An incredible individual once told me to think of the healing journey like an 100-point exam.
For the sake of the analogy, let’s say there are 4 sections worth 25 points each.
Real life is obviously more complex than this, but this is a helpful way to think if you feel stuck.
A lot of people talk about carbs like the conversation ends at the glucose curve.
But once glucose gets into the cell and moves through glycolysis, the carbon still has a major decision point. Pyruvate can move toward lactate, alanine, glucose production in certain contexts, or mitochondrial oxidation.
The major gate into that last pathway is pyruvate dehydrogenase (PDH).
PDH converts pyruvate into acetyl-CoA, which allows carb-derived carbon to enter the TCA cycle. This is one reason “carb tolerance” is not only a blood sugar conversation, but also a mitochondrial entry conversation.
The PDH complex is a multi-enzyme system that needs specific nutrient-derived cofactors to do the chemistry:
- Thiamine, B1, as TPP for the decarboxylation step
- Magnesium to support the TPP-dependent E1 step
- Lipoic acid, as lipoamide, to carry the acetyl group
- Pantothenic acid, B5, to make CoA and form acetyl-CoA
- Riboflavin, B2, as FAD for the E3 redox step
- Niacin, B3, as NAD+, to accept electrons and form NADH
This does not mean every person with poor carb tolerance needs to slam B vitamins. That is where people oversimplify things. Food exists for a reason. But if you have tons of intolerances, supplementation could be smart.
PDH is also regulated by the state of the cell.
High NADH, high acetyl-CoA, high ATP, fasting physiology, stress chemistry, low oxygen availability, poor mitochondrial demand, and inactivity can all change how pyruvate is handled.
In that context, carbs may get broken down through glycolysis, but the system may not be as ready to move pyruvate through PDH and into the TCA cycle. More pyruvate can then be pushed toward lactate instead of being efficiently oxidized.
That is why two people can eat the same carb and have completely different responses.
One person feels warm, calm, fueled, and stable.
Another person feels heavy, sleepy, wired, craving-driven, or notices poor exercise tolerance when they try to increase carbs.
The food matters, but the pathway receiving the food matters too.
If carbohydrates are going to become mitochondrial energy, they have to pass through the pyruvate dehydrogenase checkpoint.
So when someone says they “do not tolerate carbs,” it's often useful to know more than just the carb source.
Otherwise, the conversation gets stuck at blood sugar when the bottleneck may be deeper.
“What did you do to heal?”
This is a question I receive at least 10 times a day…
While it’s a valid question for someone to ask at the beginning of their journey, it may not be the RIGHT question…
Let me explain.
For many chronic conditions, symptoms overlap. On top of that, you can have two people with the same “diagnosis” for two completely different reasons
I’ll give you a personal example:
I was diagnosed with Hashimotos Thyroiditis & TSHDS small fiber neuropathy
Conventional medicine will look at these conditions, their subset of your symptoms and then prescribe you thyroid medication and some form of pain medication to manage them
This template will be applied to every patient with these conditions and subset of symptoms
BUT THIS ISN’T HEALING
NEITHER IS “ROOT CAUSE”
Many people (including myself) will spend months or even years tweedling their thumbs, obsessing on labels, symptoms and root cause - when fundamentally they aren’t asking the first question 👇
“What areas of my weakened physiology lead to this cascade within the whole system in the first place”
When you’re going through a multi systemic disease process - it isn’t about a single variable or pathway
The real investigation begins when you start looking at the individual as a WHOLE, understand their unique background, environment, life events and piece together each area of their physiological development
The Nervous System 👉 Their Light & NnEMF Environment 👉 Nutritional Status 👉 Gut Health 👉 Immune modulation 👉 Mitochondrial efficiency 👉 ETC…
This is why so many “protocols” fail, because they fail to address YOU as the ENTIRE person you are from the get go
When my team works with someone we piece together the patterns from all of these areas of physiology, not blinding ourselves to one silo or another
Begin to change the questions you ask and watch the answers present themselves
Blueberries are one of the easiest foods to underestimate because they look too simple.
But when you look at human trials, you will slowly start to realize that all of the hype is real:
- They support blood vessel function
- They may improve post-meal glucose and insulin handling
- They may help cognitive performance when the brain is under metabolic strain
- They can influence immune-cell oxidative stress
- They may shift inflammatory cleanup signals after exercise
- They feed gut-derived metabolites that talk to the rest of the body
It's officially blueberry maxxxxxing summer.
Blueberries are one of the easiest foods to underestimate because they look too simple.
But when you look at human trials, you will slowly start to realize that all of the hype is real:
- They support blood vessel function
- They may improve post-meal glucose and insulin handling
- They may help cognitive performance when the brain is under metabolic strain
- They can influence immune-cell oxidative stress
- They may shift inflammatory cleanup signals after exercise
- They feed gut-derived metabolites that talk to the rest of the body
It's officially blueberry maxxxxxing summer.
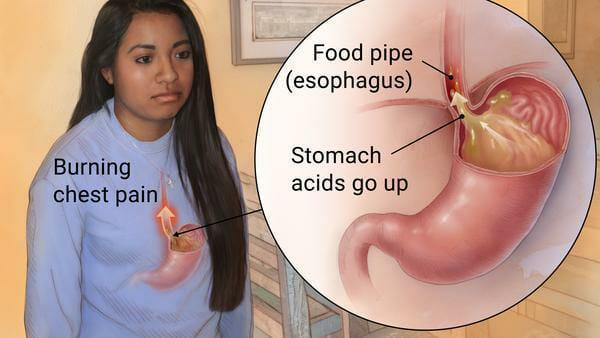
I know what it’s like to have reflux so bad that food feels like a problem.
And one thing I wish more people understood is this:
Reflux is not always solved by throwing one acid-related answer at it.
Some people need a deeper digestive context, such as stress, motility, meal timing, constipation, food tolerance, sleep, medication history, and what changed before the symptoms started.
If someone came to me with reflux, fatigue, and constipation, I’d want to know:
- Are they eating enough?
- Are they having daily bowel movements?
- Are they relying on antacids?
- Do they have undigested food in stool?
- Do they notice a "full" type of bloating?
- Is it tough to digest meat?
- Do they respond well or poorly to acidic foods?
- Do they notice lots of belching?
- Do they have a hiatal hernia?
And even then... I'm sure I would have many other questions!
The real work when looking at something tricky starts with pattern recognition over guessing every time.
I know what it’s like to have reflux so bad that food feels like a problem.
And one thing I wish more people understood is this:
Reflux is not always solved by throwing one acid-related answer at it.
Some people need a deeper digestive context, such as stress, motility, meal timing, constipation, food tolerance, sleep, medication history, and what changed before the symptoms started.
If someone came to me with reflux, fatigue, and constipation, I’d want to know:
- Are they eating enough?
- Are they having daily bowel movements?
- Are they relying on antacids?
- Do they have undigested food in stool?
- Do they notice a "full" type of bloating?
- Is it tough to digest meat?
- Do they respond well or poorly to acidic foods?
- Do they notice lots of belching?
- Do they have a hiatal hernia?
And even then... I'm sure I would have many other questions!
The real work when looking at something tricky starts with pattern recognition over guessing every time.
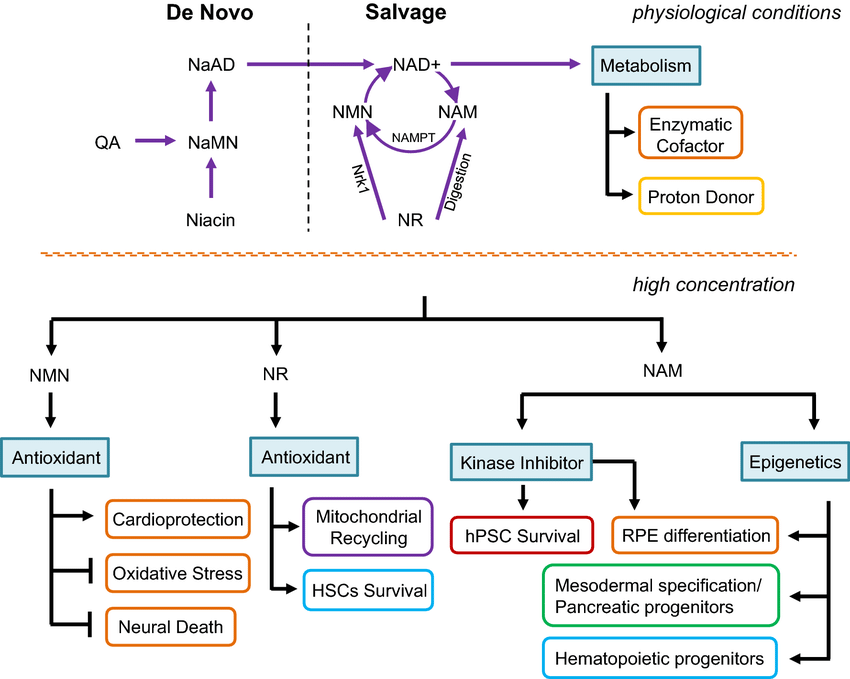
Vitamin B3 is one of the key nutrients your body uses to build NAD+.
B3/niacin exists in forms like nicotinic acid, nicotinamide, and nicotinamide riboside. Once absorbed, the body can convert niacin into NAD+, and NAD+ becomes one of the major coenzymes your cells use to run metabolism.
This matters because NAD+ helps the body turn carbohydrates, fats, and proteins into usable energy. It supports mitochondrial ATP production, DNA repair, sirtuin activity, cellular communication, and redox balance through NAD/NADH and NADP/NADPH.
So when someone says they are working on “mitochondrial health,” “cellular repair,” or “low energy,” B3 status may actually be worth checking.
Especially when the pattern looks like:
- Low overall B-vitamin intake
- Low protein or poor tryptophan status
- Gut issues or poor absorption
- Heavy alcohol burden
- Low Vitamin B2, Vitamin B6
- An advanced supplement protocol that skips basic nutritional status
That does not mean everyone is B3 deficient, and high-dose niacin is not automatically the answer. Dose, form, liver health, blood sugar, medications, and individual context all matter.
The NAD+ conversation got too obsessed with longevity marketing and forgot the basic nutrient piece.
Vitamin B3 matters because NAD+ matters for energy, repair, and resilience.
Vitamin B3 is one of the key nutrients your body uses to build NAD+.
B3/niacin exists in forms like nicotinic acid, nicotinamide, and nicotinamide riboside. Once absorbed, the body can convert niacin into NAD+, and NAD+ becomes one of the major coenzymes your cells use to run metabolism.
This matters because NAD+ helps the body turn carbohydrates, fats, and proteins into usable energy. It supports mitochondrial ATP production, DNA repair, sirtuin activity, cellular communication, and redox balance through NAD/NADH and NADP/NADPH.
So when someone says they are working on “mitochondrial health,” “cellular repair,” or “low energy,” B3 status may actually be worth checking.
Especially when the pattern looks like:
- Low overall B-vitamin intake
- Low protein or poor tryptophan status
- Gut issues or poor absorption
- Heavy alcohol burden
- Low Vitamin B2, Vitamin B6
- An advanced supplement protocol that skips basic nutritional status
That does not mean everyone is B3 deficient, and high-dose niacin is not automatically the answer. Dose, form, liver health, blood sugar, medications, and individual context all matter.
The NAD+ conversation got too obsessed with longevity marketing and forgot the basic nutrient piece.
Vitamin B3 matters because NAD+ matters for energy, repair, and resilience.
@NoahRyanCo Adopting a courage based mindset rather than a fear based one was hands down the best thing I’ve ever done for my focus.
The process of getting there though was slow and felt like making a sculpture
UNDERSTAND THIS HARD TRUTH:
Most who become chronically ill did so because of their own faulty decision making.
Be aware your mind might have remnants of this thinking.
Very few are willing to contend with that level of ego integration though.
Inflammation has a receipt.
Every time the immune system stays active, the body has to pay for that activity somehow.
In an acute infection, that makes sense. You feel heavy, foggy, sore, sleepy, and less interested in food or movement because the body is reallocating resources toward defense, repair, and containment.
That response can be useful when it has a beginning, a purpose, and an endpoint. The fatigue during a short illness is part of a coordinated shift in behavior and metabolism that helps the body deal with a threat.
The problem is when the immune system keeps getting pulled back into that state without a clean resolution.
The signal may be quieter than an acute infection, but it can still change how energy is used.
Low-grade inflammation can push cells toward faster, less efficient energy production, increase oxidative pressure, interfere with glucose handling, disturb sleep and circadian rhythm, and keep the brain receiving messages that something is still wrong.
That is one reason chronic fatigue can feel so irrational from the outside. The person may be eating, sleeping, resting, and trying to rebuild, but their body is still behaving like energy needs to be guarded, redirected, or spent on internal defense.
This is also where dysfunctional immune patterns become so important to be aware of.
A system dealing with chronic gut inflammation, unresolved infection signals, autoimmunity, mast cell activation, tissue injury, poor inflammatory resolution, or repeated stress chemistry may keep spending energy in the background.
Not always in a dramatic way. Think of it more like a slow leak.
The person does not wake up feeling like they fought a war because they are weak. They may wake up feeling that way because part of their physiology keeps acting like there is still something to fight, repair, contain, or monitor.
Inflammation can also change the relationship between the immune system and the brain.
In chronic inflammatory states, researchers have described a kind of competition for energy-rich substrates between the immune system and the brain.
So when someone has chronic fatigue, I do not only want to know how much energy they are making. I want to know where that energy is going.
Is the body using it to build, repair, think, move, digest, and recover? Or is too much of it being pulled into immune activation, inflammatory signaling, oxidative stress management, and damage control?
That question changes the way fatigue is understood.
Sometimes the issue is not that the person needs to force more output.
Sometimes the system needs fewer reasons to keep spending energy on protection.
Inflammation has a receipt.
Every time the immune system stays active, the body has to pay for that activity somehow.
In an acute infection, that makes sense. You feel heavy, foggy, sore, sleepy, and less interested in food or movement because the body is reallocating resources toward defense, repair, and containment.
That response can be useful when it has a beginning, a purpose, and an endpoint. The fatigue during a short illness is part of a coordinated shift in behavior and metabolism that helps the body deal with a threat.
The problem is when the immune system keeps getting pulled back into that state without a clean resolution.
The signal may be quieter than an acute infection, but it can still change how energy is used.
Low-grade inflammation can push cells toward faster, less efficient energy production, increase oxidative pressure, interfere with glucose handling, disturb sleep and circadian rhythm, and keep the brain receiving messages that something is still wrong.
That is one reason chronic fatigue can feel so irrational from the outside. The person may be eating, sleeping, resting, and trying to rebuild, but their body is still behaving like energy needs to be guarded, redirected, or spent on internal defense.
This is also where dysfunctional immune patterns become so important to be aware of.
A system dealing with chronic gut inflammation, unresolved infection signals, autoimmunity, mast cell activation, tissue injury, poor inflammatory resolution, or repeated stress chemistry may keep spending energy in the background.
Not always in a dramatic way. Think of it more like a slow leak.
The person does not wake up feeling like they fought a war because they are weak. They may wake up feeling that way because part of their physiology keeps acting like there is still something to fight, repair, contain, or monitor.
Inflammation can also change the relationship between the immune system and the brain.
In chronic inflammatory states, researchers have described a kind of competition for energy-rich substrates between the immune system and the brain.
So when someone has chronic fatigue, I do not only want to know how much energy they are making. I want to know where that energy is going.
Is the body using it to build, repair, think, move, digest, and recover? Or is too much of it being pulled into immune activation, inflammatory signaling, oxidative stress management, and damage control?
That question changes the way fatigue is understood.
Sometimes the issue is not that the person needs to force more output.
Sometimes the system needs fewer reasons to keep spending energy on protection.
An incredible individual once told me to think of the healing journey like an 100-point exam.
For the sake of the analogy, let’s say there are 4 sections worth 25 points each.
Real life is obviously more complex than this, but this is a helpful way to think if you feel stuck.