@Jeff_Mans took a risk and snagged Spears, Boutte, Franklin, and Harvey to get me through the bye week. Appreciate your guidance and weekly rankings. Keep up the good work man
@RougeAnalyst@miljan0x Kompete is doing just fine. Even after declining to pay influencers to shill it. Still strong development team with an actual product you can play
After speaking with @JKOMPETE about #Kompete I am even more bullish than I previously was when I first looked into it
Very early on in the project but strong conviction
Building a monster game and platform.
Super impressed with what they have built so far
@KOMPETEgame
Just finished watching Dr. Carmody's YouTube videos. You can't find a better in depth analysis of the recent USMLE scandal—mathematically proven and so many of the questions are answered. They should make a documentary from this. @jbcarmody
This will shift the dominant application strategy from “Apply to as many programs as possible” to “How do I most effectively allocate my preference signals?”
Applicants who signal wisely will benefit… those who don’t will suffer.
More here:
https://t.co/UcIGLzbxU8
@mattdinniman new achievement! You tweeted at the author of your favorite book in a feeble attempt to join the closed kickstarter. Your rewaaaaard? Nothing! Like turning in late homework- you get the satisfaction that at least you tried (May I somehow still join?)
📄 20 studies that Internal Medicine Residents should read in the first year 👇
1/ 🏃♀️ RACE II trial: Lenient resting HR < 110 was non-inferior to a strict HR < 80 in patients with atrial fibrillation.
🧵
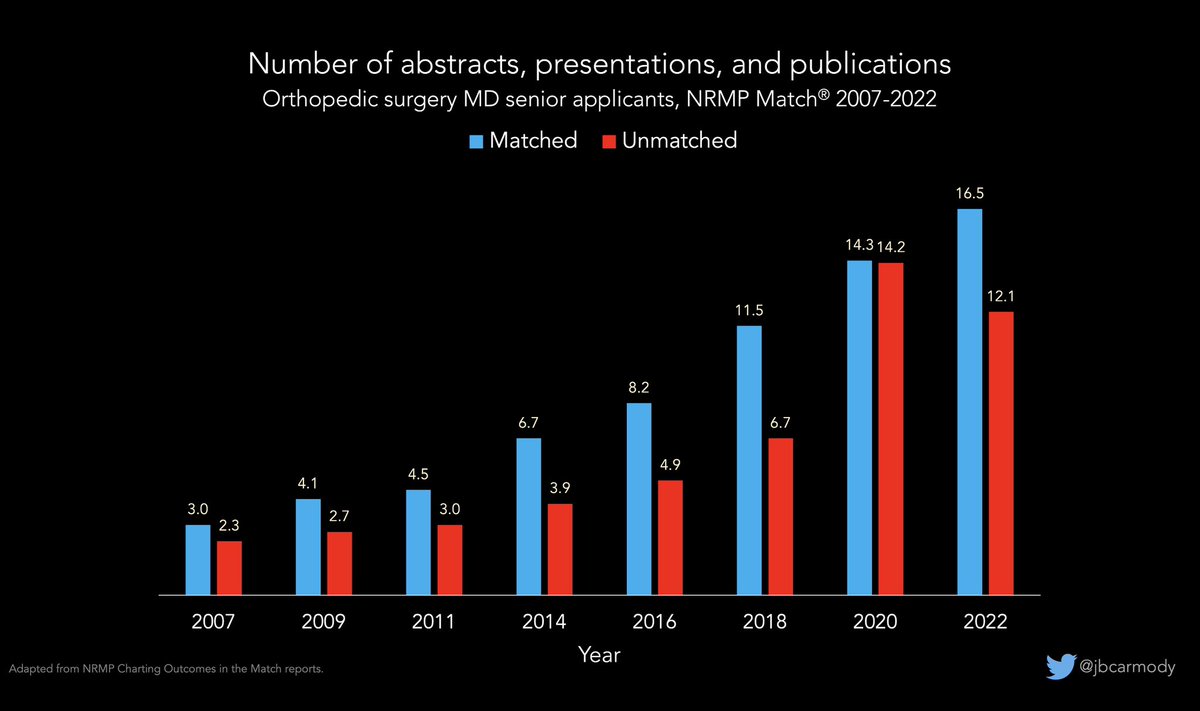
To me, what’s most striking is the increase in research output by *unmatched* applicants.
Today’s unsuccessful applicants are still do more research than successful applicants from even just a few years ago.
It’s an arms race, pure and simple.
e.g., for orthopedic surgery:
I delve into @doximity physician compensation data based on region, academia/private practice, yrs of experience, and most importantly comparing specialty to subspecialties in the US (cards vs international vs EP) and insight after 1 yr as an attending
I have had a lot of DMs
As way of context, a 🧵
1) Any health professional doing an invasive procedure should be able to deal with complications particularly life-threatening ones.
If they cant pt lives are put at risk
I trained full time for 3 yrs, did >1000 first opertor procedures as a trainee, to be able to undertake PCI. If there is coronary obstruction- the operator needs to be trained in PCI or the pt will die. You need to be able to do this in 1 or 2 minutes, same with pericardiocentesis. A nurse does not have the necessary training to deal with these complications, manage the pt pre and post procedure.
I'm a consultant interventionalist, but was a trainee just 18mo ago. I am an educational supervisor (to doctors) and have mentored ANPs & pharmacists to expand their skills. I am clinical lead for my department, so all too aware of the pressures on trusts. Here are my thoughts. https://t.co/NTtasXQiam