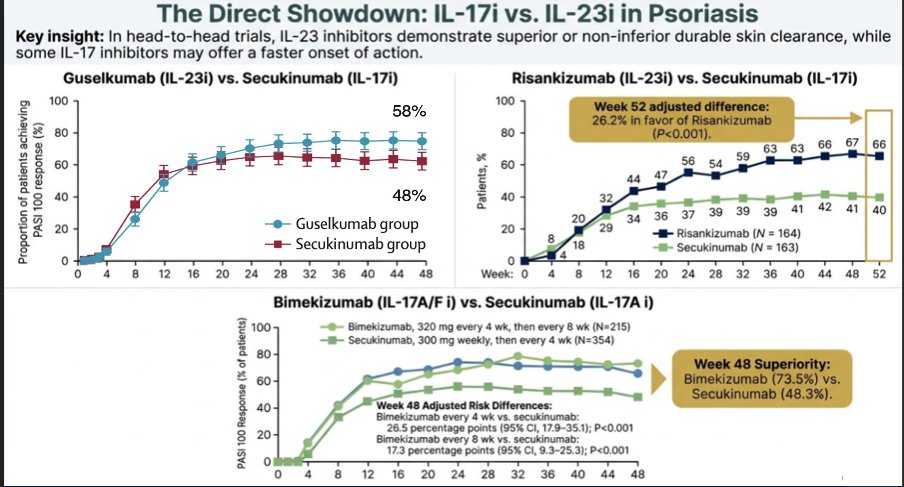
Super Bowl Battle:
IL17 vs IL 23 in PsA?
#RNL26@RheumNow Andre Riberio
Severe skin:
IL17 & IL23 both show superiority over TNFi for plaque PsO
IL17 quicker, IL23 show superior or non-inferiority skin
Bimiekizumab (IL-17A/F superior to other IL17)
IL-17 v IL-23
#RNL26@RheumNow
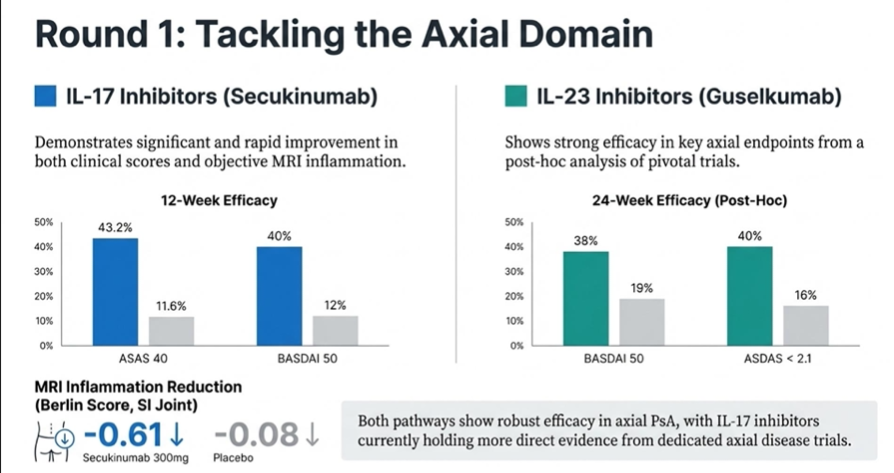
Axial domain- good IL-17 data as well IL-23 post-hoc data
Both show data of prevention of damage
Real-world data suggest IL-23 longer persistence
Safety: higher candidiasis and IBD risks w IL17
Dupilumab-associated arthritis
#RNL26@RheumNow
Onset wks to mos
Diffuse/symm jt pain
Trigger IL23/IL17 mediated inflamm MSK syndrome
Resolves with cessation of dupilumab, but can Rx through with NSAIDs, steroids, MTX, JAK
May have enthesitis/tenosynovitis/arthritis phenotype
2025 update of EULAR recommendations on lupus nephritis
At the 2025 EULAR congress in Barcelona, Prof Dimitrios Boumpas presented updated EULAR recommendations on managing lupus nephritis (LN). The key change is that the historic standard of care (mycophenolate with glucocorticoids) is now considered inferior to several licensed and unlicensed combination therapies.
https://t.co/wBsacwmqKA
Hydroxychloroquine for Everyone
Nearly 25 years ago, while lecturing on best therapies for rheumatoid arthritis (RA), I loudly stated that hydroxychloroquine was “useless” and, deservedly, I was “boo-ed” off stage. My point then was that rheumatologists needed to be aggressive, if not overly aggressive, in treating all RA patients. And my view was that HCQ was representative of under-treatment.
https://t.co/hNbPdPt9qG
Os dejamos este paper recién publicado 💪🏼 Este estudio concluye resultados muy relevantes para el manejo de pacientes con aortitis asociada en ACG 🫣
❌TCZ en monoterapia NO funciona
✅TCZ + MTX SÍ funciona
😍😍Click on "2025 Systemic Lupus Erythematosus Guidelines" here:
https://t.co/B4Gd6HexIe
@ACRheum@ACR_Journals
Some of my favs:
✅ Though they recommend SLEDAI for disease activity, they realistically acknowledge that many rheumatologists are WAY too busy to realistically measure it every visit.
✅ T2T is remission. They acknowledge that DORIS remission (a research tool) is the most widely used tool, but they note that T2T RCTs are needed.
😡I DO NOT like DORIS in clinical practice!! It allows patients on steroids. That is NOT remission. Remission should be no active inflammation clinically (SLEDAI, PGA, and BILAG = 0 and no steroids)!
✅ They give very nice, practical advice for general rheumatologists about some common manifestations, eg not over treating asx cytopenias, and how to treat leukocytoclastic vasculitis (don't 'over treat).
✅They recommend UV protection in ALL SLE patients. Though they did not state this, they are silently acknowledging that almost all SLE patients are UV sensitive even if they do not get photosensitive rashes.
✅ They recommend the use of quinacrine for CLE. To learn how to RX quinacrine, go to: https://t.co/L0sbLyJo5h
✅They recommend lenalidomide instead of the more dangerous thalidomide in severe CLE.
✅ Though the summary makes it sound like they recommend biologics "down the road" in lupus arthritis, thankfully, the manuscripts acknowledges that "there will be individuals for whom biologic therapy ... is preferable." We CANNOT allow some of our patients to progress to Jaccoud's. Rapid remission is important!
What I do not like:
✅ They recommend up to 1000 mg IV methylprednisolone. There is NO evidence that 1000 mg works better than 500 mg. However, retrospective studies show that 1000 mg is clearly associated with more severe infections! (see the studies referenced in Porta et al, link below).
✅ Unfortunately, they do not recommend using more high dose IV pulse methylprednisolone to take advantage of its safer and faster working non-genomic effects and its ability to greatly lower oral steroids faster. @eular_org and our European counterparts are way ahead of us on this one. Everyone should read https://t.co/hGf0Ixpj8Q
✅ For the zero steroids recommendation, they recommend within 6 months. That is TOO LONG for most patients. Use steroids per Porta et al, test HCQ drug levels every visit, start with combination tx immediately in moderate to severe SLE, and 5 mg is easily achievable much faster than 6 mo in the vast majority of SLE patients.
✅ So, so sad that they don't recommend HCQ drug levels. How much more evidence do you need? I can plop a huge pile of studies on your desks. Nathalie Costedoat-Chalumeau has been publishing convincing evidence since 2006. I've used them since 2016 (recommended by Michelle Petri) and it has GREATLY transformed my clinic into more remissions and markedly less steroids. Rheumatologists who are not using it every visit are missing poor adherence, and allowing patients a higher risk for retinopathy (too many with levels above 1200 ng/mL), and too many patients below the therapeutic goal of 750 ng/mL).
My final verdict: Over all... wonderful job Guidelines Committee!
Since this is a living document... please go back and add using HCQ drug levels!
It’s interview season! Here’s an article I wrote with advice for applicants, based on 15+ years of doing interviews at every level from med school to residency to fellowship. Give it a read and let me know what you think. https://t.co/97FBg96Xj0
FDA Approves Obinutuzumab for Active Lupus Nephritis
The FDA has approved obinutuzumab (Gazyva) for the treatment of lupus nephritis. This is good news for the more than 1.7 million people worldwide with lupus nephritis.
https://t.co/WbpATY86BY