General Surgeon | Trauma | Academic Dept of Military Surgery & Trauma / Centre for Trauma Sciences | Decision Making BNs
Views my own, not those of my employer
Critical decision-making in trauma- Penetrating Thoraco-abdominal injury. Laparotomy or Thoracotomy?
Success relies not just on operative skill, but on strategic restraint-knowing that CT scans lie about the diaphragm, chest tubes lie about the source of blood, and that surviving the trauma requires deliberately identifying the true source of instability before making the first incision. @MaxMarsden83 #ASGBI2026
A study published today in Science may be the most important AI paper in clinical medicine this year. And it happened to land on the same day I submitted a letter to JAMA arguing that AI can already deliver clinically adequate care for defined tasks.
Researchers at Harvard Medical School and Beth Israel Deaconess Medical Center ran six experiments pitting OpenAI's o1 reasoning model against hundreds of physicians across the full spectrum of clinical reasoning: differential diagnosis, management planning, probabilistic reasoning, and clinical documentation. Then they did something most AI studies don't. They tested it on 76 real, unstructured emergency department cases pulled directly from the medical record at a major academic medical center.
The results across all six experiments: the AI outperformed physicians.
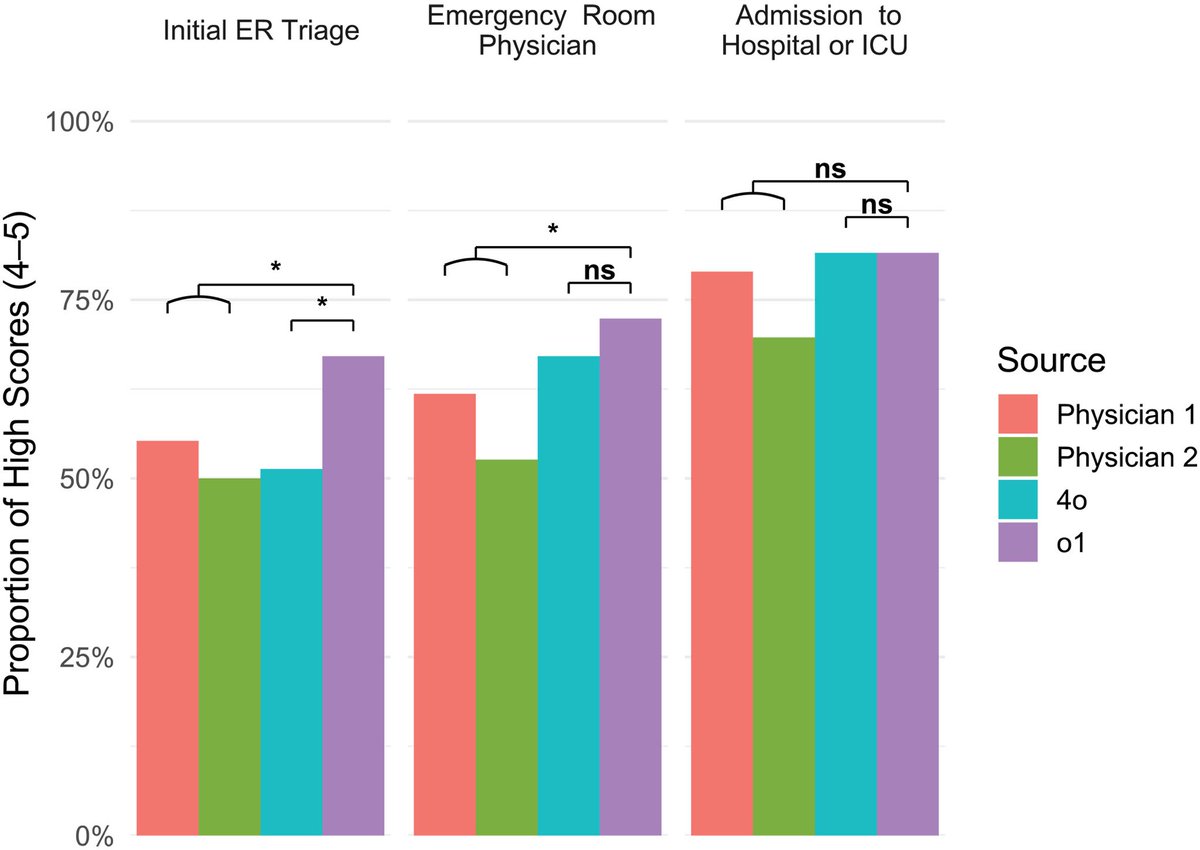
On the real ER cases — the messiest, most clinically relevant test — the AI identified the correct or very close diagnosis in 67.1% of cases at initial triage, 72.4% at ER physician evaluation, and 81.6% at hospital admission. The two attending physicians scored 55.3% and 50.0% at triage, 61.8% and 52.6% at ER evaluation, and 78.9% and 69.7% at admission. The gap was widest at initial triage.
On management reasoning using expert-scored clinical vignettes, the AI scored a median of 89%. Physicians with conventional resources scored 34%. That is not a typo.
The physician evaluators were blinded and could not distinguish AI-generated differentials from human ones. One evaluator guessed correctly 15% of the time. The other guessed correctly 3% of the time.
I'm an emergency physician. I work in a rural Texas ED. These are my cases. These are my decision points. And I can tell you that the triage finding is the one that matters most. Triage is where the least information meets the highest stakes — where the wrong call means a patient sits in the waiting room while their sepsis progresses or their STEMI evolves. The AI was 12 to 17 percentage points better than experienced attendings at exactly that moment.
The authors are careful to note this is text-based reasoning only; the AI doesn't see the patient's distress, doesn't hear breath sounds, doesn't read the room. Those are real limitations today. But the cognitive reasoning component of emergency medicine — pattern recognition under uncertainty with incomplete data — is precisely what this model is demonstrating it can do.
This was published in Science. Not a preprint. Not a company blog post. Peer-reviewed, in one of the two most prestigious scientific journals in the world.
The profession needs to stop debating whether AI will be good enough. It needs to start planning for the fact that, for an expanding set of clinical reasoning tasks, it already is.
And yes, this was written with AI. Sorry!!
@BehindTheKnife After years of listening to Behind the Knife—it even helped me pass my FRCS!—it was brilliant to finally contribute. Dive into London's trauma system management here: [https://t.co/WjBqr8YMhQ]
Juicy new CLINICAL CHALLENGES IN TRAUMA SURGERY ➡️ Stabbed in the Back - Decision Making in a Penetrating Junctional Vascular Injury🩸
Join our elite @LonTraumaSchool team @maxmarsden83 @cjaylwin for an engaging, high-yield conversation.
🎧https://t.co/uo18JYe5Xg🎧
@bonedocnavy@OxboneOrg Brilliant news well done.
I hope you mentioned at your final ARCP the ability to talk a stressed general surgeon through an axillary artery repair?
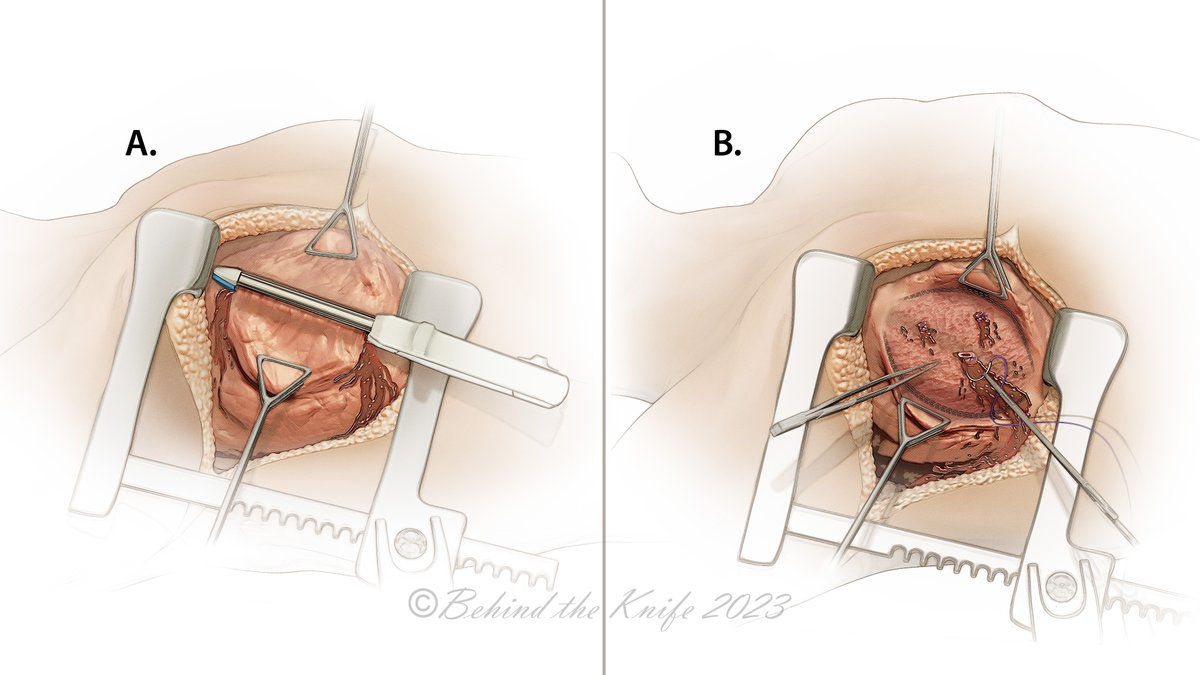
PENETRATING LUNG 🫁 INJURY?!
Rule of 👍🏼 ➡️ 1500 cc bloody drainage @ time of chest tube placement or > 200 cc/hr 🟰 OR. In reality, many factors go into this decision 🧠 , including stability, transfusion requirements/trend 📈, concomitant injuries, etc.
✔️ Quickest + safest approach for a TRAUMA patient is an anterolateral thoracotomy.
✔️ Small injuries can often be managed with suture repair alone.
✔️ Treat peripheral injuries with a non-anatomic stapled resection.
✔️ A pulmonary tractotomy can be used to expose deep injuries, allowing for repair.
✔️ Central 🫁 injuries are tough. Control the hilum with fingers, a clamp, or in extreme cases, hilar twist.
✔️ Total pneumonectomy is a last resort ➡️ mortality is ~50%
✔️ Repair the diaphragm primarily ➡️ use permanent suture & whatever technique works best.
Be sure to watch the high-yield @BehindTheKnife video in our Trauma Atlas: https://t.co/6cbVAgBGLy
I wasn’t there, but know that the role played by friends. colleagues, and people we don’t know, on 7/7 was extrordimary. There are amazing people in this world, with acts of kindness always outglowing the hate. 🙏🏼 for everyone who was affected, and who played a part to help.
@karimbrohi You didn’t just build a trauma system you set off a ripple effect that reshaped trauma care across the globe.
Thousands of lives saved thousands of learners taught! A model studied and copied.
Legends don’t step down. They leave shockwaves.
Respect, Karim 👊
An excellent turnout from @LeedsEGS at the @asgbi Gala Dinner last night! Superb location and excellent craic with a ceilidh to top things off! @abppc@josiewalshaw1
Hey, what do you think? IV or IO?
This video in our partnership with @DGlaucomflecken summarizes new research comparing initial attempts at intraosseous or intravenous vascular access in adults who had out-of-hospital cardiac arrest.
Full trial: https://t.co/Ha2o7JpnCX