It is your prerogative to decide what and how to communicate about your personal health situation. However, the underlying data is very much everybody's business.
Not everybody going on about ivermectin is 'shilling'. That said, I too am somewhat bewildered by the range of uses I see it promoted, and arguably shilled, for.
The use of ivermectin against Sars-CoV2 is not such a use. In my opinion, a competent honest scientific evaluation of the data results in the conclusion that it very much seems to be quite effective in preventing and treating Covid19.
A scientific establishment that misses or suppresses that warrants fear.
There are so many aspects to this:
'Yes, I had a very severe reaction to my second Moderna shot.'
Sounds like you became very ill shortly after taking this shot, and you concluded the illness was caused by Moderna. I am assuming you are likely right about this, however, the steps involved in reaching this conclusion are a worthwhile topic in itself.
'responsible scientist [..] not extrapolating'
I mostly disagree with that. This extrapolation is exactly what formal 'adverse event' monitoring is for. Apart from a formal setting, like a trial, informally, family doctors will do the same for their patients, people for their village or family, or even for themselves only, and they should.
This is not to say we should assume your reaction is something the whole population will experience, of course. It is however key data for calculating the risk for an individual. The data is of course incomplete for an quantified estimate, except for one: that the risk is greater than zero. For that last one, it suffices, and that is relevant to the general public.
'first mRNA vaccine [..] decision to avoid them'
I'd say it was your second, but possibly not at all the same one. In all fabrication processes, there is a spread for many characteristics of the end product. In case of these shots, the initial tests used a very different production process as was used for the general rollout. I think there are many indications that these later batches of Pfizer and Moderna had considerable differences between them, so, some batches may have been more dangerous or effective than others.
'irresponsible [..] telling millions of people online to not get vaccinated'
That, I agree with, at least on the basis of that experience alone. I think it is however another matter to be open about things like these and to let people reach their own conclusions about the risks and possible benefits involved.
Personal testimony, even a large collection of them, isn't a substitute for real, population-level data.
I get what you mean and don't want to be all too nit picky about it, but a large collection of personal testimonies IS a form of population level data. It is just, in many cases, like self report without careful sampling it is going be be skewed for the metric in question, like cost/benefit.
Windpark Goyerbrug UT,
Opvallend is dat sinds ons (noodsignaal) artikel in het AD en ons verzoek aan de gedeputeerde van de provincie Utrecht om de mega-windturbine die het dichtst bij onze woning staat (tijdelijk) buiten bedrijf te stellen, deze juist vaker lijkt te draaien.
We hebben sterk het gevoel dat we worden getreiterd.
@ProvUtrecht@gemHouten@HartvNL@SonjaAllachi@mariannezw@RPlasterk@ClintelNED@ElzevH
The totality of evidence of ivermectin working against SARS-CoV2 is in fact overwhelming.
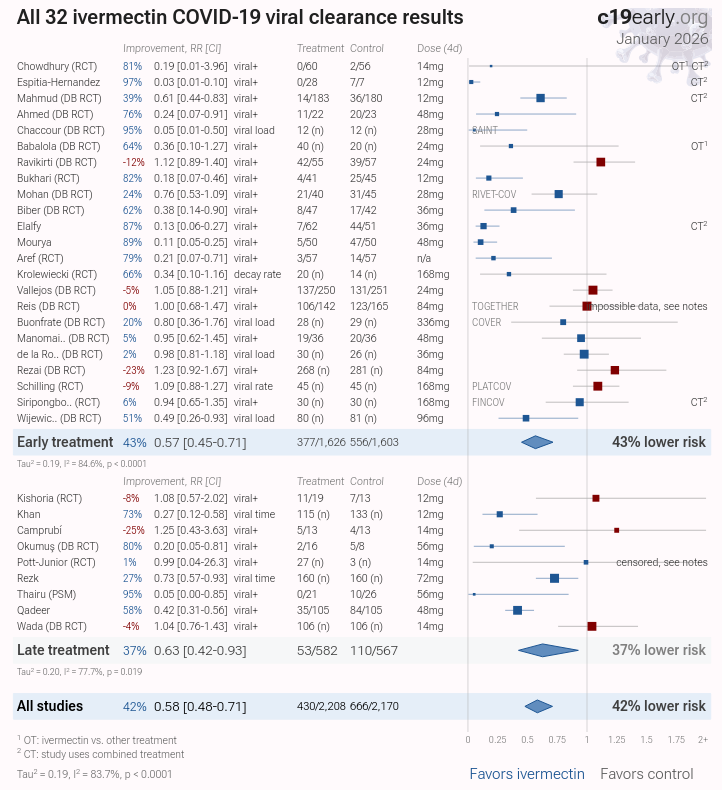
Below I have posted a forest plot of viral clearance and viral load results from Januari this year. The trend of this meta analysis is very clear, 15 of the 32 trials are full on significant, one more (Krolewiecki) is significant on re analysis where it even hits .99. TOGETHER, while showing up as a negative result on this plot, should in fact be positive result if one looks at what actually happened here (the 3 day result is meaningless as there is no base line measurement, but the trend between 3 and 7 days strongly favors ivermectin).
If one believes that SARS-CoV2 causes Covid19, and that viral load is positively correlated with disease severity, these results alone are strong evidence of efficacy.
But we can look further, say at the four largest (non prophylaxis) RCT's. These are TOGETHER, ACTIVE-6 low dose, Active-6 high dose, and PRINCIPLE. IN ALL these trials recovery was faster for the treatment group, sometimes significantly so.
Overall, the other results of these trials favor ivermectin, even if they fall short of significance (including mortality). Some endpoints of course do not, this is almost always the case, even for medications that work (i.e. the negative signal for the WHO compound clinical improvement scale results in ACTIVE HD, which stink to high heaven, and the meaningless low event results of the clinical endpoints in PRINCIPLE).
Despite the fact that in these large 'high quality and rigorous' (hah!) trials the ivermectin was only given roughly 3-14 days after first symptoms, which is really much too late for an antiviral to be maximally effective. It is ridiculous. THIS is why the large RCTs had mediocre, if still positive, outcomes for the drug. It was not because the drug did not work well.
So these large RCT's actually align with the positive evidence from the antiviral results, as do the trends in the smaller RCT's, and non RCT trials.
All of this can be found on C19early dot org, the better systematic analysis (not Cochrane).
It is funny how many places are portrayed as the true spiritual centers of Christianity. From Jerusalem to Rome, to Constantinople, to Athos, to Moscow, to Joseph of Arimathea bringing the Holy Grail to Glastonbury, or the puritans founding their City on the Hill as a Christian beacon, in America.
While the real successors are, of course, the Mormons in Salt Lake City. Take that, Dugin.
@ufmasters@CassieWats86780@ValerieAnne1970 Or, you could also genuinely look at my earlier reply with the screenshot of the actual tables in the research papers. I'm not saying it is easy to read this, it is not, but it is doable. The AI summary is wrong on 2 counts, and missed the key information on the 3rd.
Because it is in fact the right conclusion based on the available data. Grok is not correct here.
In TOGETHER, the results were in favor of ivermectin across the board. Grok, and other AI's, continue to interpret the results that in fact signaled moderate benefit for ivermectin in TOGETHER, just not at the traditional 0.95 threshold, as evidence for no benefit. In TOGETHER, hospitalizations were reduced by about 20%, (the 'primary endpoint').
Something similar happened for ACTIVE low dose, the third of the very large trials (of those, only ACTIVE HIGH dose was not a clear signal FOR efficacy of ivermectin).
In PRINCIPLE, for the primary endpoint of recovery, the patients that received ivermectin did in fact recover faster (and it met the 0.95 threshold). The researchers however had set a threshold that the difference should be a certain minimum, otherwise 'it does not count'.
The reason that the results for ivermectin were not stronger than they were in these trials appears to be very clear: it was given too late. Ivermectin was being evaluated as an 'antiviral', a drug that stops the viral replication. Those work if they are given early enough, ideally BEFORE a person gets sick, OR at first symptoms. If you wait after that, it is less effective.
In the 'large, rigorous' the patients were first tested for virus, then randomized, then the ivermectin was sent to them, anywhere from 3 to 14 days (!!) after first symptoms. While even 3 days after first symptoms is still categorized as 'early treatment' of Covid, it is NOT early treatment as far as antivirals go. The viral replication is already slowing down by itself at this point.
While the importance of early application of antivirals is well understood, and was extensively discussed in for example the a video presentation by dr Mills, one of the researchers in TOGETHER on their own website, I think none of the final publications payed a lot (if any) attention to the fact administration of ivermectin in these trials was not optimal because it was just too late for that, even at 3 days after first symptoms, let alone longer delays, up to 14 days.
And that alone refutes any claim that these trials were 'rigorous'. They were not.
The person I responded to did use Grok. The answer to that person is sufficiently relevant to your post to link it.
But I can go over your points too. I provide screen shots from the publications and a meta analysis. Look at them for yourself!
Lets start with PRINCIPLE, table 2. 15% faster recovery in the ivermectin patient p > 0.999 ! That sure is some way to conclusively show the drug does not speed up recovery! It is especially remarkable that they gave ivermectin up to like 18 days after infection.
In TOGETHER, table 3, hospitalizations for the ivermectin group were 17% lower. Deaths in the ivermectin group were 12% lower.
Your AI, whichever one it was, was wrong about these two trials. Just plain old wrong.
About antivirality: the fact that, in vitro, toxic concentrations amounts were used for an antiviral mechanism means nothing about the antiviral effects at safe doses for humans. Could work, could not work.
But do we have information about antiviral activity in patient populations? Well, yes we do: viral clearance and viral load data, forest plot linked. This meta analysis shows overwhelming evidence for an antiviral activity, the trend is strong in that direction. 15 out of 32 trials are full on significant. Additionally, Krolewiecki in re analysis actually hits a .99 threshold, and if we look at the antiviral results for TOGETHER, we see that that is actually evidence for an antiviral effect too. (The issue here is they established no base line).
Because it is in fact the right conclusion based on the available data. Grok is not correct here.
In TOGETHER, the results were in favor of ivermectin across the board. Grok, and other AI's, continue to interpret the results that in fact signaled moderate benefit for ivermectin in TOGETHER, just not at the traditional 0.95 threshold, as evidence for no benefit. In TOGETHER, hospitalizations were reduced by about 20%, (the 'primary endpoint').
Something similar happened for ACTIVE low dose, the third of the very large trials (of those, only ACTIVE HIGH dose was not a clear signal FOR efficacy of ivermectin).
In PRINCIPLE, for the primary endpoint of recovery, the patients that received ivermectin did in fact recover faster (and it met the 0.95 threshold). The researchers however had set a threshold that the difference should be a certain minimum, otherwise 'it does not count'.
The reason that the results for ivermectin were not stronger than they were in these trials appears to be very clear: it was given too late. Ivermectin was being evaluated as an 'antiviral', a drug that stops the viral replication. Those work if they are given early enough, ideally BEFORE a person gets sick, OR at first symptoms. If you wait after that, it is less effective.
In the 'large, rigorous' the patients were first tested for virus, then randomized, then the ivermectin was sent to them, anywhere from 3 to 14 days (!!) after first symptoms. While even 3 days after first symptoms is still categorized as 'early treatment' of Covid, it is NOT early treatment as far as antivirals go. The viral replication is already slowing down by itself at this point.
While the importance of early application of antivirals is well understood, and was extensively discussed in for example the a video presentation by dr Mills, one of the researchers in TOGETHER on their own website, I think none of the final publications payed a lot (if any) attention to the fact administration of ivermectin in these trials was not optimal because it was just too late for that, even at 3 days after first symptoms, let alone longer delays, up to 14 days.
And that alone refutes any claim that these trials were 'rigorous'. They were not.
@pbcoppola@ValerieAnne1970 TOGETHER, ACTIVE, and PRINCIPLE all actually showed signal for a moderate benefit of ivermectin against SARS-CoV2. Some of it 'significant' too.
The main reason the benefit was not much larger was that ivermectin was given late to ridiculously late in these trials.
There is no short way to explain this, and one will encounter many skilled people making cases against my following statement, but the reality is this: the totality of evidence for ivermectin working against SARS-CoV2 is overwhelming.
The best meta analysis about it is from C19early dot org, not anything published in the major papers. Yes, it is easy to find opportunistic reasons to critique that meta analysis, but most of them do not hold on careful examination.
I do have a (relatively solid) background in this kind of research, and I have thought long and hard about the ivermectin data, and the methods of C19early (like, half a year full time maybe). It is not a trivial thing to do, not even with previous training. But the overwhelming results are really all there, if one actually looks at it after that.