@amyfaithho Thank you for your post. @PNHP is trying to create a win-win health system in which patients and clinicians benefit. https://t.co/iHCe51Xw3T
What an absolutely amazing experience to collaborate with such a brilliant, engaged, and innovative group of scientists focused on addressing the crippling toll of prolonged organ recovery from sepsis! @SepsisAlliance
@msiuba I agree that we need to move on from midodrine/octreotide. MAP matters, and, from a vasopressor perspective, I think angiotensin 2 warrants formal assessment (https://t.co/IE6inf5rl0), esp compared to vaso/terlipressin (https://t.co/CFEjkLnR3v).
@lucey_mark@RAmirahmadi@epi_noel@EMNerd_ That’s great! The platelet count never stopped me from placing lines, but we wanted to provide objective data to support what we know makes sense in many situations.
@PulmCrit If people feel inclined to pursue an RCT to further solidify the argument, hopefully we’ve at least laid the groundwork to justify one. Even if there were a mild increase in bleeding (there wasn’t), I’d prefer a bandage over a hematological tissue transplant.
@PulmCrit The technique & skill level of the CVC inserter tends to better dictate bleeding complication risk than a patient’s clotting defects. Changing hospital policy to a 10k threshold required a lot of negotiation, making studying lower thresholds difficult.
This study highlights the safety of placing PICCs in severely thrombocytopenic patients without prophylactic platelet administration, which can save thousands of blood products annually. Great work from a team willing to rethink the status quo — congratulations, crew!
Our paper just published in Annals of Hematology showed lowering PICC insertion platelet requirement from 50K to 10K resulted in less prophylactic platelet & total blood transfusions with no difference in PICC bleeding
https://t.co/LENXJc1oSF
@epi_noel@MikeMcCurdyMD@EMNerd_
My heart breaks knowing that my friends & colleagues at St. Luc & St. Damien Hospitals in Port-au-Prince, Haiti, are experiencing the kidnapping of one of their own. 😢
The St Luc Foundation and St Damien Hospital of NPFS decide to close the activities of St Damien and St LUc Hospitals until further notice following the kidnapping of Dr.Benetty Augustin.
Regardless of the issue at hand, standing by what’s right and supporting people of ALL backgrounds and walks of life who are trying to make the best of their circumstances is ALWAYS the right move. This ND grad nicely summarizes these points…
Senator Lana Theis accused me by name of grooming and sexualizing children in an attempt to marginalize me for standing up against her marginalizing the LGBTQ community...in a fundraising email, for herself.
Hate wins when people like me stand by and let it happen. I won't.
@MalloryMcMorrow Regardless of the issue at hand, standing by what’s right and supporting people of ALL backgrounds and walks of life who are trying to make the best of their circumstances is ALWAYS the right move. This ND grad nicely summarizes these points…
For years, we’ve advocated multimodal therapies in practically every other pathophysiological state (including HYPERtension); it’s surely time to acknowledge that the acutely deadly state of vasodilatory shock warrants a similar approach!
@KhannaAshishCCM@pwierusz @JonathanChowMD @LaurenceBusse @MMazzeffi @BellomoRinaldo Who knows the meaning, right (retrospective, etc)?… What I am pretty confident about, though, is that relegating even an optimal intervention to salvage therapy for a deadly disease & expecting it to meaningfully improve mortality is magical thinking. 🤷♂️
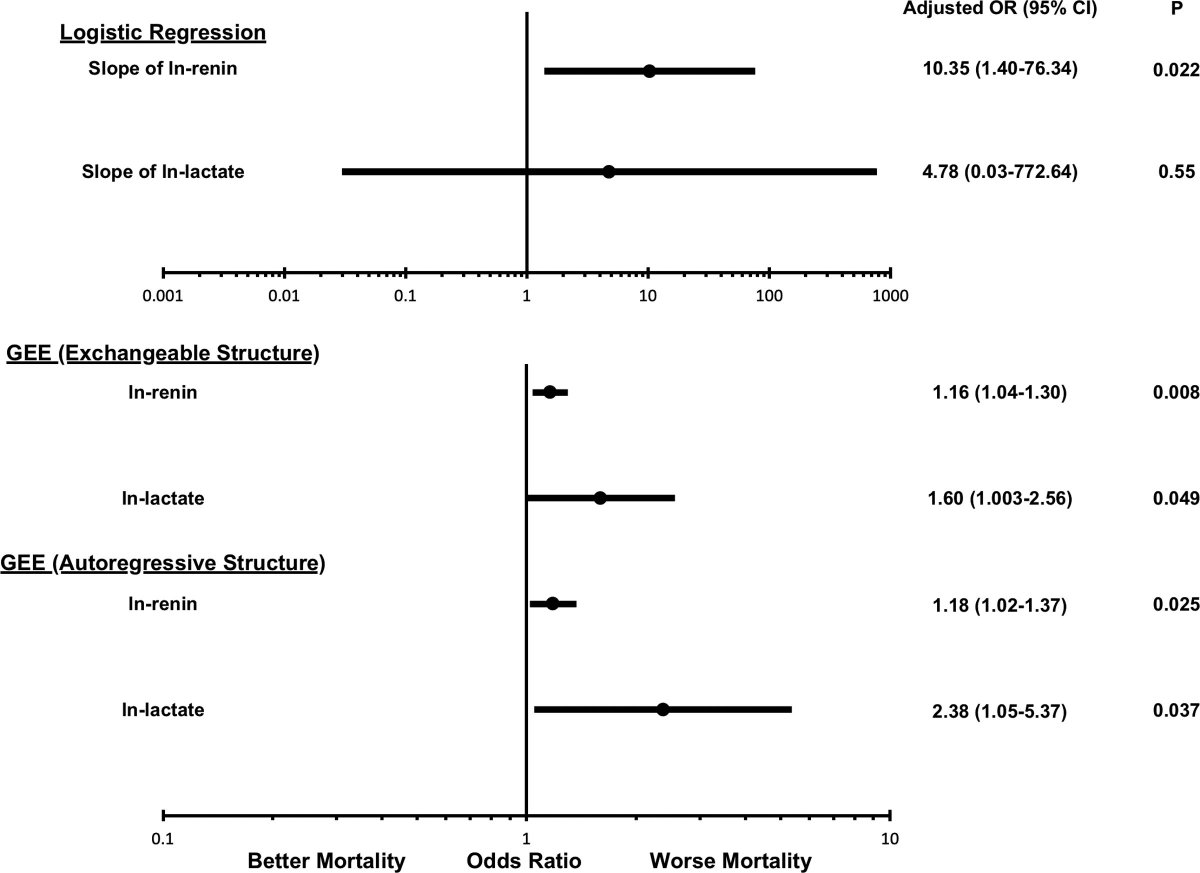
Not only does renin appear to outperform lactate in predicting mortality, selective angiotensin II therapy may improve mortality when renin levels are high (https://t.co/gxR0J8g60j). A ray of hope in personalized vasopressor therapy.
Jeyaraju et al : Renin Kinetics Superior to Lactate Kinetics for Predicting In-Hosp Mortality in Hypotensive #adultICU pts
Link: https://t.co/soAMjqN3Ol
Editorial: https://t.co/CMRT2TzjjB
#CritCareMed@SCCM @JonathanChowMD @KhannaAshishCCM
Fig: Forest plot aOR #mortality
It’s official — I am excited to announce that I have started a new position as the Chief Medical Officer of BOA Biomedical to pursue innovative diagnostic & therapeutic solutions to sepsis!
BOA Biomedical is excited to announce the appointment of Michael McCurdy, MD, FAAEM, FCCM to the position of Chief Medical Officer. We look forward to Dr. McCurdy’s leadership as BOA continues product development and clinical trials in our fight against infectious disease.