Until now, physicians using AI in clinic had to assemble the patient’s context themselves. Allergies, comorbidities, medications, prior procedures, copy-pasted in from the chart.
Today we’re announcing a partnership with @CedarsSinai. OpenEvidence now works directly inside Epic, drawing on the patient’s full record and interpreting the medical literature through the lens of that specific patient.
Cedars-Sinai is the first academic health system to deploy patient-aware clinical intelligence at enterprise scale. The clinician asks a complex question in natural language. The answer reflects both the best available evidence and the patient in front of them.
Patient data is never stored after the clinical session or used for any other purpose.
Oxford researchers just confirmed what we feared:
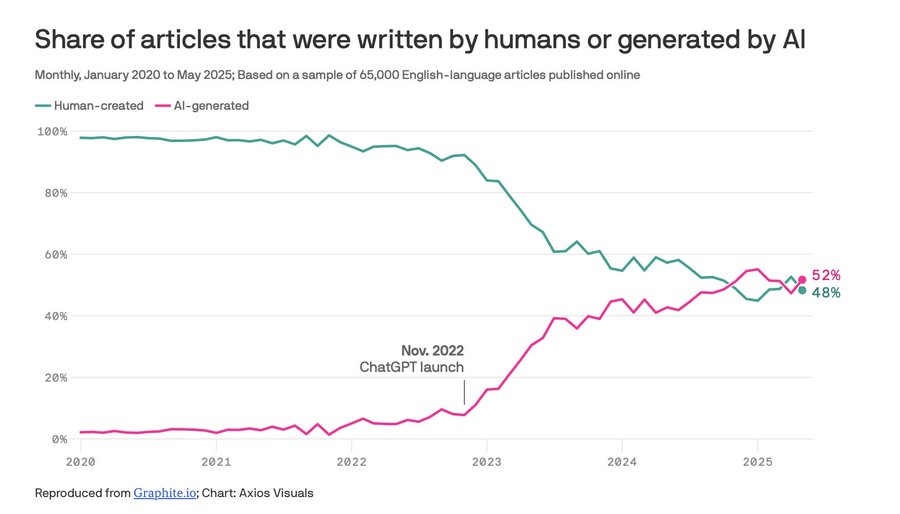
The internet as we knew it is dying.
AI content went from ~5% in 2020 to 48% by May 2025. Projections say 90%+ by next year.
Why? AI articles cost <$0.01. Human writers cost $10-100.
But the real crisis is model collapse. When AI trains on AI-generated content, quality degrades like photocopying a photocopy. Rare ideas disappear. Everything converges to generic sameness.
It's recursive. Today's AI slop becomes tomorrow's training data, producing worse output, which becomes training data again.
Do you ever feel that some cities are just more alive than others?
It's probably because they're "mixed-use".
This is a simple idea, but it changes everything...
We're too eager to bet on people who overestimate themselves—and too hesitant to invest in those who underestimate themselves.
It's easier to build up confidence than to tear down arrogance.
The people with the most potential are the ones who know they have a lot to learn.
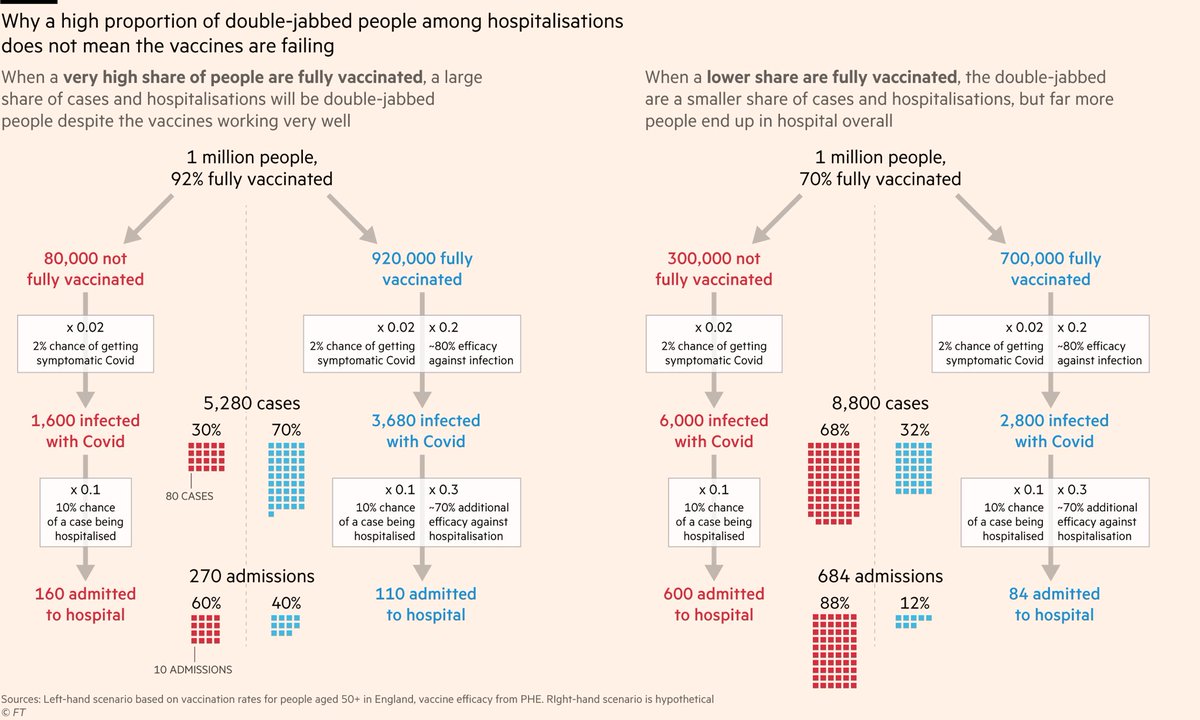
NEW: people worry when they hear "40% of hospitalisations are fully vaxxed", but this chart shows that's actually good news.
The more people you vaccinate, the higher their share of hospitalisations, but the *total* number in hospital is a fraction of what it would otherwise be